📋 Key Information Summary
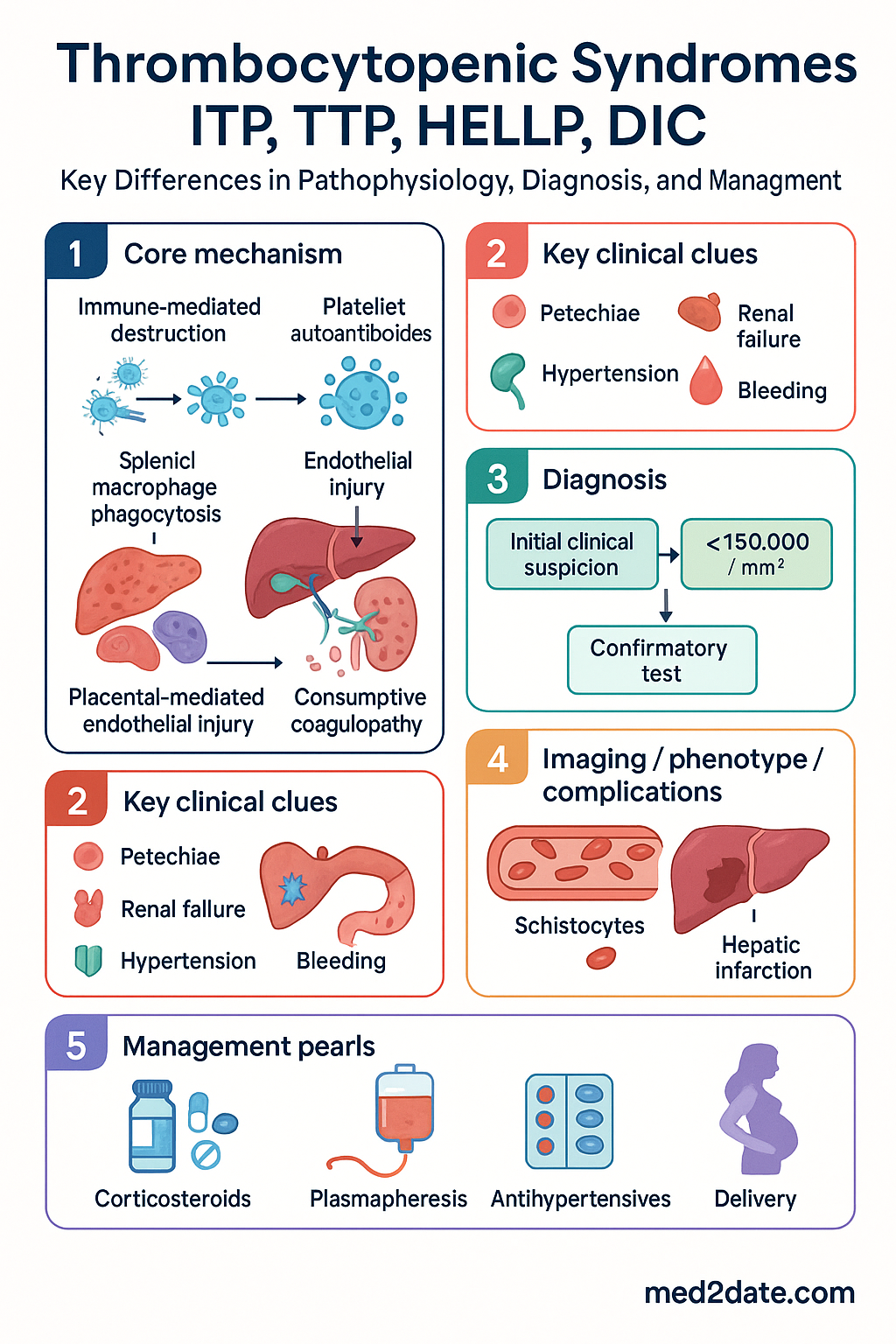
- ITP, TTP, HELLP, and DIC all cause thrombocytopenia but arise from fundamentally different pathophysiological mechanisms — immune-mediated destruction (ITP), thrombotic microangiopathy (TTP), placental-mediated endothelial injury (HELLP), and consumptive coagulopathy (DIC).
- Rapid differentiation is critical: TTP carries >90% mortality without urgent plasma exchange; ITP is rarely life-threatening acutely.
- Schistocytes on blood film are present in TTP, HELLP, and DIC but are absent in ITP — this is the single most important bedside differentiator.
- ADAMTS13 activity <10% confirms TTP and mandates emergency plasma exchange; coagulation studies (PT/INR, aPTT, fibrinogen) are typically normal in ITP and TTP but deranged in DIC.
- HELLP is a pregnancy-specific syndrome (typically >20 weeks' gestation) characterised by haemolysis, elevated liver enzymes, and low platelets — delivery is the definitive treatment.
- DIC is always secondary — identify and treat the underlying cause (sepsis, trauma, obstetric catastrophe, malignancy) while supporting coagulation.
- ITP diagnosis is one of exclusion: isolated thrombocytopenia with normal coagulation, no schistocytes, and no alternative explanation.
- TTP requires urgent plasma exchange (PLEX) initiated within 4–6 hours of clinical suspicion — do not wait for ADAMTS13 results.
- In obstetric thrombocytopenia, gestational thrombocytopenia (most common, 75%) must be distinguished from pre-eclampsia/HELLP, TTP, and ITP.
- DIC management centres on treating the precipitant; platelet transfusion threshold is <10 × 10⁹/L (or <50 × 10⁹/L with active bleeding).
- Aboriginal and Torres Strait Islander women experience higher rates of pre-eclampsia and HELLP syndrome — lower thresholds for specialist review are recommended.
- The PLASMIC score can risk-stratify for TTP at the bedside while awaiting ADAMTS13 results.
Introduction & Australian Epidemiology
Thrombocytopenic syndromes — immune thrombocytopenia (ITP), thrombotic thrombocytopenic purpura (TTP), haemolysis, elevated liver enzymes, low platelets (HELLP) syndrome, and disseminated intravascular coagulation (DIC) — share the common feature of a reduced platelet count but diverge profoundly in pathophysiology, clinical urgency, and management. Misidentification delays life-saving therapy, particularly plasma exchange for TTP or delivery for HELLP.
In Australia, ITP affects approximately 3–4 per 100,000 adults annually, with a bimodal distribution in young adults and the elderly. TTP incidence is approximately 3–5 per million per year; acquired TTP due to anti-ADAMTS13 autoantibodies predominates in adults, while Upshaw–Schulman syndrome (congenital) accounts for <5% of cases. HELLP complicates 0.5–0.9% of all pregnancies and 10–20% of severe pre-eclampsia presentations. DIC is not a primary diagnosis but a complication of severe sepsis (the most common cause in Australian ICUs), major trauma, obstetric emergencies (placental abruption, amniotic fluid embolism), and advanced malignancy.
This guideline provides a structured comparison to enable rapid differentiation and evidence-based management in Australian emergency, obstetric, and haematology settings.
Pathophysiology Comparison
Understanding the distinct mechanism of thrombocytopenia in each syndrome is essential for rational investigation and treatment.
| Feature | ITP | TTP | HELLP | DIC |
|---|---|---|---|---|
| Primary mechanism | Autoimmune IgG anti-platelet antibodies (GPIIb/IIIa, GPIb/IX) → Fc-mediated splenic destruction | Severe ADAMTS13 deficiency → uncleaved ultra-large vWF multimers → platelet-rich microthrombi | Placental endothelial injury → microangiopathic haemolysis + hepatic sinusoidal fibrin deposition | Widespread activation of coagulation → consumption of platelets, fibrinogen, clotting factors → microthrombi + haemorrhage |
| Coagulation cascade | Normal (PT, aPTT, fibrinogen) | Normal (PT, aPTT, fibrinogen) | Usually normal or mildly deranged | Markedly deranged — ↑PT/INR, ↑aPTT, ↓fibrinogen, ↑D-dimer |
| Schistocytes | Absent | Present (hallmark) | Present | Present |
| Haptoglobin | Normal | Low (consumed) | Low | Low |
| Fibrin deposition | No | Platelet-vWF microthrombi (no fibrin) | Hepatic sinusoidal fibrin | Widespread fibrin microthrombi |
| Key driver | Immune dysregulation | ADAMTS13 deficiency (autoimmune or congenital) | Placental pathology / pre-eclampsia spectrum | Systemic inflammatory response (tissue factor release) |
Clinical Context — Obstetric, Sepsis, and Autoimmune Settings
Obstetric Thrombocytopenia
Thrombocytopenia occurs in approximately 7–10% of pregnancies. The differential narrows by gestational age:
Sepsis-Associated DIC
DIC complicates 25–50% of sepsis admissions to Australian ICUs. Gram-negative bacteraemia (especially Escherichia coli, Neisseria meningitidis) and Staphylococcus aureus are common triggers. The ISTH DIC score (platelets, fibrinogen, D-dimer, PT prolongation) provides a rapid diagnostic framework.
Autoimmune / ITP Context
Primary ITP is a diagnosis of exclusion. Secondary ITP may occur in association with SLE, antiphospholipid syndrome (APS), CLL, H. pylori infection, hepatitis C, HIV, or post-vaccination. In APS, thrombocytopenia may paradoxically coexist with thrombosis — this mimics DIC but coagulation studies are normal. Drug-induced thrombocytopenia (heparin, quinine, valproate, vancomycin) must always be excluded.
Thrombotic Microangiopathy (TMA) Overlap
TTP, STEC-HUS, complement-mediated HUS, and HELLP all fall under the TMA umbrella. ADAMTS13 testing distinguishes TTP (ADAMTS13 <10%) from other TMAs. In pregnancy, the distinction between HELLP and TTP is critical because treatment differs fundamentally — delivery for HELLP versus plasma exchange for TTP.
Key Investigations to Differentiate
The following investigations, arranged by urgency, should be performed in all patients presenting with thrombocytopenia of uncertain aetiology.
Investigation Comparison Table
| Test | ITP | TTP | HELLP | DIC |
|---|---|---|---|---|
| Platelet count | ↓ (often <100) | ↓↓ (often <30) | ↓ (<100) | ↓ (variable) |
| Schistocytes | Absent | Present | Present | Present |
| PT/INR | Normal | Normal | Normal/mild ↑ | Prolonged |
| aPTT | Normal | Normal | Normal | Prolonged |
| Fibrinogen | Normal | Normal | Normal/elevated | Low |
| D-dimer | Normal | Mildly ↑ | ↑ | ↑↑↑ |
| LDH | Normal | ↑↑ | ↑↑ | ↑ |
| Haptoglobin | Normal | Low | Low | Low |
| AST/ALT | Normal | Normal/mild ↑ | ↑↑ (≥2× ULN) | Variable |
| ADAMTS13 | Normal | <10% | Normal/mild ↓ | Variable |
| Creatinine | Normal | Often ↑ | Often ↑ | Often ↑ |
Management Differences
Emergency Priorities by Syndrome
Pharmacotherapy Comparison
Platelet Transfusion Thresholds
| Syndrome | Transfusion Threshold | Rationale |
|---|---|---|
| ITP | Only for life-threatening haemorrhage (any count) | Rapid immune-mediated destruction; platelets may be consumed in <1 hour. Use IVIg to extend survival. |
| TTP | Contraindicated unless life-threatening bleeding or urgent surgery | May fuel microvascular thrombosis and worsen organ damage. |
| HELLP | <50 × 10⁹/L if delivery/C-section planned | Procedural safety for neuraxial anaesthesia and surgery. |
| DIC | <10 × 10⁹/L prophylactic; <50 × 10⁹/L with active bleeding | Consumptive loss; transfusion is supportive alongside cause-directed therapy. |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians experience disproportionate burden from conditions that cause thrombocytopenic syndromes, particularly hypertensive disorders of pregnancy and sepsis.
📚 References
- 1. Provan D, Arnold DM, Bussel JB, et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Advances. 2019;3(22):3780–3817.
- 2. Zheng XL, Vesely SK, Cataland SR, et al. ISTH guidelines for treatment of thrombotic thrombocytopenic purpura. J Thromb Haemost. 2020;18(10):2496–2502.
- 3. Practice Bulletin No. 222: Gestational Hypertension and Preeclampsia. Obstet Gynecol. 2020;135(6):e237–e260. (ACOG)
- 4. Levi M, Scully M. How I treat disseminated intravascular coagulation. Blood. 2018;131(8):845–854.
- 5. National Blood Authority Australia. Australian Patient Blood Management Guidelines — Module 5: Obstetrics and Maternity. Canberra: NBA; 2015 (updated 2019).
- 6. Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG). Management of Hypertension in Pregnancy. C-Obs 36. Melbourne: RANZCOG; 2023.
- 7. Bender L, Birch K, et al. RACGP Red Book — Investigation of bleeding and thrombocytopenia. In: RACGP Guidelines for Preventive Activities in General Practice. 9th ed. East Melbourne: RACGP; 2018.
- 8. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework 2020 — Maternal Health. Canberra: AIHW; 2022.
- 9. RHDAustralia (RHD Australia, ARF/RHD writing group). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Darwin: Menzies School of Health Research; 2020.
- 10. Bendapudi PK, Hurwitz S, Fry A, et al. Derivation and external validation of the PLASMIC score for rapid assessment of adults with thrombotic microangiopathies: a cohort study. Lancet Haematol. 2017;4(4):e157–e164.
- 11. Taylor FB, Toh CH, Hoots WK, Wada H, Levi M. Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation — ISTH Scientific Subcommittee on DIC. Thromb Haemost. 2001;86(5):1327–1330.
- 12. Scully M, Cataland SR, Peyvandi F, et al. Caplacizumab treatment for acquired thrombotic thrombocytopenic purpura. N Engl J Med. 2019;380(4):335–346.