📋 Key Information Summary
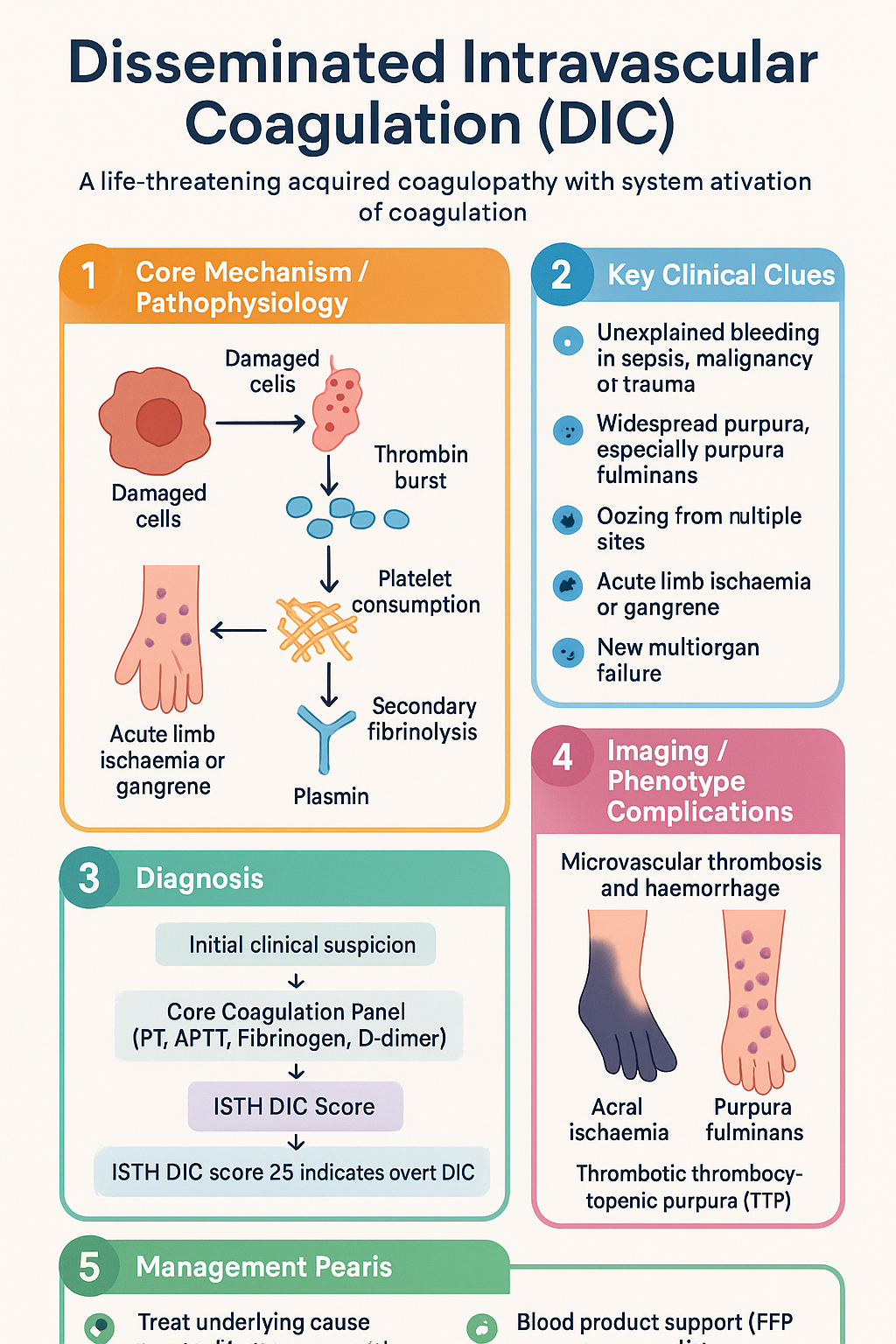
- Disseminated intravascular coagulation (DIC) is a life-threatening acquired coagulopathy characterised by systemic activation of coagulation leading to simultaneous microvascular thrombosis and consumptive haemorrhage.
- The most common trigger in Australia is severe sepsis (bacterial, viral, or fungal), followed by major trauma, obstetric emergencies, and advanced malignancy (especially acute promyelocytic leukaemia).
- The ISTH DIC score (platelets, fibrinogen, D-dimer, PT prolongation) is the recommended bedside scoring system — a score ≥5 is compatible with overt DIC and carries high mortality.
- Laboratory hallmarks: prolonged PT/APTT, falling fibrinogen, elevated D-dimer, schistocytes on blood film, and progressive thrombocytopaenia.
- Treat the underlying cause aggressively — source control in sepsis, delivery in placental abruption, chemotherapy in APL — as no blood product alone will resolve DIC.
- Transfuse FFP (15 mL/kg) for active bleeding with prolonged PT/APTT; cryoprecipitate (1 unit per 5–10 kg) to maintain fibrinogen ≥1.0 g/L (≥1.5 g/L if bleeding or pre-procedure).
- Transfuse platelets when count <50 × 10⁹/L with active bleeding, or <10 × 10⁹/L prophylactically; aim <100 × 10⁹/L before invasive procedures.
- Anticoagulation (heparin) may be considered in thrombotic-predominant DIC (e.g., purpura fulminans, APL) but is contraindicated in active haemorrhage.
- In septic DIC, early broad-spectrum antibiotics within 1 hour, haemodynamic resuscitation, and ICU admission are essential components of care.
- Obstetric DIC (abruption, amniotic fluid embolism, HELLP) requires coordinated obstetric–haematology–ICU management and early consideration of massive transfusion protocol activation.
- Aboriginal and Torres Strait Islander peoples have higher rates of sepsis-related DIC; ensure culturally safe care and timely transfer from remote settings.
- Serial laboratory monitoring (every 4–6 hours in acute DIC) guides blood product therapy; avoid prophylactic transfusion in non-bleeding patients with compensated DIC.
Introduction & Australian Epidemiology
Disseminated intravascular coagulation (DIC) is a serious acquired coagulopathy characterised by the systemic activation of coagulation pathways within the microvasculature. This leads to the paradoxical combination of widespread fibrin deposition (thrombosis) and consumption of clotting factors and platelets (haemorrhage). DIC is never a primary diagnosis — it is always secondary to an underlying condition that triggers the coagulation cascade.
In Australia, DIC is most frequently encountered in the context of severe sepsis and septic shock, accounting for approximately 30–50% of all DIC presentations to tertiary intensive care units. Other significant triggers include major polytrauma (particularly relevant given Australia's high burden of road traffic and agricultural injuries), obstetric emergencies, and haematological malignancies — notably acute promyelocytic leukaemia (APL, FAB M3).
The incidence of DIC in Australian ICUs is estimated at 8–12 per 1,000 ICU admissions, with in-hospital mortality ranging from 40–80% depending on the underlying aetiology and severity of organ dysfunction. Sepsis-related DIC carries a mortality of approximately 45–65%, while DIC associated with solid tumours or trauma has somewhat lower but still significant mortality (25–50%). The Australian Institute of Health and Welfare (AIHW) reports that sepsis-related hospitalisations have been rising at approximately 3–5% per year, which has implications for the frequency of DIC in clinical practice.
Early recognition, aggressive treatment of the triggering condition, and judicious blood product support remain the cornerstones of DIC management in Australian hospitals. This guideline provides a framework for the identification and management of DIC in primary haematology, emergency medicine, and intensive care settings across metropolitan, regional, and remote Australian healthcare facilities.
Pathogenesis & Triggers
DIC results from the unregulated systemic activation of the coagulation cascade, overwhelming the natural anticoagulant systems (antithrombin, protein C, tissue factor pathway inhibitor) and fibrinolytic capacity. The pathophysiology can be conceptualised in four overlapping phases.
Pathophysiological Mechanism
- Tissue factor exposure: Damaged or activated cells (monocytes, endothelium, tumour cells) express tissue factor (TF), which activates the extrinsic coagulation pathway via factor VII.
- Thrombin burst: Massive thrombin generation leads to widespread fibrin formation in the microvasculature, consuming fibrinogen, factor V, factor VIII, and other procoagulant factors.
- Platelet consumption: Platelets are activated and consumed in microthrombi, leading to progressive thrombocytopaenia.
- Secondary fibrinolysis: Plasminogen activation generates plasmin, cleaving fibrin and producing fibrin degradation products (FDPs) and D-dimer. In advanced DIC, excess plasmin can paradoxically worsen haemorrhage.
Major Triggers in Australian Practice
| Trigger Category | Common Causes | Mechanism | Approximate Frequency |
|---|---|---|---|
| Sepsis / Infection | Gram-negative bacteraemia, meningococcaemia, Staphylococcus aureus, Clostridium perfringens, malaria, COVID-19 | Endotoxin/cytokine-mediated TF expression on monocytes and endothelium | 30–50% |
| Malignancy | Acute promyelocytic leukaemia (APL), adenocarcinoma (pancreas, lung, prostate), mucin-secreting tumours | Cancer cell TF expression, chemotherapy-induced tumour lysis | 15–25% |
| Trauma | Major polytrauma, crush injuries, burns, traumatic brain injury, snake envenomation | Tissue damage, fat embolism, endothelial injury, shock-induced hypoperfusion | 10–20% |
| Obstetric | Placental abruption, amniotic fluid embolism, HELLP syndrome, retained dead fetus, eclampsia | Amniotic fluid/thromboplastin entry into maternal circulation | 5–10% |
| Vascular | Giant haemangiomas (Kasabach–Merritt), aortic aneurysm, large vessel aneurysms | Stasis, turbulent flow, endothelial activation | 2–5% |
| Other | Heat stroke, severe transfusion reaction, pancreatitis, liver failure, envenomation (brown snake, taipan) | Variable — toxin-mediated, immune-mediated | 5–10% |
Clinical Features — Bleeding & Thrombosis
DIC presents a clinical paradox: patients may bleed, thrombose, or — most commonly — exhibit features of both simultaneously. The dominant phenotype depends on the trigger and the balance between procoagulant activation and fibrinolysis.
- Oozing from venepuncture sites, cannulae, wounds
- Petechiae and purpura
- Gingival bleeding, epistaxis
- GI haemorrhage, haematuria
- Menorrhagia (in premenopausal women)
- Acral (digital) ischaemia and gangrene
- Purpura fulminans (skin necrosis)
- Deep vein thrombosis, pulmonary embolism
- Renal cortical necrosis (oliguria/anuria)
- Hepatic infarction, adrenal haemorrhagic necrosis
- Acute kidney injury (microvascular thrombosis)
- ARDS / respiratory failure
- Altered consciousness, seizures
- Shock liver (hepatic dysfunction)
- Adrenal haemorrhagic infarction (Waterhouse–Friderichsen syndrome)
Clinical Clues to DIC
- Unexplained bleeding in a patient with known sepsis, malignancy, or major trauma.
- Widespread purpura, especially purpura fulminans with skin necrosis.
- Oozing from multiple sites simultaneously (cannulae, wounds, mucosal surfaces).
- Acute limb ischaemia or gangrene in a patient with systemic illness.
- New multiorgan failure unresponsive to standard resuscitation.
- Schistocytes on peripheral blood film (microangiopathic haemolytic anaemia).
Investigations
Laboratory investigation is the cornerstone of DIC diagnosis. Serial testing is essential, as DIC is a dynamic process and a single set of results may not capture the full picture.
Core Coagulation Panel
Additional Investigations
ISTH DIC Scoring System
The International Society on Thrombosis and Haemostasis (ISTH) scoring system is the most widely validated tool for diagnosing overt DIC. It is simple, reproducible, and recommended by the Australian and New Zealand Society of Blood Transfusion (ANZSBT).
| Parameter | 0 Points | 1 Point | 2 Points | 3 Points |
|---|---|---|---|---|
| Platelet count (× 10⁹/L) | ≥100 | <100 | <50 | — |
| D-dimer (fibrin-related marker) | No increase | Moderate increase | Strong increase | — |
| Prolonged PT (seconds) | <3 s | 3–6 s | >6 s | — |
| Fibrinogen (g/L) | ≥1.0 | <1.0 | — | — |
Supportive Tests
- Blood cultures (at least 2 sets, including peripheral and any central lines) — essential in sepsis-triggered DIC.
- Lactate, blood gas, renal function, liver function — for organ dysfunction assessment.
- Peripheral blood film — look for schistocytes, which confirm microangiopathic process.
- Urinalysis — haematuria and proteinuria may indicate renal microvascular thrombosis.
- Imaging (CT, ultrasound) — as indicated for source control (abscess, effusion, thrombosis).
Risk Stratification & Severity Scoring
Beyond the ISTH score, several clinical and laboratory factors help predict outcome and guide the intensity of monitoring and intervention.
| Risk Factor | Poor Prognostic Indicator | Implication |
|---|---|---|
| ISTH DIC score | ≥7 (severe DIC) | Mortality >60%; requires ICU admission |
| SOFA score | ≥10 | Severe multiorgan dysfunction; consider goals-of-care discussion |
| Platelet trend | Falling >50% in 24 h or <20 × 10⁹/L | Active consumption; high bleeding risk |
| Fibrinogen | <0.5 g/L | Severe consumption; cryoprecipitate urgently required |
| Lactate | >4 mmol/L | Severe tissue hypoperfusion; aggressive resuscitation needed |
| Underlying cause | APL, septic shock, amniotic fluid embolism | Highest-mortality triggers; early specialist consultation essential |
When to Escalate
- ICU referral: All patients with overt DIC (ISTH ≥5) and organ dysfunction; any patient with DIC and haemodynamic instability.
- Haematology referral: APL or other haematological malignancy; unexplained DIC; DIC unresponsive to initial management; need for anticoagulation in DIC.
- Massive transfusion protocol (MTP): Activate when anticipated need exceeds 5 units of packed red blood cells within 4 hours, or any patient with DIC and life-threatening haemorrhage.
Management
DIC management has two pillars: (1) treat the underlying cause, and (2) supportive blood product replacement guided by laboratory results and clinical bleeding. No single therapy resolves DIC without addressing the trigger.
Step 1 — Treat the Underlying Cause
Step 2 — Blood Product Support
Transfusion in DIC should be goal-directed, guided by laboratory parameters and clinical bleeding. Prophylactic transfusion in non-bleeding patients does not improve outcomes and may worsen thrombosis.
Step 3 — Adjunctive & Emerging Therapies
Transfusion Triggers — Quick Reference
Monitoring
DIC is a dynamic process. Serial laboratory and clinical monitoring is essential to guide therapy and detect deterioration early.
Recommended Monitoring Schedule
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Levi M, Toh CH, Thachil J, Watson HG. Guidelines for the diagnosis and management of disseminated intravascular coagulation. British Journal of Haematology. 2009;145(1):24–33.
- 2. Taylor FB Jr, Toh CH, Hoots WK, Wada H, Levi M. Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thrombosis and Haemostasis. 2001;86(5):1327–1330.
- 3. Wada H, Thachil J, Di Nisio M, et al. Guidance for diagnosis and treatment of DIC from harmonization of the recommendations from three guidelines. Journal of Thrombosis and Haemostasis. 2013;11(4):761–767.
- 4. Australian Institute of Health and Welfare (AIHW). Sepsis in Australia. Cat. no. PHE 312. Canberra: AIHW; 2023.
- 5. National Blood Authority (NBA). Patient Blood Management Guidelines: Module 1 — Critical Bleeding / Massive Transfusion. Canberra: NBA; 2011.
- 6. National Blood Authority (NBA). Patient Blood Management Guidelines: Module 2 — Perioperative. Canberra: NBA; 2012.
- 7. CRASH-2 Collaborators. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. The Lancet. 2010;376(9734):23–32.
- 8. WOMAN Trial Collaborators. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. The Lancet. 2017;389(10084):2105–2116.
- 9. Squizzato A, Hunt BJ, Kinasewitz GT, et al. Supportive management strategies for disseminated intravascular coagulation. Thrombosis and Haemostasis. 2016;115(5):896–904.
- 10. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 11. Thachil J, Wada H, Gando S. DIC in the new millennium. Current Opinion in Hematology. 2022;29(5):230–237.
- 12. ISBT (International Society of Blood Transfusion) / ANZSBT. Guidelines for the administration of blood products. 3rd ed. 2022.
- 13. Brown AF, Lane DA. Anticoagulation in disseminated intravascular coagulation: current evidence and future directions. Internal Medicine Journal. 2020;50(4):401–408.
- 14. RHDAustralia (Australian Government Department of Health). Recommendations for managing acute rheumatic fever and rheumatic heart disease in Australia. 3rd ed. Darwin: Menzies School of Health Research; 2020.