📋 Key Information Summary
- Non-acute lower GI bleeding (LGIB) encompasses intermittent rectal bleeding not associated with haemodynamic instability and managed predominantly in primary care across Australia.
- The most common causes of non-acute LGIB are haemorrhoids (internal and external), anal fissures, colonic diverticular disease, and inflammatory bowel disease (IBD).
- Risk stratification begins with distinguishing the character of bleeding — bright red blood on wiping or streaked on stool (typically anorectal) versus dark red blood mixed within stool (suggests a more proximal colonic source).
- Assess for haemodynamic stability (heart rate, blood pressure, postural symptoms) even in non-acute presentations to exclude covert significant haemorrhage.
- Alarm features mandating urgent referral include: age ≥45 years with new-onset bleeding, change in bowel habit, unintentional weight loss, iron deficiency anaemia, or a palpable abdominal/rectal mass.
- Initial primary care evaluation should include a thorough history (dietary and medication causes, personal and family history of colorectal neoplasia, IBD, diverticular disease), digital rectal examination (DRE), and consideration of in-office anoscopy.
- Baseline investigations include full blood count (FBC/CBC), serum ferritin, and iron studies to assess for iron deficiency anaemia — a red flag for colorectal malignancy until proven otherwise.
- Patients aged ≥45–50 years with rectal bleeding should be referred for colonoscopic evaluation in line with the Australian National Bowel Cancer Screening Program (NBCSP) age thresholds and RACGP recommendations.
- Faecal immunochemical test (FIT) is useful in risk stratification for colorectal cancer but does not replace colonoscopy in symptomatic patients with rectal bleeding.
- Iron deficiency anaemia in the context of LGIB requires both investigation of the GI tract (upper and lower endoscopy) and oral or intravenous iron replacement — PBS-listed ferrous sulfate 325 mg PO daily is first-line.
- Aboriginal and Torres Strait Islander peoples have higher rates of colorectal cancer and lower screening participation; culturally safe assessment, proactive screening engagement, and accessible referral pathways are essential.
- Patients with known haemorrhoids or fissures who develop new or changing bleeding patterns must be re-evaluated — never attribute rectal bleeding solely to known benign pathology without excluding malignancy, particularly in those aged ≥50 years.
Introduction & Australian Epidemiology
Lower gastrointestinal bleeding (LGIB) refers to any haemorrhage originating distal to the ligament of Treitz, encompassing sources in the colon, rectum, and anus. Non-acute LGIB — characterised by intermittent, self-limited episodes without haemodynamic compromise — is one of the most common presentations in Australian general practice. While the majority of cases are attributable to benign anorectal pathology, a clinically significant minority harbour serious underlying conditions including colorectal carcinoma, inflammatory bowel disease, and angiodysplasia.
In Australia, rectal bleeding is reported by approximately 10–15% of adults in community surveys, with haemorrhoidal disease affecting an estimated 30–40% of the adult population at some point in their lifetime. Diverticular disease is increasingly prevalent with age, found in over 40% of Australians aged >65 years on colonoscopic or imaging studies. Colorectal cancer remains the third most commonly diagnosed cancer in Australia (excluding non-melanoma skin cancer) and the second leading cause of cancer-related mortality, with approximately 15,500 new cases diagnosed annually according to the Australian Institute of Health and Welfare (AIHW, 2023).
The Australian National Bowel Cancer Screening Program (NBCSP), offering biennial faecal immunochemical testing (FIT) to eligible Australians aged 50–74 years, has improved early detection. However, symptomatic patients with rectal bleeding require clinical assessment beyond screening pathways. Prompt differentiation between benign and sinister causes in primary care is essential to ensure timely referral and reduce mortality from colorectal malignancy.
Risk Stratification
Risk stratification in non-acute LGIB serves two primary objectives: (1) to identify patients who can be safely managed in primary care with conservative measures, and (2) to detect features that warrant urgent or semi-urgent specialist referral. Even in the non-acute setting, systematic assessment is essential to avoid delayed diagnosis of serious pathology.
Character of Bleeding
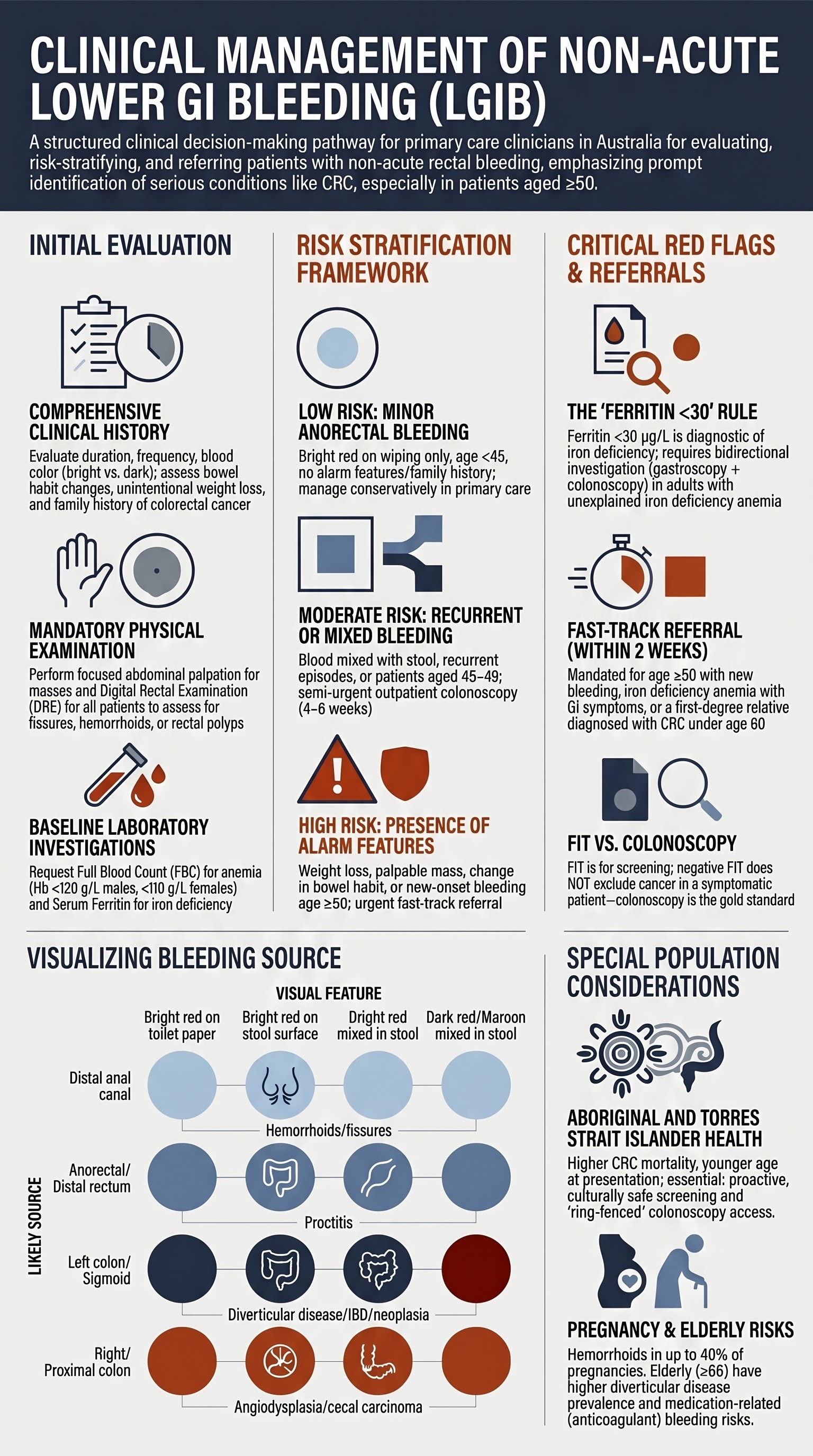
The appearance and pattern of bleeding provide important localising information:
| Feature | Likely Source | Typical Causes | Significance |
|---|---|---|---|
| Bright red blood on toilet paper only | Distal anal canal / perianal | External haemorrhoids, anal fissure, perianal dermatitis | Usually benign — manage in primary care if age <45 and no alarm features |
| Bright red blood on surface of formed stool | Anorectal / distal rectum | Internal haemorrhoids, rectal polyp, proctitis | Low–moderate concern; investigate if recurrent or age ≥45 |
| Bright red blood mixed into stool or in toilet bowl | Left colon / sigmoid / rectum | Diverticular disease, colorectal neoplasia, IBD, ischaemic colitis | Moderate–high concern; colonoscopy recommended |
| Dark red / maroon blood mixed with stool | Right colon / proximal colon | Angiodysplasia, right-sided diverticula, caecal carcinoma | High concern — colonoscopy indicated |
| Occult blood only (FIT positive, no visible bleeding) | Any colonic site | Polyps, colorectal cancer, angiodysplasia, NSAID-related mucosal injury | Significant — requires colonoscopic evaluation per NBCSP pathway |
Haemodynamic Assessment
Even in non-acute presentations, a focused haemodynamic assessment should be performed:
- Heart rate: Resting tachycardia (>100 bpm) may indicate occult blood loss or anxiety; compare with baseline if available.
- Blood pressure: Hypotension (systolic <100 mmHg) or postural hypotension (systolic drop ≥20 mmHg on standing) suggests significant volume depletion — consider acute LGIB pathway.
- Symptoms of anaemia: Fatigue, dyspnoea on exertion, dizziness, palpitations, or angina (in elderly patients) suggest chronic or subacute blood loss with resultant iron deficiency anaemia.
- Transfusion history: Previous requirement for blood transfusion in the context of GI bleeding indicates a high-risk patient.
Anxiety Symptoms
Patients presenting with non-acute rectal bleeding frequently express significant anxiety about the possibility of cancer. Acknowledging and addressing these concerns while pursuing appropriate investigation is an important component of patient-centred care. Conversely, patients who minimise or have normalised their bleeding — particularly those with a long history of "haemorrhoids" — require careful re-evaluation to ensure no change in pattern has occurred.
Initial Evaluation in Primary Care
The primary care evaluation of non-acute LGIB aims to identify likely benign causes, detect alarm features, and determine the need for and urgency of further investigation. A structured approach ensures that serious pathology is not missed.
History
A comprehensive history should address the following domains:
Bleeding Characteristics
- Duration and frequency of episodes (first episode vs. recurrent)
- Volume of blood loss (drops on paper vs. streaks vs. splashing in toilet bowl vs. clots)
- Colour: bright red (distal) vs. dark red/maroon (proximal)
- Relationship to defaecation — blood on wiping only, on stool surface, or mixed through stool
- Presence of mucus, pus, or faecal occult blood
- Associated symptoms: pain with defaecation (fissure), prolapsing mass (haemorrhoids), tenesmus (rectal pathology)
Bowel Habit
- Change in bowel habit — new constipation, diarrhoea, or alternating pattern (alarm feature for colorectal cancer)
- Narrow or ribbon-like stools (may indicate left-sided colonic obstruction)
- Straining at stool (associated with haemorrhoidal disease and fissures)
- Nocturnal symptoms — nocturnal diarrhoea or bleeding suggests organic rather than functional disease
Risk Factors for Serious Pathology
- Personal history: Colorectal polyps, colorectal cancer, IBD (Crohn's disease, ulcerative colitis), diverticular disease, previous colonoscopy findings
- Family history: First-degree relative with colorectal cancer (especially if diagnosed <60 years) — increases risk 2–4 fold
- Known haemorrhoids: Patients with a prior diagnosis of haemorrhoids who present with new or changed bleeding patterns require re-investigation
- Medications: Anticoagulants (warfarin, DOACs), antiplatelet agents (aspirin, clopidogrel), NSAIDs — these may exacerbate bleeding from an existing lesion and do not explain the underlying cause
- Systemic symptoms: Unintentional weight loss (>5% body weight in 6 months), fevers, night sweats, fatigue
Dietary and Benign Causes
- Exclude dietary causes of red-coloured stool: beetroot, dragon fruit (pitaya), tomatoes, red food colouring, certain medications (iron tablets cause black stool, not red; rifampicin may cause red discolouration)
- Constipation and straining — a very common precipitant of minor rectal bleeding from fissures and haemorrhoids
- Recent antibiotic use (associated with Clostridioides difficile colitis, though usually presents acutely)
Physical Examination
A focused examination in primary care should include:
- General assessment: Pallor (conjunctival, palmar), vital signs (HR, BP, postural measurements), signs of chronic disease
- Abdominal examination: Palpation for masses, tenderness, organomegaly; auscultation for bruits (rare, but may suggest mesenteric vascular disease)
- Digital rectal examination (DRE): Mandatory in all patients presenting with rectal bleeding. Assess for anal fissure, perianal skin tags, external haemorrhoids, rectal mass or polyp, and stool character (hard impacted stool, mucus, blood). Note: A normal DRE does not exclude significant proximal pathology.
Investigations
The following baseline investigations should be requested in primary care for all patients presenting with non-acute rectal bleeding:
Interpreting Iron Deficiency Anaemia in the Context of LGIB
Iron deficiency anaemia (IDA) in a patient with rectal bleeding is a significant finding that demands thorough investigation. In premenopausal women, menstrual blood loss is a common contributor and may coexist with GI pathology. In men and postmenopausal women, IDA in the setting of rectal bleeding is colorectal cancer until proven otherwise.
First-Line Management of Benign Causes (in Primary Care)
When investigation has excluded alarm features and a benign anorectal cause is confirmed:
Lifestyle and Conservative Measures
- Dietary fibre: Increase soluble and insoluble fibre intake to 25–30 g/day — dietary fibre supplements (psyllium husk, e.g., Metamucil®) are PBS-listed for some indications and available OTC
- Fluid intake: Adequate hydration (≥1.5–2 L water daily) to soften stool
- Toilet habits: Avoid prolonged straining; use a footstool to optimise anorectal angle; respond promptly to the urge to defaecate
- Sitz baths: Warm water baths for 10–15 minutes after defaecation can reduce anal sphincter spasm and promote healing in fissures
- Weight management: Obesity is an independent risk factor for haemorrhoidal disease and colorectal neoplasia
Referral for Colon Evaluation
Timely referral for colonoscopic evaluation is the cornerstone of managing non-acute LGIB when investigation extends beyond the anorectum or when alarm features are present. The threshold for referral should be low in Australian practice, reflecting the high incidence of colorectal cancer and the proven efficacy of early detection in reducing mortality.
Indications for Colonoscopy Referral
Colonoscopy is the gold standard investigation for evaluating the colonic mucosa. The following indications are based on RACGP, GESA, and Cancer Council Australia guidelines:
- Age ≥50 years with new-onset rectal bleeding
- Any age with iron deficiency anaemia and GI symptoms
- Unintentional weight loss with rectal bleeding
- Palpable rectal or abdominal mass
- Change in bowel habit (new constipation, diarrhoea, or looser stools lasting >6 weeks) with bleeding
- First-degree relative with CRC diagnosed <60 years + rectal bleeding at any age
- Age 45–49 years with rectal bleeding (even if likely benign)
- Recurrent rectal bleeding (>2 episodes) with no identified anorectal cause
- FIT-positive result via NBCSP pathway
- Mild iron deficiency (ferritin 15–30 µg/L) without anaemia, in the absence of other alarm features
Age Thresholds and the NBCSP
The Australian National Bowel Cancer Screening Program currently invites Australians for FIT at ages 50, 54, 55, 58, 60, 64, 68, 70, 72, and 74 years (expanding toward biennial screening for all 50–74 year olds). However, in a symptomatic patient with rectal bleeding, the NBCSP age threshold should not delay clinical investigation:
- Age ≥50 years with rectal bleeding: Refer for colonoscopy regardless of FIT result — do not wait for a screening FIT to become available
- Age 45–49 years with rectal bleeding: Given the rising incidence of early-onset colorectal cancer in Australia, a low threshold for colonoscopy referral is appropriate, particularly with any additional risk factor
- Age <45 years, single episode, clear anorectal cause on DRE: May be managed conservatively in primary care with safety-netting; refer if recurrent
Role of FIT in Symptomatic Patients
Faecal immunochemical testing (FIT) quantifies faecal haemoglobin concentration. In the screening (asymptomatic) population, FIT has a sensitivity of approximately 70–75% for colorectal cancer and is the basis of the NBCSP. However, in symptomatic patients:
- A negative FIT does not exclude colorectal cancer or significant colonic pathology — sensitivity drops in the symptomatic setting
- A positive FIT in a patient with rectal bleeding reinforces the need for colonoscopy but does not add diagnostic value beyond the indication already provided by the bleeding itself
- FIT may be most useful in patients with minor, intermittent bleeding where clinical uncertainty exists about whether bleeding is from an anorectal vs. colonic source — a high FIT result (>100 µg Hb/g) supports urgent colonoscopy
Preparing for the Referral
When referring for colonoscopy, the following information should accompany the referral to facilitate triage:
Alternative and Complementary Investigations
Patient Safety-Netting and Follow-Up
Regardless of the management plan, all patients should receive clear safety-netting advice:
- Return promptly if bleeding increases in volume or frequency
- Return if dark red or maroon blood develops (suggesting a more proximal source)
- Return if new symptoms develop: weight loss, change in bowel habit, abdominal pain, fatigue, dizziness
- Follow up within 4–6 weeks to confirm symptom resolution and review investigation results
- Patients managed conservatively should have a documented plan for reassessment and a clear timeframe for referral if symptoms persist beyond 4–6 weeks
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians experience a disproportionate burden of colorectal cancer compared with non-Indigenous Australians. According to the AIHW, Indigenous Australians are diagnosed with colorectal cancer at a younger age and often present at a later stage, contributing to higher mortality rates. Culturally safe, proactive, and community-embedded approaches are essential to improve outcomes.
📚 References
- 1. Australian Institute of Health and Welfare (AIHW). Cancer data in Australia. Cat. no. CAN 122. Canberra: AIHW; 2023.
- 2. Cancer Council Australia Colorectal Cancer Guidelines Working Party. Clinical practice guidelines for the prevention, early detection and management of colorectal cancer. Sydney: Cancer Council Australia; 2017. Available at: wiki.cancer.org.au/australiawiki/index.php?oldid=181103.
- 3. National Health and Medical Research Council (NHMRC). National bowel cancer screening program: modelling of the transition to biennial screening. Canberra: NHMRC; 2022.
- 4. Strate LL, Gralnek IM. ACG clinical guideline: management of patients with acute lower gastrointestinal bleeding. Am J Gastroenterol. 2016;111(5):712–721.
- 5. Oakland K, Chadwick G, East JE, et al. Diagnosis and management of acute lower gastrointestinal bleeding: guidelines from the British Society of Gastroenterology. Gut. 2019;68(5):776–789.
- 6. Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice (Red Book). 9th edn. Melbourne: RACGP; 2018.
- 7. Gastroenterological Society of Australia (GESA). Colonoscopy clinical care standards. Melbourne: GESA; 2020.
- 8. Young GP, Symonds EL, Allison JE, et al. Advances in colorectal cancer screening and diagnosis: the role of fecal immunochemical tests. Clin Gastroenterol Hepatol. 2022;20(3):479–489.
- 9. Australian Institute of Health and Welfare (AIHW). The health and welfare of Australia's Aboriginal and Torres Strait Islander peoples. Cat. no. IHW 230. Canberra: AIHW; 2023.
- 10. Con D, De Cruz P. Endoscopic evaluation and management of lower gastrointestinal bleeding. Aust Fam Physician. 2018;47(10):694–698.
- 11. Sengupta N, Tapper EB. Lower gastrointestinal bleeding: epidemiology and outcomes. Gastroenterol Clin North Am. 2022;51(1):1–13.
- 12. National Bowel Cancer Screening Program (NBCSP). Program overview and participation data. Australian Government Department of Health and Aged Care; 2024. Available at: www.health.gov.au/our-work/national-bowel-cancer-screening-program.
- 13. Goddard AF, James MW, McIntyre AS, Scott BB; British Society of Gastroenterology. Guidelines for the management of iron deficiency anaemia. Gut. 2011;60(10):1309–1316.