📋 Key Information Summary
- Colorectal cancer (CRC) is the second most common cancer in Australia; the National Bowel Cancer Screening Program (NBCSP) provides free faecal immunochemical test (FIT) kits every 2 years to eligible Australians aged 50–74.
- Average-risk individuals should commence structured screening at age 50 with biennial FIT via the NBCSP; emerging guidelines (USPSTF 2021, ACS) support initiating discussion from age 45.
- Increased-risk groups — first-degree relative (FDR) with CRC, hereditary syndromes (Lynch, FAP), inflammatory bowel disease (IBD), prior adenomas — require earlier and more intensive surveillance with colonoscopy.
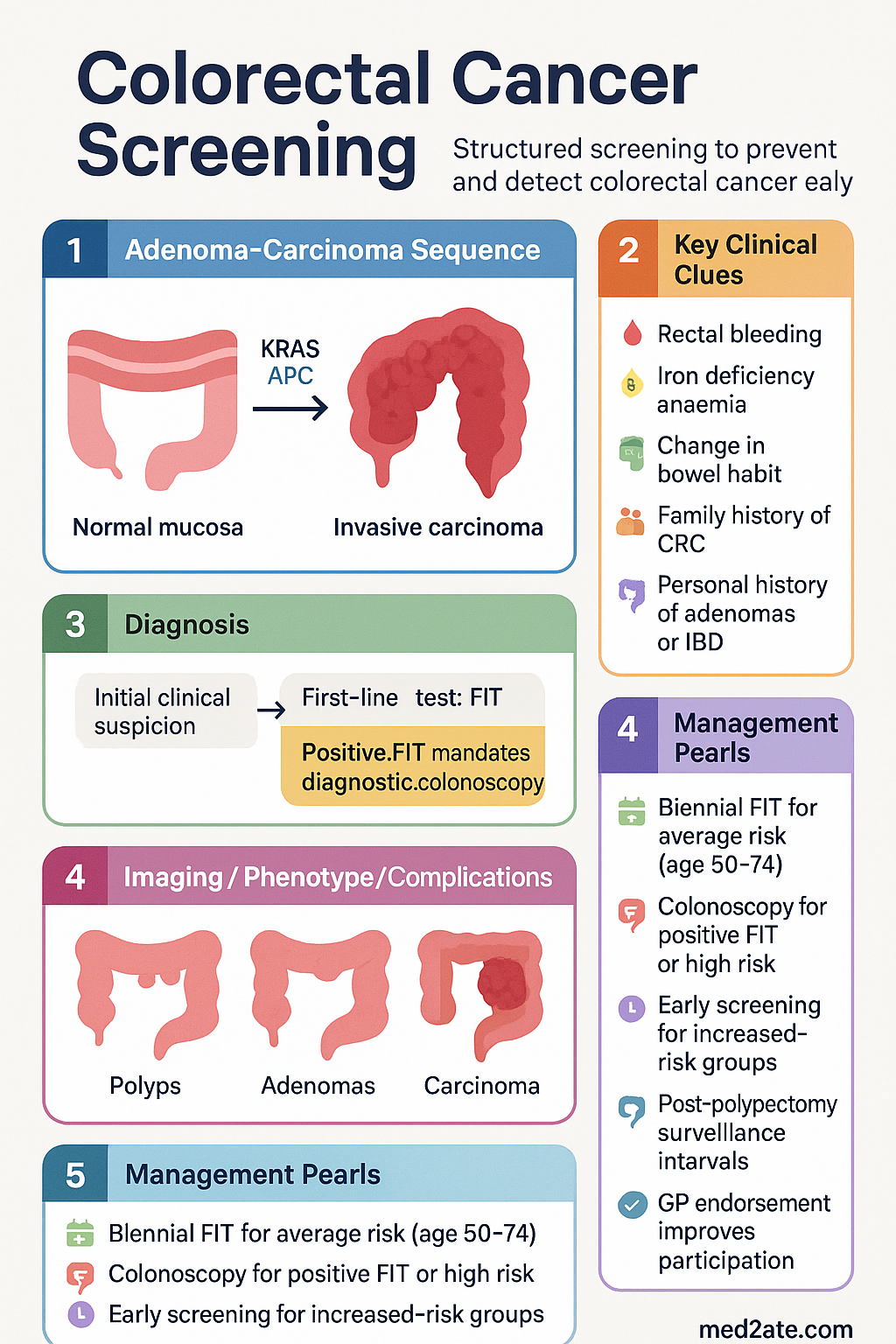
- FIT is the recommended primary screening modality for average-risk populations due to its sensitivity, non-invasiveness, and cost-effectiveness; a positive FIT mandates diagnostic colonoscopy.
- Colonoscopy remains the gold-standard diagnostic and therapeutic investigation; it enables polypectomy and histological assessment but carries procedural risk (~1:1000 perforation).
- Flexible sigmoidoscopy (once-off around age 55) has an evidence base from landmark RCTs but is less commonly used in Australia than FIT-based programmes.
- Stool DNA (e.g., Cologuard®) is not currently funded by the PBS or MBS in Australia and is not part of the NBCSP; it may be discussed in select clinical scenarios.
- Primary care clinicians are pivotal: opportunistic screening discussions, ensuring NBCSP participation, recognising red-flag symptoms (PR bleeding, iron deficiency anaemia, change in bowel habit), and timely referral.
- All patients with a positive non-invasive screening test must proceed to diagnostic colonoscopy — this is not optional and should occur within 30 days ideally.
- Aboriginal and Torres Strait Islander peoples experience higher CRC incidence and mortality with later-stage diagnosis; culturally safe engagement and addressing barriers to screening are essential.
- Post-polypectomy surveillance intervals follow the 2020 Colorectal Cancer Screening Guidelines: low-risk adenoma → repeat colonoscopy in 5 years; high-risk adenoma → repeat colonoscopy in 3 years.
- Iron deficiency anaemia in any adult, particularly men and postmenopausal women, warrants investigation to exclude CRC regardless of age.
Introduction & Australian Epidemiology
Colorectal cancer (CRC) — encompassing cancers of the colon, rectum, and anus — is a leading cause of cancer-related morbidity and mortality in Australia. The adenoma-carcinoma sequence provides a prolonged window of opportunity during which precursor polyps can be detected and removed, making CRC one of the most screen-preventable malignancies.
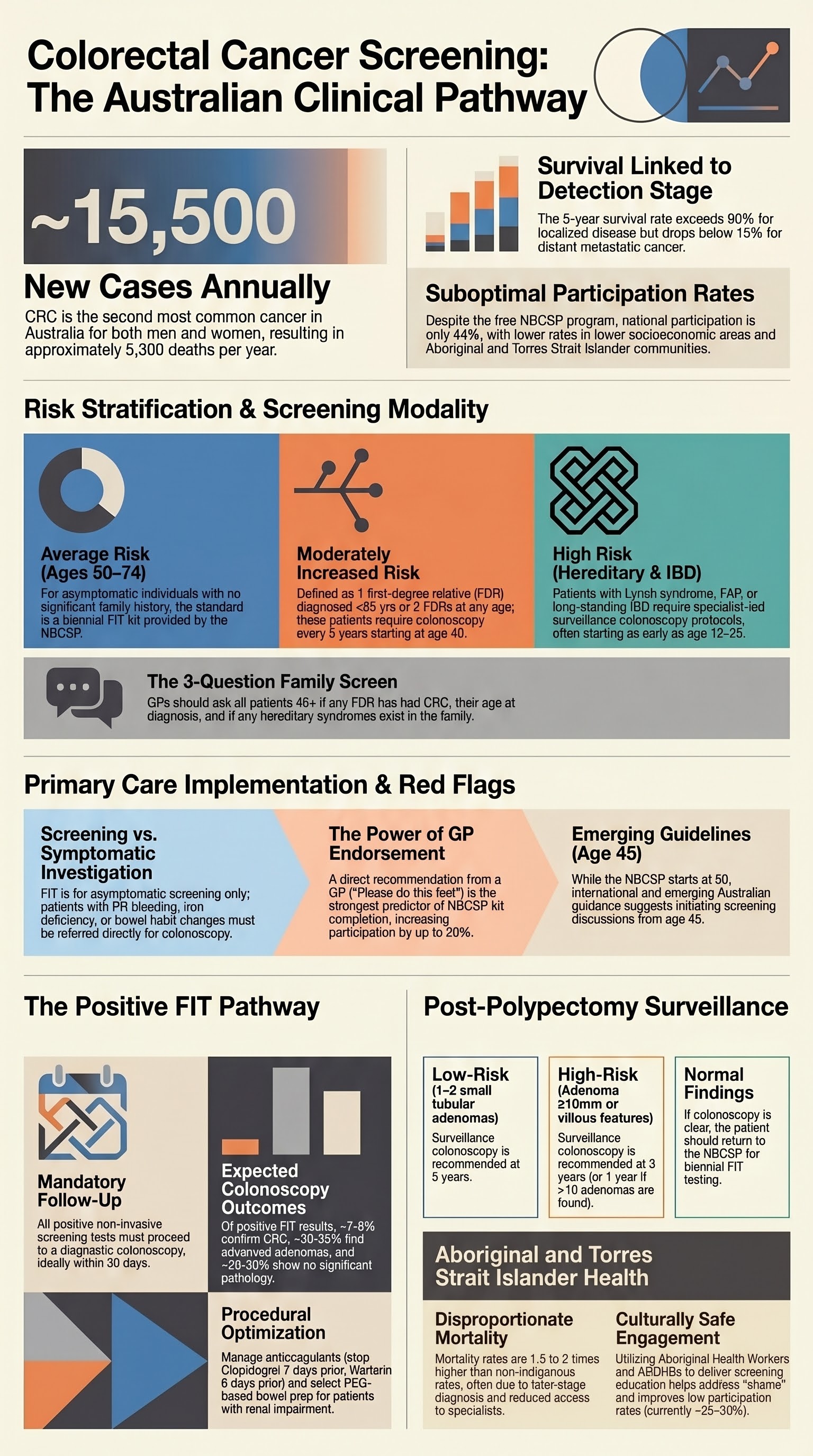
According to the Australian Institute of Health and Welfare (AIHW), CRC is the second most commonly diagnosed cancer in both men and women in Australia, with an estimated 15,500 new cases diagnosed annually. It remains the second leading cause of cancer death, responsible for approximately 5,300 deaths per year. The five-year relative survival rate is approximately 70%, but this varies markedly by stage at diagnosis — exceeding 90% for localised disease but falling below 15% for distant metastatic disease.
The Australian Government established the National Bowel Cancer Screening Program (NBCSP) in 2006, which has been progressively expanded. Since 2020, all Australians aged 50–74 receive a free immunochemical faecal occult blood test (iFIT/FIT) kit by mail every two years. Participation rates, however, remain suboptimal at approximately 44% nationally, with lower rates among men, those in lower socioeconomic areas, and Aboriginal and Torres Strait Islander peoples.
| Statistic | Value | Source |
|---|---|---|
| New cases per year (est.) | ~15,500 | AIHW 2023 |
| Deaths per year (est.) | ~5,300 | AIHW 2023 |
| 5-year survival (all stages) | ~70% | AIHW Cancer Data |
| NBCSP participation rate | ~44% | AIHW NBCSP Report 2023 |
| NBCSP target age range | 50–74 years | Australian Government DoH |
| Screening interval | Every 2 years | NBCSP |
Risk Stratification & Screening Modalities
Risk stratification is the foundation of an effective CRC screening strategy. Individuals are categorised into average risk, moderately increased risk, and high risk based on personal and family history, with each category dictating the recommended screening modality, starting age, and surveillance interval.
Risk Categories
Screening Modalities
| Modality | Sensitivity (CRC) | Specificity | Interval | Australian Availability | Best For |
|---|---|---|---|---|---|
| FIT (Faecal Immunochemical Test) | ~74% (single round); >90% programme sensitivity | ~95% | Every 2 years | NBCSP (free); MBS item 66766 | Average risk, population screening |
| Colonoscopy | ~95% | ~90% | Every 5–10 years (risk-dependent) | MBS item 32222 (colonoscopy); all states | Positive FIT, high risk, surveillance |
| Flexible Sigmoidoscopy | ~70–75% (distal CRC) | ~95% | Once-off (age 55) or every 10 yrs | Available; MBS item 32218 | Average risk (distal colon assessment) |
| Stool DNA / Multitarget Stool DNA | ~92% | ~87% | Every 3 years | Not PBS/MBS funded; available privately | Select cases; not first-line in Australia |
| CT Colonography (Virtual Colonoscopy) | ~90% (>10 mm polyps) | ~86% | Every 5 years | Available; MBS item 57721 (specialist request only) | Patients unable to undergo colonoscopy |
Modality Details
Faecal Immunochemical Test (FIT)
The FIT detects human haemoglobin in stool using antibody-based immunoassay technology. Unlike older guaiac-based faecal occult blood tests (gFOBT), FIT is specific for human globin (not affected by dietary peroxidases) and has superior sensitivity for CRC and advanced adenomas. The NBCSP uses a quantitative FIT with a cut-off of 100 ng/mL buffer (~20 µg Hb/g faeces). A single FIT sample is sufficient for the NBCSP kit.
Colonoscopy
Colonoscopy is the most sensitive and specific test for CRC detection and enables simultaneous biopsy and polypectomy. It requires full bowel preparation, sedation (typically propofol-based monitored anaesthesia care in Australia), and carries a procedural perforation risk of approximately 1 in 1,000 and a significant bleeding risk of 1 in 200 (higher with polypectomy). Adequate bowel preparation and caecal intubation rates (>95%) are quality benchmarks per Gastroenterological Society of Australia (GESA) standards.
Flexible Sigmoidoscopy
Flexible sigmoidoscopy examines the rectum and sigmoid/descending colon to approximately 60 cm. The UK Flexible Sigmoidoscopy Screening Trial demonstrated a 33% reduction in CRC incidence and 43% reduction in CRC mortality with a single screen at age 55–64. In Australia, it is less commonly used as a primary screening tool but remains valuable when colonoscopy is contraindicated or as part of diagnostic workup.
Stool DNA (Multitarget Stool DNA)
Multitarget stool DNA testing (e.g., Cologuard®, combining methylated DNA markers and FIT) has higher single-round sensitivity for CRC (~92%) than FIT alone (~74%), but at the cost of lower specificity (~87% vs ~95%). This test is not currently funded by the PBS or MBS in Australia and is not part of the NBCSP. It may be considered in specific clinical scenarios where colonoscopy is declined or contraindicated, but clinicians should counsel regarding the higher false-positive rate.
Recommended Approach by Risk Level
| Risk Level | First-Line Screening | Start Age | Interval | Alternative / Adjunct |
|---|---|---|---|---|
| Average | FIT (NBCSP) | 50 years | Every 2 years | Flexible sigmoidoscopy once-off at 55; discuss from age 45 per emerging guidance |
| 1 FDR CRC ≥55 yrs | FIT (NBCSP) acceptable | 50 years (or 10 yrs before FDR dx) | Every 2 years | Consider colonoscopy discussion |
| 1 FDR CRC <55 yrs or ≥2 FDRs | Colonoscopy | 40 years (or 10 yrs before youngest FDR dx) | Every 5 years | Genetic counselling referral |
| Lynch syndrome | Colonoscopy | 25 years (or 10 yrs before youngest family dx) | Every 1–2 years | Genetic counselling; consider aspirin chemoprevention |
| FAP | Flexible sigmoidoscopy / colonoscopy | 12–15 years | Every 1–2 years | Genetic testing; prophylactic colectomy discussion |
| IBD (extensive colitis >8 yrs) | Surveillance colonoscopy with chromoendoscopy | 8 years after symptom onset | Every 1–3 years (risk-dependent) | Pancolonic dye-spray or virtual chromoendoscopy preferred |
Primary Care Implementation
General practitioners (GPs) are the cornerstone of CRC screening in Australia. Primary care clinicians are responsible for opportunistic screening discussions, supporting NBCSP participation, assessing risk, initiating appropriate referrals, and managing surveillance recall.
When to Start Screening
Family History Assessment — The 3-Question Screen
Every adult presenting for a health check or aged 45+ should be asked:
- Has any first-degree relative (parent, sibling, child) been diagnosed with colorectal cancer?
- If yes, how old were they at diagnosis? (Before or after 55 years?)
- Is there a known hereditary cancer syndrome in the family (e.g., Lynch syndrome, FAP)?
Opportunistic Screening Strategies in General Practice
- Health assessments: Incorporate CRC screening into 45–49-year-old health checks, 75+ health assessments, and Aboriginal and Torres Strait Islander health checks (MBS item 715).
- Chronic disease consultations: Use diabetes, cardiovascular, or other chronic disease reviews as an opportunity to discuss CRC screening status.
- Practice registers and recalls: Maintain a register of patients aged 50–74 and their screening status. Use clinical software (e.g., Best Practice, Medical Director) to set reminders for overdue screening.
- Patient education: Provide written resources (Cancer Council Australia pamphlets) and explain the purpose, simplicity, and importance of the FIT kit.
- Address barriers: Common reasons for non-participation include embarrassment, lack of awareness, perceived low risk, and forgetting. Direct GP endorsement significantly improves uptake.
MBS Items Relevant to CRC Screening in Primary Care
| MBS Item | Description | Relevance |
|---|---|---|
| 715 | Aboriginal and Torres Strait Islander health check | Opportunity to assess CRC screening status and risk |
| 699 | GP Management Plan (GPMP) | Incorporate screening recall into chronic disease management |
| 10997 | GP consultation (Level C — extended) | For detailed family history assessment and risk counselling |
| 66766 | Faecal occult blood test (FIT) | If ordering FIT outside NBCSP (symptomatic patients) |
Comorbidities and Life Expectancy Considerations
Screening decisions in older adults (≥75 years) and those with significant comorbidities should be individualised based on life expectancy, functional status, and patient preference. Screening is unlikely to benefit patients with a life expectancy of less than 10 years, as the natural history of the adenoma-carcinoma sequence means the harms of screening and colonoscopy may outweigh benefits. Conversely, healthy older adults may continue to benefit from screening.
Follow-Up of Positive Tests
A positive non-invasive screening test (FIT, stool DNA) is not a diagnosis of cancer but indicates the need for definitive investigation with colonoscopy. Timely follow-up is critical — delays of more than 6 months are associated with more advanced-stage cancer at diagnosis.
Pathway After Positive FIT
Positive FIT — Expected Findings at Colonoscopy
| Finding | Approximate Proportion | Action |
|---|---|---|
| CRC confirmed | ~7–8% | Staging (CT chest/abdomen/pelvis); MDT referral; surgical/oncology |
| Advanced adenoma (≥10 mm, villous, high-grade dysplasia) | ~30–35% | Polypectomy; surveillance colonoscopy in 3 years |
| Non-advanced adenoma (<10 mm, tubular) | ~25–30% | Polypectomy; surveillance colonoscopy in 5 years |
| No significant pathology | ~25–30% | Return to NBCSP (biennial FIT); consider upper GI source if anaemia |
Post-Polypectomy Surveillance
Surveillance colonoscopy intervals should be determined by the highest-risk finding at index colonoscopy, in accordance with the 2020 Australian Colorectal Cancer Screening Guidelines and Cancer Council Australia recommendations.
| Index Colonoscopy Finding | Surveillance Interval | Notes |
|---|---|---|
| Normal or hyperplastic polyps only | No surveillance needed; return to NBCSP | FIT every 2 years per NBCSP |
| 1–2 small (<10 mm) tubular adenomas, no villous features | 5 years | Low-risk adenoma |
| 3–4 small tubular adenomas | 3 years | Intermediate risk |
| ≥5 adenomas, or any adenoma ≥10 mm, or villous features, or high-grade dysplasia | 3 years (or 1 year if ≥10 adenomas) | High-risk adenoma; consider 1 year if very high adenoma burden |
| Sessile serrated lesions (SSL) ≥10 mm or with dysplasia | 3 years | Serrated polyposis syndrome → annual colonoscopy |
| CRC resected | 1 year post-surgery, then per protocol | CEA monitoring; CT surveillance per MDT |
Tracking and Communication
- Practice systems: Use clinical software flags and recall systems to track all patients with positive FIT results. Every positive FIT should have a documented outcome — colonoscopy booked, completed, or patient declined (with documented counselling).
- Completion rates: Nationally, approximately 60–70% of patients with a positive NBCSP FIT complete follow-up colonoscopy. GPs play a crucial role in closing this gap by contacting patients directly and addressing barriers (cost, transport, anxiety, language).
- Patient communication: Provide clear, written follow-up instructions. Use interpreter services where needed. Emphasise that most positive FIT results do NOT indicate cancer.
- Medicare Safety Net: Patients may incur out-of-pocket costs for colonoscopy in private settings. Discuss the option of public hospital waitlist or identify bulk-billing colonoscopists where available.
Investigations
Investigations in CRC screening encompass the screening tests themselves and the diagnostic workup triggered by positive results or symptoms.
CRC Staging Investigations (for confirmed CRC)
Once CRC is confirmed histologically, staging is coordinated by the treating surgical or oncology team:
- CT chest/abdomen/pelvis with IV contrast: Standard staging imaging. MBS item 55054.
- Pelvic MRI: Essential for rectal cancer local staging (T and N staging, circumferential resection margin assessment). MBS item 63054.
- Carcinoembryonic antigen (CEA): Baseline serum CEA for post-treatment surveillance. MBS item 66398.
- PET-CT: Not routine; considered for equivocal findings on CT or suspected recurrence. MBS item 61605 (specialist request).
Special Populations
Pregnancy
Paediatrics & Young Adults
Elderly (≥75 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of colorectal cancer. While CRC incidence rates are broadly similar to or slightly lower than the non-Indigenous population, mortality rates are significantly higher — estimated at 1.5 to 2 times the non-Indigenous rate. This disparity reflects later-stage diagnosis, lower screening participation, reduced access to timely colonoscopy and specialist services, and the compounding effects of social determinants of health.
📚 References
- 1. Australian Institute of Health and Welfare. Bowel cancer screening in Australia: monitoring report. Canberra: AIHW; 2023.
- 2. Cancer Council Australia Colorectal Cancer Guidelines Working Party. Clinical practice guidelines for the prevention, early detection and management of colorectal cancer. Sydney: Cancer Council Australia; 2017 (updated 2020).
- 3. > US Preventive Services Task Force, Davidson KW, Barry MJ, et al. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325(19):1965–1977.
- 4. Wolf AMD, Fontham ETH, Church TR, et al. Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA Cancer J Clin. 2018;68(4):250–281.
- 5. > Atkin W, Wooldrage K, Parkin DM, et al. Long term effects of once-only flexible sigmoidoscopy screening after 17 years of follow-up: the UK Flexible Sigmoidoscopy Screening randomised controlled trial. Lancet. 2017;389(10076):1299–1311.
- 6. Imperiale TF, Ransohoff DF, Itzkowitz SH, et al. Multitarget stool DNA testing for colorectal-cancer screening. N Engl J Med. 2014;370(14):1287–1297.
- 7. Gastroenterological Society of Australia. Colonoscopy clinical care standards. Melbourne: GESA; 2020.
- 8. Australian Government Department of Health and Aged Care. National Bowel Cancer Screening Program. Canberra: DoH; 2024. Available from: https://www.health.gov.au/our-work/national-bowel-cancer-screening-program.
- 9. Hewitson P, Glasziou P, Watson E, Towler B, Irwig L. Cochrane systematic review of colorectal cancer screening using the fecal occult blood test (hemoccult): an update. Am J Gastroenterol. 2008;103(6):1541–1549.
- 10. Rex DK, Boland CR, Dominitz JA, et al. Colorectal cancer screening: recommendations for physicians and patients from the U.S. Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2017;153(1):307–323.
- 11. Cunningham M, Rumbold AR, Zhang X, Condon JR. Incidence, aetiology, and outcomes of cancer in Indigenous peoples in Australia. Lancet Oncol. 2008;9(6):585–595.
- 12. National Health and Medical Research Council. Clinical practice guidelines for the management of colorectal cancer. 2nd ed. Canberra: NHMRC; 2005 (superseded by Cancer Council guidelines; retained for historical context).
- 13. Rabeneck L, Paszat LF, Hilsden RJ, et al. Bleeding and perforation after outpatient colonoscopy and their risk factors in usual clinical practice. Gastroenterology. 2008;135(6):1899–1906.
- 14. Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colonoscopic polypectomy. N Engl J Med. 1993;329(27):1977–1981.