📋 Key Information Summary
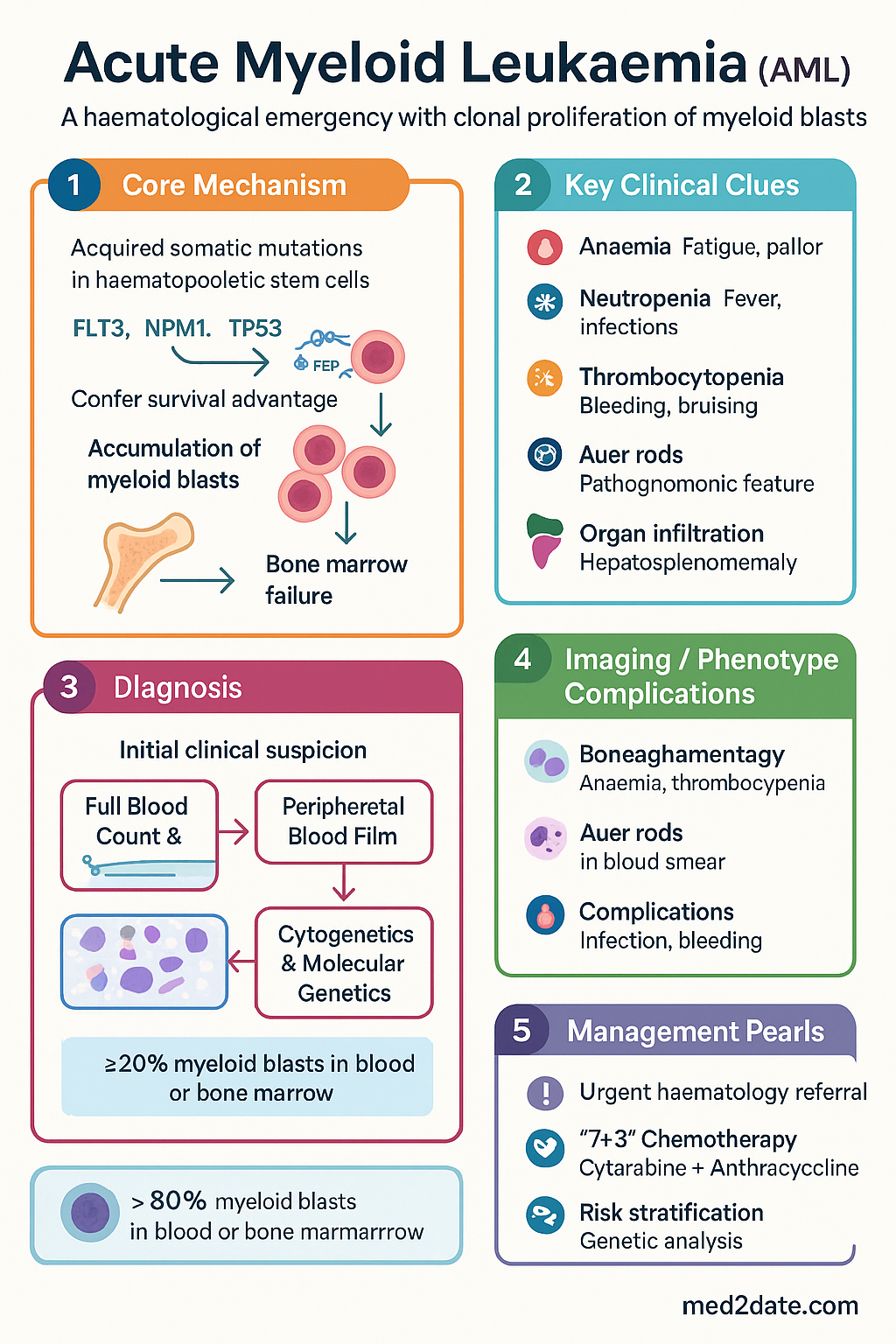
- Acute Myeloid Leukaemia (AML) is a haematological emergency characterised by clonal proliferation of myeloid blasts leading to bone marrow failure.
- Diagnosis requires ≥20% myeloid blasts in bone marrow or blood, with specific WHO classification subtypes.
- Presenting features include symptoms of anaemia, infection (neutropenia), and bleeding (thrombocytopenia); Auer rods are pathognomonic.
- Immediate management involves urgent referral to a haematology centre, supportive care, and risk stratification for treatment.
- Standard intensive induction for eligible patients is "7+3" chemotherapy: 7 days of continuous cytarabine infusion plus 3 days of an anthracycline.
- Post-remission therapy is stratified by genetic risk: favourable (consolidation chemotherapy), intermediate/adverse (allogeneic haematopoietic stem cell transplant).
- Molecular and cytogenetic analysis (e.g., FLT3, NPM1, TP53, core-binding factor translocations) is essential for risk classification and guiding therapy.
- Supportive care is paramount: broad-spectrum antibiotics for febrile neutropenia, blood product support, and tumour lysis prophylaxis.
- Special populations (elderly, those with comorbidities) may be considered for lower-intensity therapies like venetoclax with azacitidine.
- Aboriginal and Torres Strait Islander patients may face barriers to timely diagnosis and access to transplant; culturally safe care is critical.
- Long-term follow-up for survivors includes monitoring for late effects, particularly secondary malignancies and cardiovascular disease.
Introduction & Australian Epidemiology
Acute Myeloid Leukaemia (AML) is an aggressive, clonal haematopoietic malignancy characterised by the uncontrolled proliferation of immature myeloid precursors (blasts) in the bone marrow and peripheral blood. This leads to bone marrow failure, resulting in anaemia, thrombocytopenia, and neutropenia. AML is a medical emergency requiring prompt diagnosis and initiation of treatment.
In Australia, AML accounts for approximately 1,100 new diagnoses annually, with an age-standardised incidence of 4.2 per 100,000. The median age at diagnosis is 67 years. While it can occur at any age, incidence rises sharply after age 50. Outcomes remain poor, particularly for older adults and those with adverse-risk genetics, with 5-year overall survival rates around 30% for all patients combined. Management must be centralised in specialised haematology centres due to the complexity of therapy and high risk of treatment-related morbidity.
Pathogenesis & FAB Classification
AML arises from acquired somatic mutations in haematopoietic stem or progenitor cells. These mutations confer a survival and proliferative advantage, leading to the accumulation of arrested myeloid precursors (blasts) that fail to differentiate. The pathogenesis is often multi-hit, involving cooperating mutations in genes regulating cell proliferation (e.g., FLT3, KIT), differentiation (e.g., RUNX1, CEBPA), and epigenetic regulation (e.g., NPM1, DNMT3A, IDH1/2).
The French-American-British (FAB) classification (M0-M7) was historically used and is based on morphology and cytochemistry. It remains familiar in clinical practice but has been largely superseded by the World Health Organization (WHO) Classification (5th edition, 2022), which integrates morphology, genetics, and clinical features for more refined prognostication and treatment selection.
| FAB Subtype | Name | Key Features |
|---|---|---|
| M0 | Minimally differentiated | Blasts lack morphological and cytochemical myeloid features; requires immunophenotyping for diagnosis. |
| M1 | Without maturation | High blast percentage with minimal granulocytic maturation. |
| M2 | With maturation | Often associated with t(8;21) translocation; Auer rods may be present. |
| M3 | Acute promyelocytic leukaemia (APL) | t(15;17); associated with coagulopathy; specific all-trans retinoic acid (ATRA) therapy. |
| M4 | Myelomonocytic | Both myeloid and monocytic differentiation; may have inv(16). |
| M5 | Monocytic | High risk of tissue infiltration (gums, skin, CNS). |
| M6 | Erythroid | Predominantly erythroid precursors. |
| M7 | Megakaryoblastic | Often associated with Down syndrome in children. |
Clinical Features & Auer Rods
Presentation is typically rapid over weeks and directly results from bone marrow failure and organ infiltration.
- Symptoms of Anaemia: Fatigue, dyspnoea, pallor, tachycardia.
- Symptoms of Neutropenia: Fever, recurrent or severe infections (e.g., pneumonia, cellulitis, sepsis).
- Symptoms of Thrombocytopenia: Spontaneous bruising, petechiae, gingival bleeding, epistaxis, menorrhagia.
- Constitutional Symptoms: Fever, night sweats, weight loss, anorexia.
- Organ Infiltration: Hepatosplenomegaly, lymphadenopathy, bone pain, gingival hypertrophy (especially monocytic subtypes), skin infiltration (leukaemia cutis).
Investigations & Diagnosis
Urgent investigation is required. Diagnosis is established by the presence of ≥20% myeloid blasts in the peripheral blood or bone marrow, with specific exceptions for certain WHO-defined genetic subtypes (e.g., APL, AML with t(8;21), inv(16), which may have <20% blasts).
Management
All patients should be discussed at a multidisciplinary team meeting at a tertiary haematology centre. Management is stratified by patient fitness, age, and genetic risk.
1. Supportive Care (Immediate)
- Febrile Neutropenia: Immediate empirical IV broad-spectrum antibiotics (e.g., piperacillin-tazobactam) per local antibiogram. Refer to Australian Commission on Safety and Quality in Health Care (ACSQHC) standards.
- Transfusion Support: Irradiated, leucodepleted blood products. Platelet transfusion for active bleeding or prophylaxis (threshold often <10 x 10⁹/L).
- Tumour Lysis Prophylaxis: IV hydration, rasburicase or allopurinol, electrolyte monitoring.
- Fertility Counselling: Urgent referral for reproductive counselling before initiating gonadotoxic chemotherapy.
2. Intensive Induction Chemotherapy ("7+3")
For medically fit patients (typically <70-75 years with good performance status).
Expected outcome: Aplasia (nadir) at 7-14 days, with marrow recovery at 21-28 days. Day 14 marrow is performed to assess blast clearance. Complete remission (CR) is defined as <5% marrow blasts, count recovery, and no extramedullary disease.
3. Post-Remission (Consolidation) Therapy
Stratified by ELN 2022 genetic risk:
4. Allogeneic Haematopoietic Stem Cell Transplant (allo-HSCT)
The only curative option for intermediate and high-risk AML. Utilises donor-derived stem cells to provide a graft-versus-leukaemia effect. Requires HLA-matched sibling or unrelated donor, or haploidentical family donor. Conditioning regimens are myeloablative or reduced-intensity, tailored to patient age and comorbidities. Associated with significant risks of graft-versus-host disease, infection, and treatment-related mortality.
5. Lower-Intensity & Targeted Therapies
For patients not fit for intensive chemotherapy.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples may have a higher incidence of AML and poorer outcomes compared to non-Indigenous Australians. This disparity is influenced by complex social, economic, and historical factors.
📚 References
- 1. Döhner H, Wei AH, Appelbaum FR, et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood. 2022;140(12):1345-1377.
- 2. Khoury JD, Solary E, Abla O, et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia. 2022;36(7):1703-1719.
- 3. Cancer Australia. Acute Myeloid Leukaemia (AML) in Australia. Available at: [https://www.cancer.gov.au](https://www.cancer.gov.au) (Accessed: 2024).
- 4. Australian Institute of Health and Welfare (AIHW). Cancer in Australia 2021. AIHW, Canberra. 2021.
- 5. DiNardo CD, Jonas BA, Pullarkat V, et al. Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. N Engl J Med. 2020;383(7):617-629.
- 6. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2017.
- 7. Leukaemia Foundation. Understanding Acute Myeloid Leukaemia. Leukaemia Foundation, Australia. 2023.
- 8. Australasian Leukaemia & Lymphoma Group (ALLG). Clinical Trials. Available at: [https://allg.org.au](https://allg.org.au) (Accessed: 2024).
- 9. National Health and Medical Research Council (NHMRC). National Statement on Ethical Conduct in Human Research. 2023 Updated. Canberra: NHMRC.
- 10. Australian Indigenous HealthInfoNet. Summary of Aboriginal and Torres Strait Islander health. 2023. Available at: [https://healthinfonet.ecu.edu.au](https://healthinfonet.ecu.edu.au).