📋 Key Information Summary
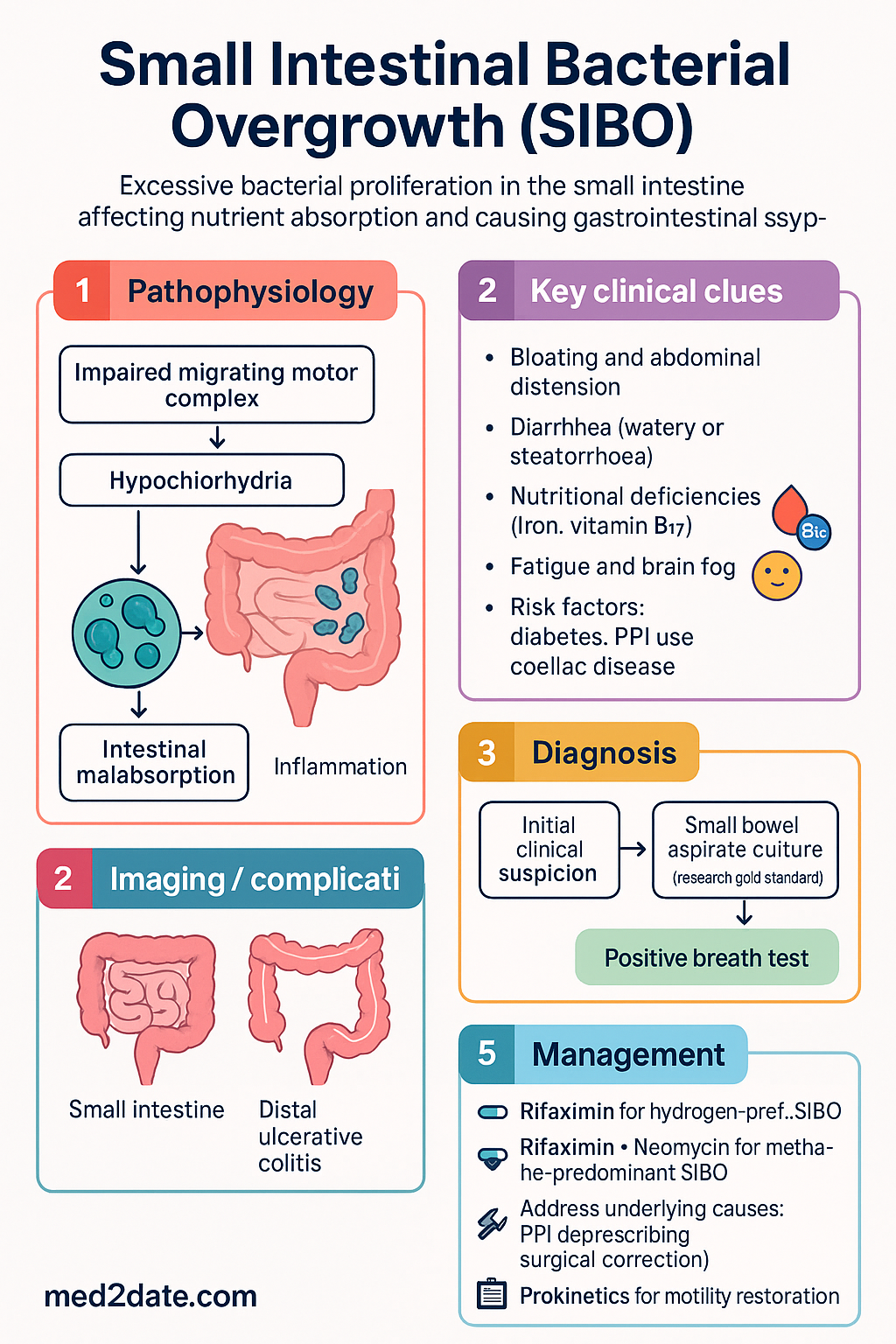
- Small intestinal bacterial overgrowth (SIBO) is defined as an excessive proliferation of bacteria in the small intestine — typically ≥10³ CFU/mL on jejunal aspirate culture.
- SIBO is increasingly recognised in Australia, particularly in patients with irritable bowel syndrome (IBS), diabetes mellitus, coeliac disease, and prior abdominal surgery.
- The two primary diagnostic modalities available in Australia are glucose hydrogen breath test (G-HBT) and lactulose hydrogen-methane breath test (L-HMBT), interpreted using North American consensus criteria.
- A positive breath test is defined as a rise in hydrogen ≥20 ppm above baseline within 90 minutes (glucose) or 120 minutes (lactulose), OR a methane level ≥10 ppm at any point.
- Small bowel aspirate culture remains the research gold standard (≥10³ CFU/mL diagnostic) but is rarely performed in routine Australian practice due to invasiveness and cost.
- Predisposing factors include motility disorders (diabetic gastroparesis, scleroderma), anatomic abnormalities (blind loops, strictures, surgical diversions), hypochlorhydria (PPI use, atrophic gastritis), and immunodeficiency.
- Hydrogen-predominant SIBO is treated with rifaximin 550 mg PO TDS for 14 days — the first-line agent in Australia (PBS Authority Required for SIBO indication).
- Methane-predominant overgrowth (intestinal methanogen overgrowth, IMO) requires combination therapy: rifaximin 550 mg TDS + neomycin 500 mg BD for 14 days.
- Recurrent SIBO is common (up to 44%); rotating antibiotic regimens and prokinetics (low-dose erythromycin, prucalopride) to restore motility are recommended to reduce recurrence.
- Identifying and addressing the underlying cause is essential for sustained remission — PPI deprescribing, surgical correction, and glycaemic optimisation in diabetes are key strategies.
- Aboriginal and Torres Strait Islander peoples may face higher SIBO prevalence due to higher rates of chronic disease, limited specialist access in remote areas, and food insecurity affecting dietary management.
Introduction & Australian Epidemiology
Small intestinal bacterial overgrowth (SIBO) is a condition characterised by an abnormal increase in the number and/or type of bacteria in the small intestine, typically defined as ≥10³ colony-forming units per millilitre (CFU/mL) on culture of a small bowel aspirate. The condition leads to malabsorption, bloating, diarrhoea, and nutritional deficiency through bile acid deconjugation, mucosal inflammation, and competitive nutrient consumption.
In Australia, SIBO is increasingly recognised as a clinically significant condition. Prevalence estimates vary widely depending on the population studied and the diagnostic method used. Among patients meeting Rome IV criteria for irritable bowel syndrome (IBS), breath-test-positive SIBO is detected in approximately 30–40% — a figure consistent with international data. Australian gastroenterologists report growing referrals for breath testing, particularly in patients with refractory IBS, bloating-predominant functional bowel disorders, and coeliac disease with ongoing symptoms despite a gluten-free diet.
SIBO can be categorised by the predominant gas produced: hydrogen-predominant SIBO, methane-predominant overgrowth (now termed intestinal methanogen overgrowth, IMO), and hydrogen sulphide-predominant (emerging diagnostic paradigm). This distinction is clinically important as treatment strategies differ. The microbiology of SIBO typically involves commensal organisms — Escherichia coli, Klebsiella, Enterococcus, and Streptococcus species — rather than frank pathogens, though community-acquired resistant organisms (including ESBL-producing Enterobacterales) may be encountered.
Pathophysiology
The small intestine maintains relative sterility compared to the colon through several defence mechanisms. Disruption of one or more of these mechanisms leads to SIBO:
- Migrating motor complex (MMC): The phase III motor complex sweeps residual luminal contents distally during fasting (approximately every 90–120 minutes). Impairment of the MMC — as seen in diabetic autonomic neuropathy, scleroderma, or opioid use — is the single most important mechanism for SIBO development.
- Gastric acid secretion: Gastric acid acts as a bactericidal barrier. Hypochlorhydria from chronic PPI therapy, atrophic gastritis, or Helicobacter pylori-related gastric atrophy permits oral flora to colonise the proximal small bowel.
- Ileocaecal valve competence: The ileocaecal valve prevents colonic reflux. Surgical resection, Crohn's disease, or anatomical bypass renders this mechanism ineffective.
- Intestinal immune function: Secretory IgA, Paneth cell antimicrobial peptides (defensins, lysozyme), and intact mucosal immunity control bacterial load. Immunodeficiency states (HIV, common variable immunodeficiency) predispose to SIBO.
- Anatomical factors: Blind loops (post-surgical), strictures (Crohn's disease, radiation enteritis), diverticula (including duodenal and jejunal diverticulosis), and surgically created loops cause stasis and bacterial proliferation.
The consequences of SIBO include: bile acid deconjugation leading to fat malabsorption and steatorrhoea; carbohydrate fermentation causing bloating, flatulence, and diarrhoea; competitive consumption of vitamin B₁₂ and iron leading to deficiency; direct mucosal injury producing villous blunting and crypt hyperplasia; and D-lactic acidosis from carbohydrate malabsorption in extreme cases.
Clinical Presentation & Diagnostic Criteria
Clinical Features
SIBO presents with a spectrum of non-specific gastrointestinal and systemic symptoms. The clinical picture may mimic IBS, coeliac disease, or inflammatory bowel disease:
- Gastrointestinal: Bloating and abdominal distension (most common), flatulence, diarrhoea (watery or steatorrhoeic), abdominal cramping, nausea, early satiety
- Nutritional: Weight loss, iron deficiency anaemia, vitamin B₁₂ deficiency (with macrocytosis), fat-soluble vitamin deficiencies (A, D, E, K), folate deficiency (paradoxically elevated in SIBO due to bacterial synthesis)
- Systemic: Fatigue, brain fog, peripheral neuropathy (from B₁₂ deficiency), bone pain (from vitamin D deficiency), night blindness (from vitamin A deficiency)
- Musculoskeletal: Arthralgia, myalgia — particularly in co-existent coeliac disease
When to Suspect SIBO
| Clinical Scenario | Risk Factor Category |
|---|---|
| Type 1 or type 2 diabetes with gastroparesis | Motility disorder |
| Systemic sclerosis / scleroderma | Motility disorder |
| Chronic opioid use | Motility disorder |
| Post-surgical (Billroth II, Roux-en-Y, ileocaecal resection) | Anatomic abnormality |
| Crohn's disease with strictures | Anatomic abnormality |
| Jejunal or duodenal diverticulosis | Anatomic abnormality |
| Long-term PPI therapy (>12 months) | Hypochlorhydria |
| Atrophic gastritis / H. pylori-associated atrophy | Hypochlorhydria |
| Coeliac disease with ongoing symptoms on GFD | Motility + immune |
| HIV / common variable immunodeficiency | Immunodeficiency |
| Recurrent courses of broad-spectrum antibiotics | Dysbiosis |
| Irritable bowel syndrome (especially bloating-predominant) | Associated condition |
Diagnosis
Diagnosis of SIBO in Australia is primarily based on breath testing, interpreted using the North American Consensus criteria. Small bowel aspirate culture, while the research gold standard, is rarely performed in routine clinical practice.
Hydrogen–Methane Breath Testing
Breath testing exploits the principle that bacteria in the small intestine ferment ingested substrates (glucose or lactulose), producing hydrogen and/or methane that is absorbed into the bloodstream and excreted via the lungs. Both glucose and lactulose substrates are available in Australia, and the choice between them involves trade-offs in sensitivity and specificity.
| Parameter | Glucose Hydrogen Breath Test (G-HBT) | Lactulose Hydrogen-Methane Breath Test (L-HMBT) |
|---|---|---|
| Substrate dose | 75 g glucose in 250 mL water | 10 g lactulose in 200 mL water |
| Positive criterion — H₂ | Rise ≥20 ppm above baseline within 90 minutes | Rise ≥20 ppm above baseline within 90–120 minutes (dual-peak pattern may be used as supportive) |
| Positive criterion — CH₄ | Methane ≥10 ppm at any time point | Methane ≥10 ppm at any time point |
| Sensitivity | 40–93% (limited by proximal absorption) | 31–68% (dual-peak may increase sensitivity) |
| Specificity | 44–100% | 44–100% |
| Advantages | Higher specificity; fewer false positives; glucose absorbed in proximal small bowel | Detects distal small bowel overgrowth; assesses methane (IMO); widely available in Australia |
| Disadvantages | May miss distal SIBO; glucose absorbed before reaching distal jejunum | Colonic fermentation may produce false-positive early peaks; lower specificity |
| MBS availability | Not MBS-listed; out-of-pocket ~0–200 | Not MBS-listed; out-of-pocket ~0–200 |
Small Bowel Aspirate Culture
Aspiration and quantitative culture of small bowel contents (typically via upper endoscopy with aspiration from the jejunum under fluoroscopic guidance or enteroscopy) remains the research gold standard. A bacterial count of ≥10³ CFU/mL is diagnostic — this threshold is lower than the historical ≥10⁵ CFU/mL, reflecting updated consensus.
- Advantages: Direct bacterial quantification and speciation; identification of antibiotic sensitivities; exclusion of alternative diagnoses
- Limitations: Invasive (requires endoscopy); risk of contamination from oral/pharyngeal flora; poor sensitivity due to sampling error (bacteria may be patchy); not standardised in Australian practice; costly (no specific MBS item)
- Commonly identified organisms: Escherichia coli, Klebsiella pneumoniae, Enterococcus spp., Streptococcus spp., Staphylococcus spp. — typically commensal organisms rather than frank pathogens
Identification of Predisposing Factors
A critical component of SIBO management is identifying and addressing the underlying predisposing cause. Without addressing the root aetiology, recurrence rates exceed 40%:
Investigations — Summary
Treatment
First-Line Antibiotic Therapy
The cornerstone of SIBO treatment is non-absorbable or minimally absorbable antibiotics aimed at reducing the intraluminal bacterial load. Antibiotic selection is guided by the predominant gas on breath testing.
Hydrogen-Predominant SIBO
Methane-Predominant Overgrowth (Intestinal Methanogen Overgrowth — IMO)
Methane production is driven by archaea (primarily Methanobrevibacter smithii), not bacteria. Methane slows intestinal transit and exacerbates constipation. Monotherapy with rifaximin is inadequate for IMO; combination therapy is required.
Alternative and Second-Line Agents
When rifaximin is unavailable, contraindicated, or ineffective, the following alternatives may be considered:
Rotating Antibiotic Regimens for Recurrent SIBO
Recurrence of SIBO is common — up to 44% of patients relapse within 12 months after successful initial treatment. For patients with recurrent SIBO, a rotating antibiotic strategy may be employed:
Prokinetic Therapy
Prokinetic agents address the underlying motility impairment responsible for many SIBO cases. They should be considered as adjunctive therapy — particularly in recurrent or refractory SIBO — and continued after antibiotic courses to prevent recurrence.
Addressing the Underlying Cause
Successful long-term management of SIBO requires identification and treatment of the predisposing factor. Without addressing the root cause, recurrence rates are high:
- PPI deprescribing: If long-term PPI therapy is not clearly indicated (per RACGP guidelines), step down to H₂ receptor antagonists (famotidine 20 mg PO BD) or discontinue with monitoring
- Diabetic optimisation: Tight glycaemic control to reduce autonomic neuropathy; consider diabetic gastroparesis management (metoclopramide, domperidone)
- Surgical correction: Where anatomical factors are correctable (e.g., stricturoplasty, blind loop revision)
- Opioid reduction: Taper or cease opioids if possible; consider opioid-sparing pain strategies; if ongoing use, consider peripherally acting μ-opioid receptor antagonists (naloxegol — Movantik®)
- Immunodeficiency management: Treat underlying HIV; consider immunoglobulin replacement for CVID
- Dietary modification: Low FODMAP diet may reduce symptoms; elemental diet has evidence for bacterial reduction; ensure adequate nutrition
Monitoring
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Pimentel M, Saad RJ, Long MD, Rao SSC. ACG clinical guideline: small intestinal bacterial overgrowth. Am J Gastroenterol. 2020;115(2):165–178. doi:10.14309/ajg.0000000000000505
- 2. Rezaie A, Buresi M, Lembo A, et al. Hydrogen and methane-based breath testing in gastrointestinal disorders: the North American consensus. Am J Gastroenterol. 2017;112(5):775–784. doi:10.1038/ajg.2017.46
- 3. Quigley EMM. The spectrum of small intestinal bacterial overgrowth (SIBO). Curr Gastroenterol Rep. 2019;21(1):3. doi:10.1007/s11894-019-0671-z
- 4. Dukowicz AC, Lacy BE, Levine GM. Small intestinal bacterial overgrowth: a comprehensive review. Gastroenterol Hepatol. 2007;3(2):112–122.
- 5. Rao SSC, Bhagatwala J. Small intestinal bacterial overgrowth: clinical features and therapeutic management. Clin Transl Gastroenterol. 2019;10(10):e00078. doi:10.14309/ctg.0000000000000078
- 6. Australian Institute of Health and Welfare (AIHW). Diabetes: Australian facts. Canberra: AIHW; 2023. Cat. no. CVD 84.
- 7. The Royal Australian College of General Practitioners (RACGP). Deprescribing proton pump inhibitors — evidence-based clinical practice guideline. East Melbourne: RACGP; 2023.
- 8. Shah SC, Day LW, Somsouk M, Sewell JL. Meta-analysis: antibiotic therapy for small intestinal bacterial overgrowth. Aliment Pharmacol Ther. 2013;38(8):925–934. doi:10.1111/apt.12479
- 9. Pimentel M, Constantino T, Kong Y, Bajwa M, Rezaei A, Park S. A 14-day course of rifaximin for the treatment of constipation-predominant irritable bowel syndrome. Am J Gastroenterol. 2006;101(1):326–333. doi:10.1111/j.1572-0241.2006.00399.x
- 10. Low K, Hwang L, Hua J, Zhu A, Morales W, Pimentel M. A combination of rifaximin and neomycin is most effective in treating irritable bowel syndrome patients with methane on lactulose breath test. J Clin Gastroenterol. 2010;44(8):547–550. doi:10.1097/MCG.0b013e3181c64c90
- 11. Jacobs C, Coss Adame E, Attaluri A, Valestin J, Rao SSC. Dysmotility and proton pump inhibitor use are independent risk factors for small intestinal bacterial overgrowth and its eradication. Aliment Pharmacol Ther. 2013;38(8):947–955. doi:10.1111/apt.12475
- 12. Gatta L, Scarpignato C. Systematic review with meta-analysis: rifaximin is effective and safe for the treatment of small intestine bacterial overgrowth. Aliment Pharmacol Ther. 2017;45(5):604–616. doi:10.1111/apt.13928
- 13. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework 2023 summary report. Canberra: AIHW; 2023.
- 14. Choung RS, Ruff KC, Malhotra A, et al. Clinical predictors of small intestinal bacterial overgrowth by duodenal aspirate culture. Aliment Pharmacol Ther. 2011;33(9):1059–1067. doi:10.1111/j.1365-2036.2011.04625.x