📋 Key Information Summary
- Whipple's disease is a rare, chronic, multisystem infection caused by the gram-positive actinobacterium Tropheryma whipplei.
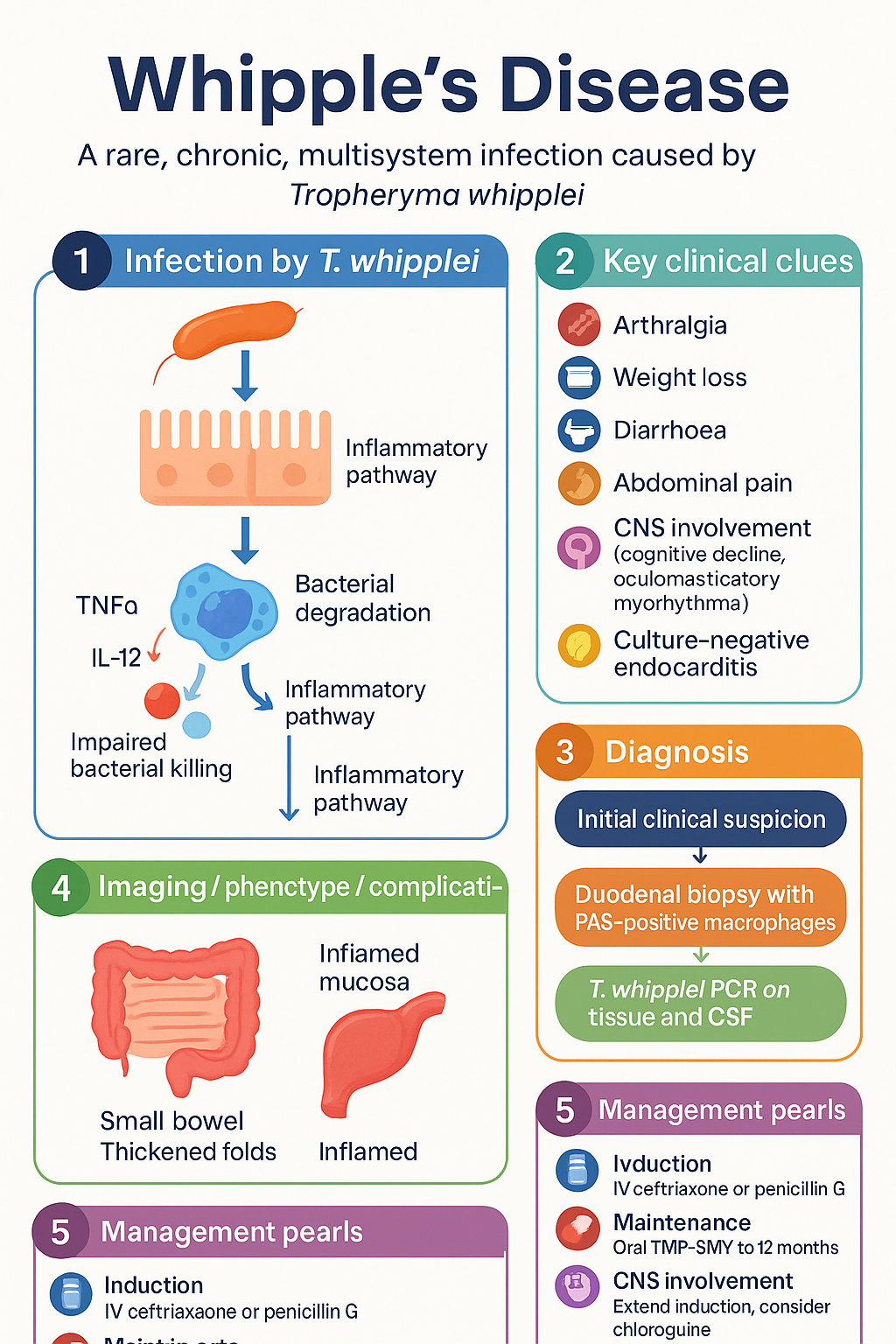
- Classic tetrad comprises arthralgia (often preceding GI symptoms by years), weight loss, diarrhoea, and abdominal pain.
- Extra-intestinal manifestations include CNS involvement (cognitive decline, oculomasticatory myorhythmia, supranuclear gaze palsy), culture-negative endocarditis, uveitis, and generalised lymphadenopathy.
- Diagnosis requires a high index of suspicion; duodenal biopsy with periodic acid-Schiff (PAS)-positive foamy macrophages remains the histological hallmark.
- T. whipplei PCR on tissue and CSF should be performed in all suspected cases; CSF analysis is mandatory even in the absence of neurological symptoms.
- Treatment consists of an induction phase with intravenous ceftriaxone (2 g IV daily) or penicillin G (4 MU IV q4h) for 2–4 weeks, followed by oral trimethoprim-sulfamethoxazole (TMP-SMX 160/800 mg BD) for 12 months.
- In patients with CNS involvement, induction should be extended and intravenous therapy chosen over oral; chloroquine or hydroxychloroquine may be added for CNS penetration.
- Immune reconstitution inflammatory syndrome (IRIS) may occur after initiation of antibiotics, particularly in immunosuppressed patients.
- Clinical and histological relapse monitoring is essential; repeat duodenal biopsy and PCR at 6, 12, and 24 months is recommended.
- Treatment is prolonged (≥12 months); premature cessation is the most common cause of relapse.
- Supportive care including nutritional supplementation, vitamin D and calcium replacement, and management of malabsorption is integral.
- Whipple's disease is notifiable in some jurisdictions; consult local public health units if culture-negative endocarditis or CNS manifestations are identified.
Clinical Features
Whipple's disease is a rare systemic infection caused by Tropheryma whipplei, an environmental gram-positive actinobacterium endemic worldwide. The disease predominantly affects middle-aged Caucasian males (male:female ratio approximately 4:1) and has a predilection for the gastrointestinal tract, joints, heart, and central nervous system. The interval between onset of arthralgia and diagnosis may span decades.
Classic Tetrad
The hallmark clinical presentation is characterised by four cardinal features, though not all may be present simultaneously:
- Arthralgia / arthritis: The most common presenting feature, occurring in >80% of cases. Typically a migratory, non-erosive, non-deforming polyarthralgia of large joints (knees, wrists, ankles). Arthritis may precede gastrointestinal symptoms by 5–10 years or longer and often responds transiently to NSAIDs.
- Weight loss: Progressive and often profound, reflecting malabsorption secondary to small bowel mucosal infiltration with PAS-positive macrophages.
- Diarrhoea: Chronic watery diarrhoea, occasionally steatorrhoeic, secondary to mucosal lymphatic obstruction and villous blunting. May be intermittent in early disease.
- Abdominal pain: Diffuse, cramping, and often postprandial; associated with mesenteric lymphadenopathy and intestinal wall thickening.
Extra-Intestinal Manifestations
T. whipplei can disseminate haematogenously to virtually any organ system. Extra-intestinal disease may occur in the absence of classic GI features.
Central Nervous System (CNS) Involvement
CNS Whipple's disease occurs in 10–40% of cases and portends a worse prognosis if not recognised early. Manifestations include:
- Cognitive and psychiatric change: Progressive dementia, personality change, memory impairment, confusion, and psychosis. These may be the sole presenting features in isolated CNS disease.
- Oculomasticatory myorhythmia: A pathognomonic movement disorder consisting of convergent–divergent pendular nystagmus synchronous with rhythmic contractions of the jaw (masticatory muscles). When present, this is essentially diagnostic of Whipple's disease.
- Supranuclear gaze palsy: Vertical gaze palsy mimicking progressive supranuclear palsy. This should prompt investigation for Whipple's disease, especially in younger patients.
- Other CNS features include hypothalamic dysfunction (polyuria, polydipsia, insomnia), ataxia, myoclonus, seizures, and cranial nerve palsies.
Culture-Negative Endocarditis
T. whipplei is an increasingly recognised cause of culture-negative infective endocarditis. Presentation may include fever, new or changing murmur, embolic phenomena, and heart failure. Diagnosis is typically made by valve tissue PCR. All patients presenting with culture-negative endocarditis should be considered for T. whipplei testing.
Ocular Involvement — Uveitis
Uveitis may be anterior, posterior, or pan-uveitis and can be the presenting feature. It may occur with or without concurrent systemic disease. Recurrent or refractory uveitis in middle-aged men should raise suspicion.
Lymphadenopathy
Generalised peripheral lymphadenopathy is common and may mimic lymphoma or other granulomatous diseases. Lymph node biopsy reveals PAS-positive macrophages. Mesenteric lymphadenopathy is particularly prominent and may be visible on CT imaging.
Other Manifestations
- Hyperpigmentation: Generalised skin darkening, particularly in sun-exposed areas.
- Seronegative polyarthritis: May mimic rheumatoid arthritis, reactive arthritis, or ankylosing spondylitis.
- Pleural/pericardial effusions: Due to lymphatic obstruction.
- Endocrine abnormalities: Adrenal insufficiency, hypogonadism from hypothalamic infiltration.
Diagnosis & Treatment
Diagnosis
Whipple's disease remains underdiagnosed due to its rarity and protean manifestations. A combination of histopathology, PCR, and clinical assessment is required for definitive diagnosis.
Histopathology — Duodenal Biopsy
- Gold standard: Oesophagogastroduodenoscopy (OGD) with biopsy of the second part of the duodenum.
- PAS staining: Duodenal mucosal biopsies reveal lamina propria infiltration with large, foamy macrophages containing PAS-positive, diastase-resistant intracellular granules. This is the histological hallmark of Whipple's disease.
- Villous blunting and lymphatic dilation may also be seen on haematoxylin and eosin staining.
- Histology alone may be insufficient in isolated CNS disease, where duodenal biopsies can be normal. PAS staining of CSF or brain biopsy tissue may be diagnostic.
T. whipplei PCR
- Tissue PCR: Should be performed on duodenal biopsy specimens to confirm T. whipplei DNA. This is particularly valuable when PAS staining is equivocal or when quantifying treatment response.
- CSF PCR: Mandatory in all patients at diagnosis, even if neurological symptoms are absent. Subclinical CNS involvement is present in a significant proportion of patients.
- Blood PCR: May be positive during active disease but has lower sensitivity than tissue PCR. Useful for monitoring treatment response.
- PCR testing is available at reference laboratories in Australia including state public health laboratories. MBS item 69496 (nucleic acid amplification) may be applicable.
CSF Examination
- Indication: CSF examination with cell count, protein, glucose, cytology, and T. whipplei PCR must be performed in every patient with confirmed or suspected Whipple's disease.
- Findings: Lymphocytic pleocytosis, elevated protein, and PAS-positive macrophages on cytospin preparation. PCR is the most sensitive CSF test.
- A normal CSF does not exclude future CNS relapse; long-term monitoring is required.
Treatment
Treatment is prolonged and must not be discontinued prematurely. The regimen consists of an intravenous induction phase followed by long-term oral maintenance therapy.
Induction Phase (2–4 Weeks)
Maintenance Phase (12 Months Minimum)
Adjunctive Therapy for CNS Disease
- Patients with proven or suspected CNS involvement should receive extended IV induction (4 weeks) followed by oral maintenance with TMP-SMX.
- If CSF PCR remains positive after initial IV therapy, consider adding hydroxychloroquine 200 mg PO BD to improve CNS drug penetration.
- Doxycycline 100 mg PO BD may be substituted or added as part of combination maintenance therapy for CNS disease.
- CNS involvement warrants a longer course of treatment — typically 12–24 months — guided by serial CSF PCR results.
Monitoring for Relapse and Immune Reconstitution Inflammatory Syndrome (IRIS)
Relapse Surveillance
Relapse occurs in up to 30% of patients and is most commonly due to premature discontinuation of therapy or inadequate CNS penetration.
- Clinical monitoring: Symptom review (arthralgia, diarrhoea, weight change, cognitive function) at 3-monthly intervals during therapy and for 2 years post-treatment.
- Histological monitoring: Repeat duodenal biopsy at 6 months, 12 months (end of therapy), and 24 months. Persistent PAS-positive macrophages or positive PCR indicates incomplete clearance.
- PCR monitoring: Tissue or blood PCR should be checked at 6 and 12 months. CSF PCR should be repeated at 12 months in patients with prior CNS involvement.
- Relapse management: Re-induction with IV ceftriaxone for 4 weeks followed by restart or modification of oral maintenance. Consider doxycycline-hydroxychloroquine combination if not already used.
Immune Reconstitution Inflammatory Syndrome (IRIS)
IRIS may occur after initiation of effective antibiotic therapy, particularly in patients who are immunosuppressed (e.g., concurrent corticosteroid use, HIV co-infection, biologic therapy). It is characterised by paradoxical worsening of symptoms due to an enhanced immune response to dying organisms.
- Features: New or worsening neurological symptoms (seizures, cognitive deterioration), fever, worsening lymphadenopathy, or new inflammatory lesions on imaging despite adequate antibiotic therapy.
- Management: Continue antibiotics; short course of corticosteroids (prednisolone 0.5–1 mg/kg/day, tapered over 2–4 weeks) may be considered in severe cases under infectious diseases supervision.
- Distinguish from treatment failure: IRIS is a diagnosis of exclusion; repeat PCR to confirm organism clearance. Persistent positive PCR suggests treatment failure or resistance rather than IRIS.
Supportive Care
- Nutritional support: Dietitian involvement is essential for patients with significant malabsorption. Consider oral nutritional supplements, and in severe cases, parenteral nutrition during induction therapy.
- Vitamin and mineral replacement: Vitamin D (cholecalciferol 1,000–2,000 IU daily), calcium (1,000–1,200 mg daily), iron (if iron deficiency anaemia present), vitamin B12, and folate supplementation as indicated by blood results.
- Bone health: DEXA scan should be considered due to chronic malabsorption and potential vitamin D deficiency. Bisphosphonate therapy if osteoporosis confirmed.
- Counselling and psychological support: Given the prolonged treatment course and potential for neurological sequelae, psychological support and patient education are important.
Management Timeline
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Marth T, Raoult D. Whipple's disease. Lancet. 2003;361(9353):239–246.
- 2. Fenollar F, Puéchal X, Raoult D. Whipple's disease. N Engl J Med. 2007;356(1):55–66.
- 3. Lagier JC, Lepidi H, Raoult D, Fenollar F. Systemic Tropheryma whipplei: clinical presentation of 142 patients with infections diagnosed or confirmed in a reference center. Medicine (Baltimore). 2010;89(5):337–345.
- 4. Gunther U, Moos V, Offenmuller G, et al. Gastrointestinal diagnosis of classical Whipple disease: clinical, endoscopic, and histopathologic features in 191 patients. Medicine (Baltimore). 2015;94(15):e714.
- 5. Dobbins WO III. Whipple's disease. Mayo Clin Proc. 1988;63(1):93–96.
- 6. Compain C, Samson S, Sellier P, et al. Central nervous system involvement in Whipple disease: clinical study of 18 patients and long-term follow-up. Medicine (Baltimore). 2013;92(6):324–330.
- 7. Gubler JG, Kuster M, Dutly F, et al. Whipple endocarditis without overt gastrointestinal disease: report of four cases. Ann Intern Med. 1999;131(2):112–116.
- 8. Williams OM, Cardiff L, Iyer A, et al. Tropheryma whipplei endocarditis: the UK national experience. Eur J Clin Microbiol Infect Dis. 2022;41(1):125–134.
- 9. Schneider T, Moos V, Loddenkemper C, et al. Whipple's disease: new aspects of pathogenesis and treatment. Lancet Infect Dis. 2008;8(3):179–190.
- 10. Feurle GE, Junga NS, Marth T. Efficacy of ceftriaxone or meropenem as initial therapies in Whipple's disease. Gastroenterology. 2010;138(2):478–486.
- 11. Lagier JC, Fenollar F, Raoult D. Acute infections caused by Tropheryma whipplei. Future Microbiol. 2017;12:247–254.
- 12. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework. Canberra: AIHW; 2023.
- 13. Royal Australian College of General Practitioners (RACGP). National guide to a preventive health assessment for Aboriginal and Torres Strait Islander people. 3rd ed. Melbourne: RACGP; 2018.