📋 Key Information Summary
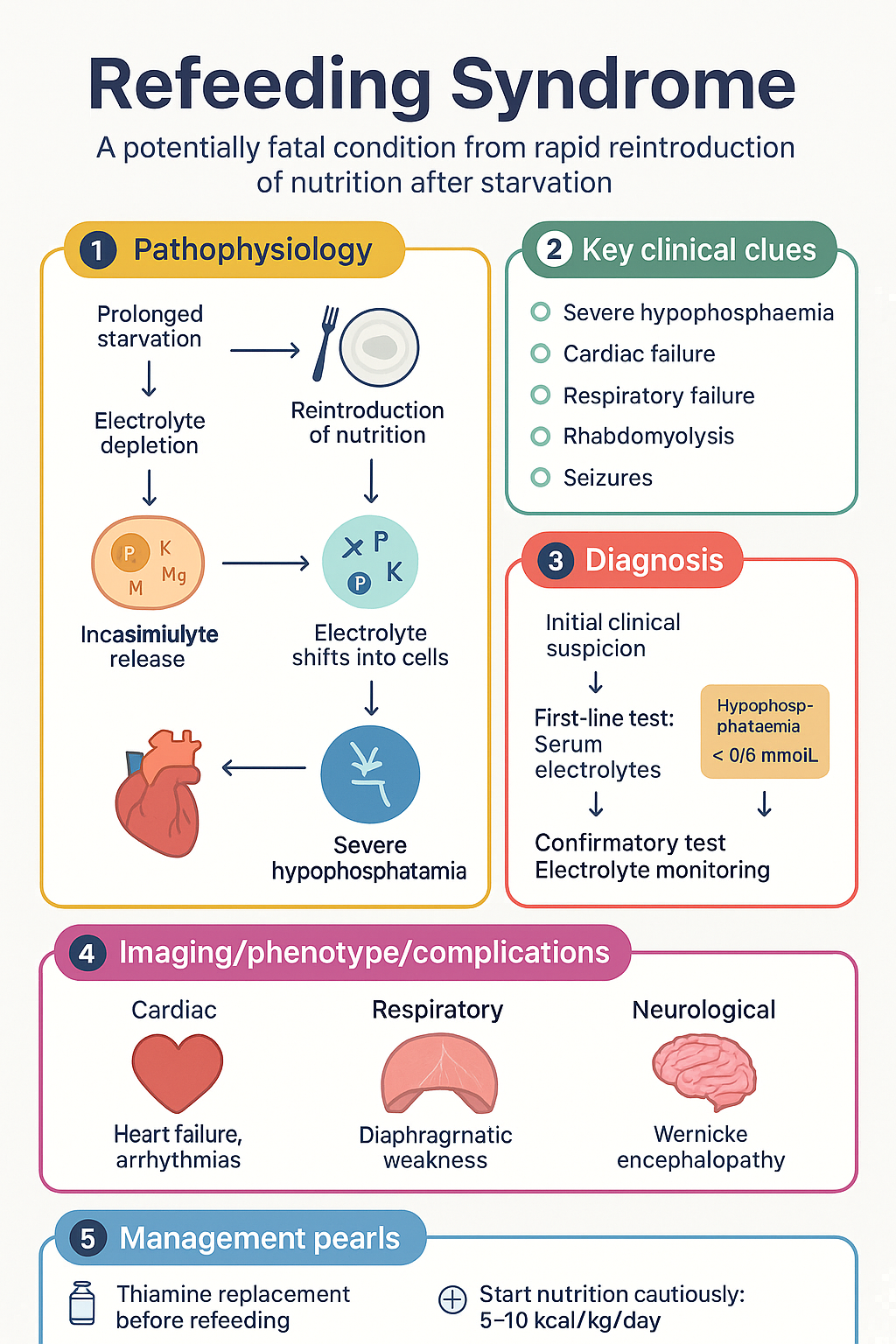
- Refeeding syndrome (RFS) is a potentially fatal condition caused by rapid reintroduction of nutrition after prolonged starvation, leading to acute shifts in electrolytes — primarily phosphate, potassium and magnesium — into depleted cells.
- Key electrolyte derangement is severe hypophosphataemia (<0.5 mmol/L), which can trigger cardiac failure, respiratory failure, rhabdomyolysis, seizures and death within days.
- Highest-risk patients: BMI <16 kg/m², >15% unintentional weight loss over 3–6 months, little or no nutritional intake for >10 days, and pre-feeding phosphate, potassium or magnesium below the normal range.
- Additional high-risk groups: chronic alcohol use disorder, anorexia nervosa, prolonged fasting (>5 days), active malignancy, post-bariatric surgery, chronic malabsorption and chronic use of antacids or diuretics.
- Thiamine replacement (200–300 mg IV or PO) and vitamin B complex must be given at least 30 minutes before — and for the first 3 days of — any refeeding.
- Start nutrition cautiously: 5–10 kcal/kg/day in highest-risk patients and 10–15 kcal/kg/day in high-risk patients; do not exceed 10 kcal/kg/day on day 1 for the very highest risk.
- Titrate caloric intake by no more than 5 kcal/kg/day every 2–3 days towards goal, ensuring electrolytes remain within normal limits before each increase.
- Mandatory daily monitoring of phosphate, magnesium, potassium, calcium, sodium and glucose for the first 72 hours; pre-feed ECG and continuous telemetry for highest-risk patients.
- Prophylactic daily electrolyte replacement is essential: phosphate 0.3–0.6 mmol/kg/day, magnesium 0.2 mmol/kg/day, potassium 1–2 mmol/kg/day — starting from day 1 of refeeding.
- Use cautious fluid management (restrict to 15–20 mL/kg/day); refeeding-associated fluid retention can precipitate acute heart failure and pulmonary oedema.
- Multidisciplinary team involvement is mandatory — dietitian, physician, pharmacist, nursing, and mental health support (especially in anorexia nervosa or chronic alcohol use disorder).
- Aboriginal and Torres Strait Islander peoples are disproportionately affected by food insecurity, chronic disease and malnutrition; culturally safe refeeding pathways must be integrated with local Aboriginal Medical Services.
Introduction & Australian Epidemiology
Refeeding syndrome (RFS) describes the potentially fatal metabolic derangement that occurs when nutrition — oral, enteral or parenteral — is reintroduced to a patient who has been chronically or severely malnourished. The hallmark is rapid intracellular movement of phosphate, potassium and magnesium driven by insulin release and anabolic recovery, causing life-threatening serum depletions.
First described among famine victims after World War II, RFS remains a common and under-recognised complication in contemporary Australian hospitals. The AIHW reports that malnutrition affects 20–50% of Australian hospital inpatients, and a significant proportion of those requiring nutritional rehabilitation are at risk of RFS. The condition carries a reported mortality of up to 25% when severe hypophosphataemia is not promptly recognised and treated.
In Australia, high-risk populations include patients with anorexia nervosa (estimated prevalence 1–2% in young women, per Butterfly Foundation data), chronic alcohol use disorder — particularly prevalent in remote and Indigenous communities — advanced malignancy, chronic bowel disease, post-bariatric surgery patients, and elderly individuals in residential aged-care facilities. NHMRC-endorsed screening tools such as the Malnutrition Screening Tool (MST) should be used at every hospital admission and aged-care review.
This guideline synthesises current NICE CG32, ASPEN 2020 clinical guidance, and Australasian Society of Parenteral and Enteral Nutrition (AuSPEN) recommendations for risk stratification, prevention and management of refeeding syndrome.
Pathophysiology
During prolonged starvation (typically >48–72 hours), the body adapts by shifting from glucose-based to fat and ketone-based metabolism. Intracellular stores of phosphate, potassium and magnesium become progressively depleted, although serum levels may remain low-normal due to extracellular redistribution and reduced renal excretion. This gives a misleading impression of metabolic stability.
When carbohydrate-rich nutrition is reintroduced, insulin secretion rises sharply. Insulin stimulates the sodium–potassium ATPase pump (Na⁺/K⁺-ATPase), driving phosphate, potassium, magnesium, glucose and water into cells. Simultaneously, anabolic processes (protein synthesis, glycolysis, ATP production) consume intracellular phosphate and magnesium at accelerated rates. The result is a rapid, often precipitous drop in serum phosphate, potassium and magnesium within 12–72 hours of refeeding onset.
The consequences are multi-organ:
- Cardiac: Hypophosphataemia impairs myocardial contractility (reduced ATP), leading to heart failure, arrhythmias and cardiac arrest. Thiamine deficiency compounds this with high-output heart failure (wet beriberi).
- Respiratory: Diaphragmatic muscle weakness from depleted ATP and phosphate reduces respiratory drive, potentially causing acute respiratory failure.
- Metabolic: Refeeding-induced hyperglycaemia and hyperinsulinaemia exacerbate intracellular fluid shift, causing fluid overload and oedema.
- Neurological: Hypophosphataemia can cause confusion, seizures, paraesthesias, and Wernicke encephalopathy (from concomitant thiamine depletion).
- Haematological: Reduced 2,3-DPG from low phosphate impairs oxygen delivery; haemolysis may occur at very low phosphate levels.
The severity of RFS correlates directly with the degree of pre-existing malnutrition and the rate of caloric reintroduction. This is why a graduated, protocol-driven approach to refeeding is essential.
Clinical Presentation & Diagnostic Criteria
There is no single universally accepted diagnostic criterion for RFS. The diagnosis is clinical, supported by laboratory findings, and is defined as the onset of electrolyte and fluid abnormalities following the initiation of nutrition in a malnourished patient. The NICE CG32 guideline (2006, updated 2017) and the Academy of Nutrition and Dietetics (AND) consensus definition require:
Timeline of onset:
Presenting features to recognise:
- New-onset or worsening peripheral or sacral oedema
- Tachycardia, new arrhythmias, or signs of acute heart failure (dyspnoea, raised JVP, pulmonary crepitations)
- Acute respiratory failure or unexplained hypoxaemia (diaphragmatic weakness)
- Generalised muscle weakness, including difficulty weaning from ventilator support
- Seizures, confusion, Wernicke encephalopathy (ophthalmoplegia, ataxia, confusion)
- Rhabdomyolysis (dark urine, elevated CK) at very low phosphate levels
- Hyperglycaemia, particularly in previously malnourished patients commenced on glucose-containing feeds
Risk Assessment
Screening for RFS risk must be performed before any nutrition support is initiated. NICE CG32 and ASPEN 2020 guidelines identify specific clinical criteria. Patients meeting one or more high-risk criteria or two or more other-risk criteria should be managed with a refeeding protocol.
High-Risk Groups in Australian Practice
| High-Risk Group | Mechanism of Risk | Australian Relevance |
|---|---|---|
| Anorexia nervosa | Prolonged self-imposed starvation, severe cachexia | ~1–2% prevalence in young women; butterfly foundation estimates ~1 million Australians affected by eating disorders |
| Chronic alcohol use disorder | Poor intake, vomiting, thiamine depletion, direct cardiac and hepatic toxicity | Significant burden in rural, remote and Indigenous communities; highest hospitalisation rates in NT and WA |
| Prolonged fasting (>5–10 days) | Complete substrate depletion; metabolic adaptation to ketosis | Post-operative patients (prolonged ileus, strict NBM), critically ill ICU patients |
| Active malignancy | Cancer cachexia, chemotherapy-induced anorexia and mucositis | Nutritional failure in ~30–50% of advanced cancer patients (Cancer Council Australia) |
| Post-bariatric surgery | Reduced absorptive surface, rapid food restriction, dumping | Rising prevalence with ~20,000 bariatric procedures annually in Australia |
| Chronic malabsorption | Coeliac disease, short bowel syndrome, IBD — chronic micronutrient loss | Coeliac prevalence ~1% nationally |
| Elderly / residential aged care | Sarcopenia, poor dentition, polypharmacy, social isolation | Malnutrition prevalence 22–50% in aged-care facilities (AIHW) |
Pre-Feeding Laboratory Assessment
Before commencing any nutrition support, obtain and review:
Prevention & Management
Prevention is far more effective than treatment of established RFS. The following protocol should be applied to all patients identified as at risk by the screening criteria above. This protocol is adapted from NICE CG32, ASPEN 2020, AuSPEN guidelines and Australian clinical practice.
Step 1: Pre-Feeding Thiamine & Vitamin Supplementation
Step 2: Caloric Initiation & Titration
The rate of caloric reintroduction must be graded according to risk level:
Step 3: Electrolyte Replacement Protocol
Prophylactic electrolyte replacement must begin from day 1 of refeeding, regardless of whether serum levels are within normal range. Intracellular depletion is universal in malnourished patients.
Step 4: Fluid Management
Step 5: Cardiac & Clinical Monitoring
| Monitoring Parameter | Frequency | Duration |
|---|---|---|
| Serum phosphate, potassium, magnesium | Every 12 hours (daily minimum) | First 72 hours, then daily until stable for 48 h |
| Serum sodium, calcium, glucose | Daily | First 7 days |
| Urea, creatinine, eGFR | Daily | First 3–5 days |
| 12-lead ECG | Baseline + repeat if K⁺, Mg²⁺ or PO₄³⁻ abnormal | Throughout refeeding |
| Continuous telemetry | Continuous | Highest-risk patients for first 72 hours |
| Fluid balance (strict I&O) | Hourly | First 72 hours, then 4–6 hourly |
| Daily weight | Daily, same time, same scales | Minimum first 7 days |
| Respiratory rate, SpO₂ | 4-hourly minimum | First 5 days |
Step 6: Multidisciplinary Nutrition Support
Refeeding syndrome prevention and management requires a coordinated multidisciplinary approach:
- Dietitian (Accredited Practising): Leads nutritional assessment, prescribes feeding regimen, caloric titration schedule, and electrolyte replacement calculations. Must review daily in highest-risk patients.
- Medical officer / physician: Oversees overall management, interprets electrolytes and ECG, manages acute complications, prescribes IV supplementation.
- Pharmacist: Verifies electrolyte dosing, checks for drug–nutrient interactions (e.g., diuretics, insulin, digoxin), ensures thiamine is given prior to feeds.
- Nursing: Monitors fluid balance, vital signs, administers IV electrolytes, assesses for oedema and respiratory deterioration. Must escalate phosphate <0.5 mmol/L urgently.
- Mental health team: Essential for anorexia nervosa and chronic alcohol use disorder. Psychological support, motivational interviewing, and supervised meal plans improve outcomes.
- Speech pathology: Swallowing assessment where dysphagia may be contributing to malnutrition (e.g., post-stroke, neurological disease).
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. National Institute for Health and Care Excellence (NICE). Nutrition support for adults: oral nutrition support, enteral tube feeding and parenteral nutrition. Clinical guideline CG32. London: NICE; 2006 (updated 2017).
- 2. da Silva JSV, Seres DS, Sabino K, et al. ASPEN consensus recommendations for refeeding syndrome. Nutrition in Clinical Practice. 2020;35(2):178–195.
- 3. Friedli N, Stanga Z, Sobotka L, et al. Revisiting the refeeding syndrome: results of a systematic review. Nutrition. 2017;35:151–160.
- 4. Crook MA, Hally V, Panteli JV. The importance of the refeeding syndrome. Nutrition. 2001;17(7–8):632–637.
- 5. Mehanna HM, Moledina J, Travis J. Refeeding syndrome: what it is, and how to prevent and treat it. BMJ. 2008;336(7659):1495–1498.
- 6. Stanga Z, Brunner A, Braga M, et al. Artificial nutrition in clinical practice: refeeding syndrome. Best Practice & Research Clinical Gastroenterology. 2023;64–65:101842.
- 7. Australian Institute of Health and Welfare (AIHW). Nutrition across the life stages. Cat. no. PHE 227. Canberra: AIHW; 2018.
- 8. Australasian Society of Parenteral and Enteral Nutrition (AuSPEN). AuSPEN clinical guidelines for parenteral and enteral nutrition. Asia Pacific Journal of Clinical Nutrition. 2014;23(4):522–540.
- 9. National Health and Medical Research Council (NHMRC). Australian dietary guidelines. Canberra: NHMRC; 2013.
- 10. Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice. 10th edition. East Melbourne: RACGP; 2024.
- 11. World Health Organization (WHO). Guideline: updates on the management of severe acute malnutrition in infants and children. Geneva: WHO; 2013.
- 12. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd edition. Sydney: ACSQHC; 2021.