📋 Key Information Summary
- Inflammatory bowel disease (IBD) encompasses Crohn's disease (CD) and ulcerative colitis (UC), with an estimated 85 000 Australians affected and rising incidence, particularly in paediatric and adolescent populations.
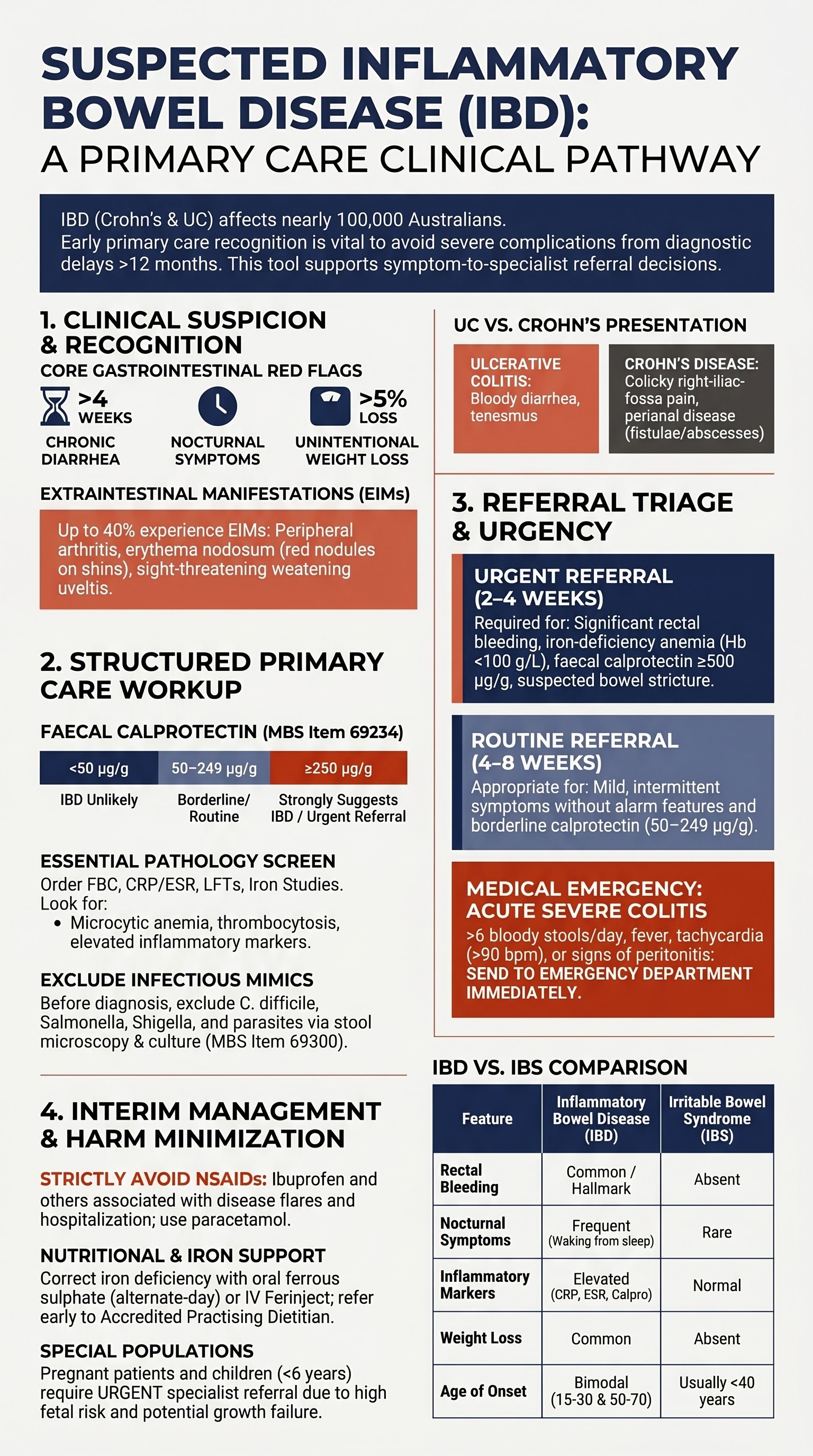
- Key clinical features suggesting IBD include chronic diarrhoea (>4 weeks), rectal bleeding, unintentional weight loss, nocturnal symptoms, and extraintestinal manifestations (arthritis, erythema nodosum, uveitis, oral aphthae).
- Red-flag features requiring urgent gastroenterology referral: significant or ongoing rectal bleeding, weight loss >5%, systemic symptoms (fever, tachycardia), iron-deficiency anaemia, suspected stricture or abscess, and failure of empirical therapy.
- First-line investigations in primary care include full blood count (FBC), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), faecal calprotectin, basic metabolic profile, liver function tests, iron studies, and stool microscopy/culture to exclude infection.
- Faecal calprotectin ≥250 µg/g in adults strongly suggests mucosal inflammation and warrants specialist referral; values of 50–249 µg/g require clinical correlation and repeat testing.
- Always exclude infectious causes of diarrhoea (Clostridioides difficile, Salmonella, Shigella, Campylobacter, parasites) before attributing symptoms to IBD.
- Avoid NSAIDs in suspected or confirmed IBD — they are associated with disease flares, GI ulceration, and IBD-related hospitalisation.
- Patients with significant bleeding, weight loss, systemic symptoms, or markers of inflammation should be referred as urgent (ideally seen within 2–4 weeks); those with milder or indolent presentations may be referred routinely.
- Interim management includes aggressive hydration, nutritional optimisation with dietitian input, iron supplementation (oral or IV) for iron-deficiency anaemia, and symptom control with loperamide only when infection has been excluded and colitis is not severe.
- Aboriginal and Torres Strait Islander Australians may present later with more aggressive disease; culturally safe care, point-of-care testing in remote communities, and engagement with Indigenous health workers are essential.
- Pregnant patients with suspected IBD require urgent referral as untreated active disease carries greater fetal risks than appropriate treatment; paediatric patients (especially <6 years) should be referred to paediatric gastroenterology.
- Definitive diagnosis requires ileocolonoscopy with biopsies and small-bowel imaging (MRI enterography); primary care role is recognition, initial workup, and timely referral — not endoscopic diagnosis.
Introduction & Australian Epidemiology
Inflammatory bowel disease (IBD) is a chronic, relapsing–remitting inflammatory condition of the gastrointestinal tract comprising two principal entities: Crohn's disease (CD) and ulcerative colitis (UC). A minority of patients (approximately 10–15%) are classified as IBD-unclassified (IBD-U) when colonic disease cannot be confidently categorised. IBD arises from a dysregulated immune response to gut microbiota in genetically susceptible individuals, modulated by environmental factors including diet, smoking, antibiotic exposure, and early-life events.
In Australia, IBD is a significant and growing health burden. Current estimates suggest approximately 85 000–100 000 Australians live with IBD, with the highest incidence and prevalence rates recorded in the Southern Hemisphere and comparable to Northern Europe and North America. Key Australian epidemiological data include:
- Incidence: Approximately 24–30 per 100 000 population per year for UC and 15–17 per 100 000 for CD.
- Prevalence: Estimated 0.4–0.7% of the Australian population, with projections suggesting continued increases over the coming decades.
- Age of onset: Bimodal, with a primary peak between ages 15–30 and a smaller secondary peak between 50–70 years. Paediatric-onset IBD (≤17 years) accounts for approximately 20–25% of new diagnoses.
- Geographic variation: Higher incidence in urban compared with rural settings; increasing incidence noted in migrants from low-prevalence regions after settling in Australia, supporting environmental triggers.
- Aboriginal and Torres Strait Islander Australians: Historically considered to have lower IBD rates, but emerging data suggest rising incidence and potential under-diagnosis due to healthcare access barriers, with later presentation and more complicated disease at diagnosis in some cohorts.
- Economic burden: The total annual cost of IBD in Australia has been estimated at over .7 billion, including direct healthcare costs, productivity losses, and carer burden (Crohn's & Colitis Australia, 2022).
The diagnosis of IBD is confirmed by specialist assessment including endoscopy with histopathology and cross-sectional imaging. However, the critical first step occurs in primary care — recognising suggestive clinical features, performing appropriate initial investigations, excluding infectious mimics, and initiating timely referral. Early diagnosis and treatment improve long-term outcomes, reduce complication rates (strictures, abscesses, fistulae in CD; toxic megacolon in UC), and decrease the need for surgery.
Clinical Features Suggesting IBD
IBD should be considered in any patient presenting with chronic or recurrent gastrointestinal symptoms, particularly when the clinical picture extends beyond simple functional bowel complaints. The clinical features differ somewhat between UC and CD but overlap significantly. A high index of suspicion is required, especially in younger patients with multiple symptom domains.
Core Gastrointestinal Symptoms
| Symptom | Crohn's Disease | Ulcerative Colitis | Clinical Significance |
|---|---|---|---|
| Chronic diarrhoea | Watery or loose; often with crampy abdominal pain | Frequent, small-volume, often bloody | >4 weeks duration warrants investigation; nocturnal diarrhoea is particularly suggestive of organic disease |
| Rectal bleeding | Less common unless colonic involvement | Present in >90% at diagnosis; hallmark feature | Any rectal bleeding >2 weeks or recurrent should prompt IBD screening; always consider and exclude colorectal malignancy in patients >40 years |
| Abdominal pain | Right iliac fossa most common; colicky, post-prandial | Diffuse or left-sided cramping; improves with defecation | Constant or severe pain may indicate stricture, abscess, or perforation — urgent evaluation |
| Weight loss | Common; reflects malabsorption and systemic inflammation | Less prominent unless severe disease | Unintentional weight loss >5% over 3–6 months is a red flag |
| Nocturnal symptoms | Nocturnal pain, waking to defecate | Nocturnal diarrhoea, urgency | Highly suggestive of organic pathology; functional disorders (IBS) rarely cause true nocturnal waking |
| Tenesmus / urgency | If rectal or perianal disease present | Very common with proctitis or left-sided colitis | Impacts quality of life significantly; indicates active mucosal inflammation |
| Perianal disease | Fissures, fistulae, abscesses, skin tags (25–35% at diagnosis) | Rare | Perianal disease in a young patient with diarrhoea is strongly suggestive of Crohn's disease |
Extraintestinal Manifestations (EIMs)
Extraintestinal manifestations occur in 25–40% of IBD patients and may precede, coincide with, or occur independently of gastrointestinal symptoms. Recognition of EIMs is important as they may be the presenting feature that prompts IBD investigation.
Features Distinguishing IBD from Irritable Bowel Syndrome (IBS)
IBS is far more prevalent than IBD in Australian primary care (~15% of the adult population). Overlap exists, but certain features favour organic disease:
- Any rectal bleeding (IBS does not cause bleeding)
- Nocturnal diarrhoea or pain waking the patient from sleep
- Unintentional weight loss
- Fever or systemic symptoms
- Iron-deficiency anaemia
- Elevated inflammatory markers (CRP, ESR, faecal calprotectin)
- Family history of IBD
- Extraintestinal manifestations (arthritis, skin lesions, eye inflammation)
- Onset after age 50 (IBS more likely to present before age 40)
Initial Primary Care Workup
When IBD is clinically suspected based on history and examination, a structured initial workup in primary care serves three purposes: (1) objectively assess for systemic and mucosal inflammation, (2) exclude infectious and other causes of symptoms, and (3) provide baseline data for the receiving specialist. Importantly, the primary care workup does not aim to confirm IBD — definitive diagnosis requires endoscopy and histopathology.
Recommended Investigations
Additional Investigations to Consider
- Coeliac serology (anti-tTG IgA + total IgA): Consider if CD is suspected or the patient has features of malabsorption; coeliac disease and IBD can coexist. Available in Australian laboratories; MBS item 66570.
- Thyroid function tests (TSH): To exclude hyperthyroidism as a cause of diarrhoea, particularly in younger women.
- HIV testing: If risk factors present or chronic diarrhoea remains unexplained; chronic diarrhoea may be an initial presentation of HIV enteropathy.
- Abdominal X-ray: May show dilated loops, faecal loading, or exclude toxic megacolon (colonic diameter >6 cm with systemic toxicity). Useful in acute presentations with significant abdominal pain. MBS item 57905.
Investigations Not Recommended at Primary Care Stage
- CT abdomen/pelvis: Not a first-line investigation for suspected IBD. Reserved for specialist-guided assessment of complications (abscess, stricture, fistula). Exposes to radiation; MRI enterography is preferred in younger patients.
- Colonoscopy in primary care: Should be performed by or arranged through a gastroenterologist. Primary care clinicians should not independently request endoscopy for IBD suspicion — referral to a gastroenterologist allows appropriate endoscopic planning with biopsies.
- pANCA and ASCA serology: Limited utility in primary care; sensitivity and specificity are insufficient for diagnostic purposes. May be requested by specialists in indeterminate cases.
Urgent vs Routine Referral
All patients with suspected IBD require gastroenterology assessment for definitive diagnosis and management planning. The urgency of referral is determined by the clinical severity, laboratory findings, and presence of red-flag features. Accurate triage ensures that patients with aggressive or complicated disease are seen promptly, while those with milder presentations are assessed within an appropriate timeframe.
- Significant or ongoing rectal bleeding
- Unintentional weight loss >5%
- Systemic features: fever >38°C, tachycardia, signs of sepsis
- Iron-deficiency anaemia (Hb <100 g/L or symptomatic)
- Faecal calprotectin ≥500 µg/g
- Significantly elevated CRP (>50 mg/L) with GI symptoms
- Suspected perianal fistula or abscess
- Clinical suspicion of stricture (crampy post-prandial pain, vomiting, distension)
- Young patient (<16 years) with suspected IBD
- Failure of empirical treatment with persistent symptoms >4–6 weeks
- Mild, intermittent symptoms without alarm features
- Faecal calprotectin 50–249 µg/g (borderline) with mild symptoms
- Mildly elevated CRP (5–50 mg/L) with chronic diarrhoea
- Family history of IBD with new GI symptoms (mild presentation)
- Chronic diarrhoea >6 weeks with normal or mildly abnormal bloods
- Mild extraintestinal features (arthralgia, aphthous ulcers) with GI symptoms
Writing an Effective Referral
To facilitate timely specialist triage, the referral should include:
- Duration and nature of symptoms (diarrhoea frequency, bleeding, weight loss)
- Nocturnal symptoms (waking from sleep)
- Extraintestinal features (joints, skin, eyes, mouth)
- Perianal symptoms (pain, discharge, skin tags)
- Smoking status (smoking worsens CD; protective in UC)
- Family history of IBD, coeliac disease, or colorectal cancer
- Current medications — especially NSAIDs, antibiotics, and oral contraceptive pill
- Results of FBC, CRP, ESR, faecal calprotectin, stool MCS
- Previous GI investigations (endoscopy reports, imaging)
- Any interim treatment commenced
Interim Symptom Management
While awaiting specialist review, primary care plays an essential role in supporting the patient, managing symptoms, correcting nutritional deficiencies, and preventing harm. The following measures are appropriate interim strategies that do not compromise subsequent specialist assessment.
1. Hydration & Fluid Management
Patients with chronic diarrhoea are at risk of dehydration and electrolyte disturbance, particularly the elderly and those with comorbidities.
- Encourage oral fluid intake of at least 2–2.5 L/day; water and oral rehydration solutions (ORS) are preferred.
- Commercial ORS solutions (Gastrolyte®, Hydrolyte®) are useful for patients with significant diarrhoea (>4 loose stools/day). Available OTC at Australian pharmacies.
- Avoid high-sugar carbonated beverages and excessive caffeine, which may worsen osmotic diarrhoea.
- Monitor for signs of dehydration: postural hypotension, reduced urine output, dry mucous membranes, confusion (elderly).
- Patients unable to maintain oral hydration or with signs of moderate–severe dehydration should be assessed for IV fluid resuscitation in an acute care setting.
2. Nutritional Optimisation
Malnutrition is common at IBD diagnosis (prevalence 20–50% depending on disease extent) and is associated with poorer outcomes, increased surgical complications, and reduced quality of life.
- Refer to an accredited practising dietitian (APD) early — ideally at the time of referral. MBS items 10950–10970 are available for patients with chronic disease management (CDM) plans (GP Management Plan, Item 721).
- Assess dietary intake with a brief food diary or validated screening tool (MUST — Malnutrition Universal Screening Tool, or the Malnutrition Screening Tool [MST]).
- Patients with significant weight loss or BMI <18.5 kg/m² should be flagged as nutritionally at risk.
- No specific dietary intervention has been proven to induce remission in IBD, but general recommendations include adequate protein intake (1.0–1.5 g/kg/day), micronutrient-rich foods, and avoidance of known dietary triggers during flares.
- Exclusive enteral nutrition (EEN) is a first-line induction therapy for paediatric CD and may be discussed with the specialist, but initiation is generally deferred to the gastroenterology team.
3. Medication Review — Avoid Harmful Agents
4. Iron Supplementation for Anaemia
Iron-deficiency anaemia affects 30–60% of IBD patients and contributes significantly to fatigue and reduced quality of life. Correction should be initiated in primary care where possible.
5. Symptom Monitoring & Safety Netting
Establish a clear safety-netting plan while the patient awaits specialist review:
- Advise the patient to return immediately if: bleeding worsens, new fever develops, pain becomes severe or constant, or they feel systemically unwell.
- Schedule a follow-up appointment at 2–4 weeks to review symptoms, check investigation results, and confirm referral status.
- Recheck FBC and CRP at 4–6 weeks if initially abnormal — assess for trajectory.
- If the patient has not been seen by the specialist within 8 weeks (routine referral), follow up and escalate the referral.
- Document the safety-netting advice and follow-up plan in the patient's record.
6. Psychosocial Support
A new diagnosis of suspected IBD can generate significant anxiety. Primary care should acknowledge the patient's concerns and provide support:
- Refer to Crohn's & Colitis Australia (crohnsandcolitis.com.au) for patient education resources, support groups, and a nurse helpline.
- Consider a mental health treatment plan (MBS item 721/723) if the patient reports significant anxiety or depression symptoms.
- Engage a GP Management Plan (Item 721) and Team Care Arrangement (Item 723) early to facilitate coordinated chronic disease management and access allied health services.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
IBD in Aboriginal and Torres Strait Islander Australians remains under-researched but is increasingly recognised as a significant health concern. Available data suggest that Indigenous Australians may present later, have more complicated disease at diagnosis, and experience greater barriers to accessing specialist gastroenterology services. Culturally safe, trauma-informed care is essential at every stage of the patient journey.
📚 References
- 1. Crohn's & Colitis Australia. The Economic Impact of Inflammatory Bowel Disease in Australia — 2022 Report. Melbourne: Crohn's & Colitis Australia; 2022.
- 2. Torres J, Mehandru S, Colombel JF, Peyrin-Biroulet L. Crohn's disease. Lancet. 2017;389(10080):1741–1755.
- 3. Ungaro R, Mehandru S, Allen PB, Peyrin-Biroulet L, Colombel JF. Ulcerative colitis. Lancet. 2017;389(10080):1756–1770.
- 4. Wilson J, Hair C, Knight R, et al. High incidence of inflammatory bowel disease in Australia: a prospective population-based Australian incidence study. Inflamm Bowel Dis. 2010;16(9):1550–1556.
- 5. D'Haens G, Sandborn WJ, Feagan BG, et al. A review of activity indices and efficacy end points for clinical trials of medical therapy in adults with ulcerative colitis. Gastroenterology. 2007;132(2):763–786.
- 6. van Rheenen PF, Van de Vijver E, Fidler V. Faecal calprotectin for screening of patients with suspected inflammatory bowel disease: diagnostic meta-analysis. BMJ. 2010;341:c3369.
- 7. Mowat C, Cole A, Windsor A, et al. Guidelines for the management of inflammatory bowel disease in adults. Gut. 2011;60(5):571–607.
- 8. Gastroenterological Society of Australia (GESA). Clinical Update: Inflammatory Bowel Disease. Melbourne: GESA; 2020.
- 9. National Institute for Health and Care Excellence (NICE). Crohn's disease: management [NG129]. London: NICE; 2019 (updated 2024).
- 10. National Institute for Health and Care Excellence (NICE). Ulcerative colitis: management [NG130]. London: NICE; 2019 (updated 2024).
- 11. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework: Summary report 2023. Canberra: AIHW; 2023.
- 12. Gearry RB, Richardson A, Frampton CMA, Collett JA, Burt MJ, Chapman BA, Barclay ML. High incidence of Crohn's disease in Canterbury, New Zealand: results of an epidemiologic study. Inflamm Bowel Dis. 2006;12(10):936–943.
- 13. Levine A, Koletzko S, Turner D, et al. ESPGHAN revised porto criteria for the diagnosis of inflammatory bowel disease in children and adolescents. J Pediatr Gastroenterol Nutr. 2014;58(6):795–806.
- 14. Royal Australian College of General Practitioners (RACGP). Guidelines for Preventive Activities in General Practice (Red Book). 9th edn. Melbourne: RACGP; 2018.
- 15. Torres J, Bonovas S, Doherty G, et al. ECCO guidelines on therapeutics in Crohn's disease: medical treatment. J Crohns Colitis. 2020;14(1):4–22.