📋 Key Information Summary
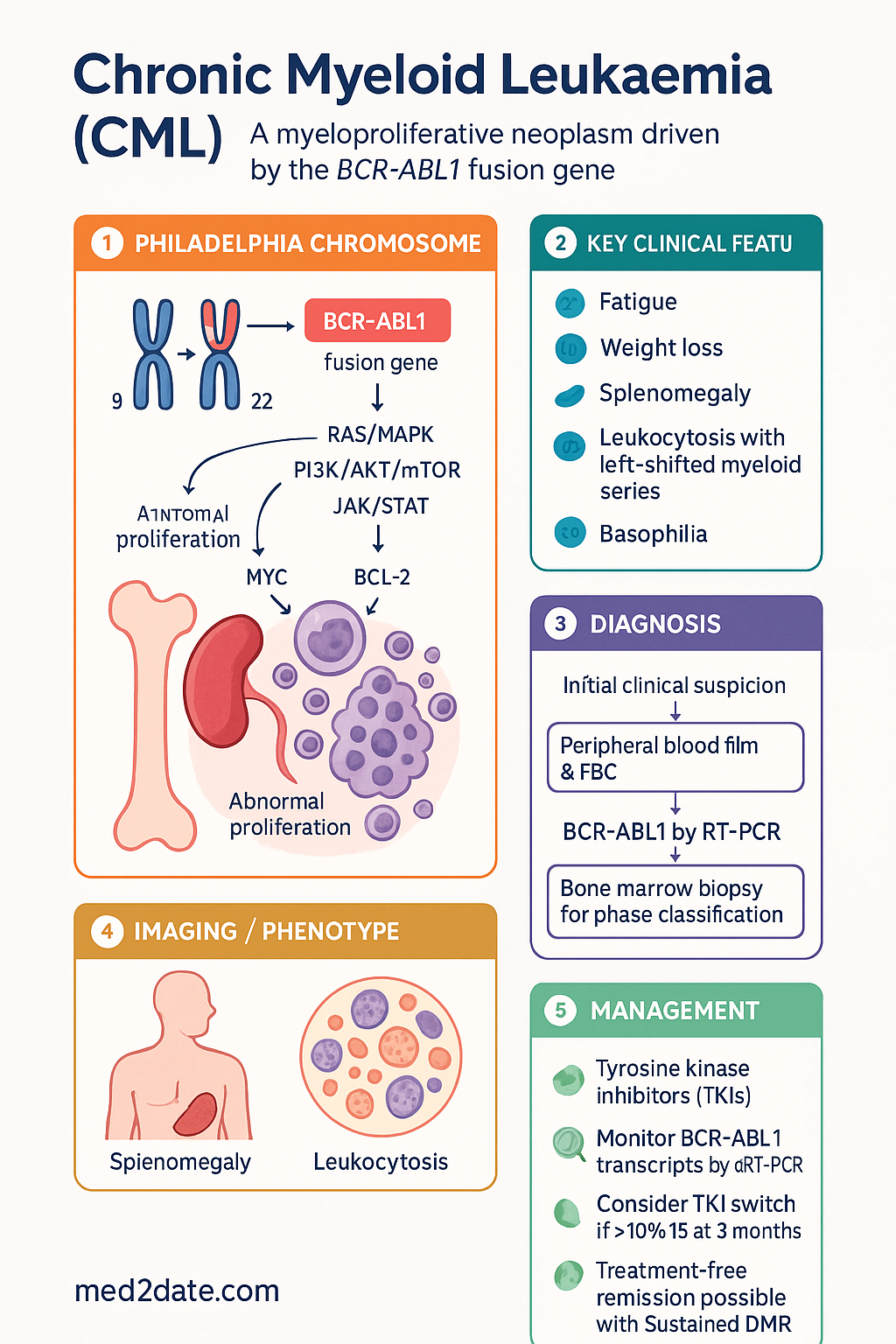
- Chronic myeloid leukaemia (CML) is a myeloproliferative neoplasm caused by the Philadelphia chromosome — the t(9;22) reciprocal translocation producing the BCR-ABL1 fusion gene encoding a constitutively active tyrosine kinase.
- The majority of patients (90–95%) present in chronic phase (CP); accelerated phase (AP) and blast phase (BP) represent disease progression and carry increasingly poor prognosis.
- Typical presenting features include fatigue, weight loss, splenomegaly, and leukocytosis with a characteristic left-shifted myeloid series and basophilia on peripheral blood film.
- Diagnosis requires demonstration of the Philadelphia chromosome by conventional cytogenetics or BCR-ABL1 by RT-PCR; bone marrow biopsy establishes baseline and phase classification.
- Tyrosine kinase inhibitors (TKIs) — imatinib (Glivec®) — transformed CML from a fatal disease to one with near-normal life expectancy for most CP-CML patients.
- Second-generation TKIs (dasatinib, nilotinib, bosutinib) are used as first-line therapy in higher-risk patients or as second-line options for imatinib resistance/intolerance.
- Third-generation TKI ponatinib (Iclusig®) is reserved for T315I-mutation or multi-TKI-resistant disease, requiring Authority PBS approval.
- Allogeneic stem cell transplantation (allo-SCT) remains curative but is now largely reserved for patients who fail multiple TKIs or present in blast phase.
- Response milestones — complete haematological response (CHR) at 3 months, major cytogenetic response (MCyR) at 6 months, complete cytogenetic response (CCyR) at 12 months, major molecular response (MMR or MR3) at 12–18 months — guide treatment decisions.
- BCR-ABL1 transcript monitoring by quantitative RT-PCR (IS) is the backbone of response assessment; values >10% IS at 3 months warrant TKI switch consideration.
- Treatment-free remission (TFR) is achievable in patients with sustained deep molecular response (DMR, MR4/MR4.5 for ≥2 years) under specialist supervision.
- All PBS-listed TKIs for CML are available as Restricted Benefit or Authority Required items; access is via haematologist initiation and PBS authority application.
- Aboriginal and Torres Strait Islander patients may face disparities in CML outcomes related to delayed presentation, limited specialist access in remote areas, and comorbidity burden.
Introduction & Australian Epidemiology
Chronic myeloid leukaemia (CML) is a clonal myeloproliferative neoplasm (MPN) characterised by the presence of the Philadelphia (Ph) chromosome — the reciprocal translocation t(9;22)(q34;q11) — which generates the BCR-ABL1 fusion oncogene. This fusion gene encodes a constitutively active tyrosine kinase that drives uncontrolled proliferation of the granulocytic lineage, leading to accumulation of maturing and mature myeloid cells in blood, bone marrow, and extramedullary sites. The introduction of tyrosine kinase inhibitors (TKIs) in 2001 marked one of the most dramatic paradigm shifts in oncology, transforming CML from a disease with a median survival of 3–5 years to one in which most patients can expect a near-normal life expectancy.
Epidemiology in Australia
CML accounts for approximately 15% of all leukaemias in adults. In Australia, the age-standardised incidence is approximately 1.2–1.6 per 100,000 population per year, with an estimated 300–350 new diagnoses annually. The median age at diagnosis is 55–60 years, though CML can present at any age, including in paediatric patients. The incidence is slightly higher in males (M:F ratio approximately 1.4:1). Environmental risk factors are limited; prior exposure to ionising radiation is the only well-established risk factor. Most cases arise de novo without identifiable predisposing factors.
Australia's TKI access programme through the Pharmaceutical Benefits Scheme (PBS) ensures that all eligible patients can access first- and second-line TKIs at subsidised cost. The Australian CML Registry and national haematology networks (including the Australasian Leukaemia & Lymphoma Group — ALLG) have contributed significantly to international CML outcome data, confirming that Australian CML survival rates are comparable to or exceed global benchmarks.
Aboriginal and Torres Strait Islander Australians may have lower incidence of CML but are more likely to present at advanced stage and have reduced access to haematology specialists in remote and very remote regions of Australia. Tailored pathways and Telehealth-supported care are critical to closing outcome gaps.
Pathogenesis & BCR-ABL
The Philadelphia Chromosome
The hallmark of CML is the Philadelphia (Ph) chromosome — the product of a balanced reciprocal translocation between chromosomes 9 and 22: t(9;22)(q34;q11). This translocation juxtaposes the ABL1 proto-oncogene (from 9q34) with the BCR gene (from 22q11), creating a novel fusion gene BCR-ABL1 on the derivative chromosome 22q−. The Ph chromosome is present in >95% of CML patients; a minority harbour cryptic or variant translocations detectable only by fluorescence in situ hybridisation (FISH) or RT-PCR.
BCR-ABL1 Fusion Variants
The breakpoint in the BCR gene determines the size of the fusion protein:
| Transcript | Breakpoint | Protein | Frequency in CML | Clinical Relevance |
|---|---|---|---|---|
| e13a2 (b2a2) | Major breakpoint cluster region (M-bcr) | p210 | ~60% | Classic CML; used for qRT-PCR monitoring |
| e14a2 (b3a2) | M-bcr | p210 | ~35–40% | Classic CML; slightly better TKI responses reported |
| e19a2 | Micro-bcr (μ-bcr) | p230 | <1% | Rare; may present with neutrophilic CML |
| e1a2 | Minor breakpoint cluster region (m-bcr) | p190 | ~1–2% | Typically ALL; if in CML, may indicate monocytic differentiation |
Oncogenic Mechanism
The BCR-ABL1 fusion protein has constitutive tyrosine kinase activity that activates multiple downstream signalling pathways:
- RAS/MAPK pathway — drives proliferation and differentiation arrest of myeloid progenitors.
- PI3K/AKT/mTOR pathway — promotes survival and anti-apoptotic signalling.
- JAK/STAT pathway — supports cytokine-independent growth.
- MYC and BCL-2 upregulation — sustains clonal expansion.
The net effect is expansion of a pluripotent haematopoietic stem cell clone with increased but not unlimited self-renewal capacity, explaining the chronic phase of the disease. Accumulation of additional genetic abnormalities (trisomy 8, isochromosome 17q, additional Ph chromosome, RUNX1, TP53 mutations) drives progression to accelerated and blast phases.
TKI Targeting of BCR-ABL1
TKIs competitively bind the ATP-binding pocket of the BCR-ABL1 kinase domain, blocking autophosphorylation and downstream signalling. Imatinib was the first TKI and binds in the inactive (DFG-out) conformation. Second-generation TKIs (dasatinib, nilotinib, bosutinib) have higher potency and can bind in active or inactive conformations, conferring activity against many (but not all) imatinib-resistant mutants. Ponatinib, a third-generation TKI, was designed to overcome the gatekeeper T315I mutation that confers resistance to all earlier TKIs.
Clinical Features & Blood Film
Presentation in Chronic Phase
Approximately 40–50% of patients are asymptomatic at diagnosis, with CML detected incidentally on a routine full blood count (FBC). When symptomatic, the presentation is insidious and includes:
- Constitutional symptoms: Fatigue, weight loss, night sweats, anorexia.
- Splenomegaly: Present in 50–70% at diagnosis; may cause left upper quadrant discomfort, early satiety, or splenic infarction.
- Hepatomegaly: Less common than splenomegaly; present in ~15%.
- Hypermetabolic symptoms: Bone pain, gout from hyperuricaemia, priapism (rare).
- Bleeding or thrombosis: Uncommon in CP; may reflect extreme thrombocytosis or platelet dysfunction.
Full Blood Count Findings
| Parameter | Typical Finding at Diagnosis | Notes |
|---|---|---|
| WCC | Markedly elevated, often 50–300 × 10⁹/L | Can exceed 500 × 10⁹/L; correlates with splenic size |
| Differential | Left-shifted myeloid series; increased myelocytes, metamyelocytes | Myelocyte peak is characteristic; blasts <5% in CP |
| Basophils | Absolute basophilia (often >5%, sometimes >20%) | Basophilia >20% in AP criteria; an important disease marker |
| Eosinophils | Frequently elevated | Part of the pan-myeloid expansion |
| Haemoglobin | Usually normal or mildly reduced | Anaemia at presentation suggests AP/BP or unrelated cause |
| Platelets | Normal, elevated (sometimes >1000 × 10⁹/L), or mildly reduced | Thrombocytopenia at diagnosis is a poor prognostic sign |
| LDH | Elevated | Reflects tumour burden and cell turnover |
| Uric acid | Frequently elevated | Risk of tumour lysis with rapid cell reduction |
Peripheral Blood Film
The blood film in CML has several characteristic features that can suggest the diagnosis before cytogenetic confirmation:
- Leukoerythroblastic picture: Immature myeloid cells (promyelocytes, myelocytes, metamyelocytes) and occasional nucleated red cells.
- Myelocyte peak: Myelocytes often exceed metamyelocytes — the so-called "CML hump" on the differential.
- Basophilia: Readily visible basophils; often more prominent than expected.
- Platelet morphology: Large platelets may be present; megakaryocyte fragments occasionally seen.
- Absence of significant dysplasia: Unlike MDS/MPN overlap syndromes, CML cells mature relatively normally.
- Blasts: Should be <5% in chronic phase; ≥10% suggests accelerated phase, ≥20% defines blast phase.
Diagnosis & Staging (Phases)
Diagnostic Work-Up
The diagnosis of CML requires demonstration of the BCR-ABL1 fusion gene. The following investigations should be performed at baseline:
Phase Classification (2022 WHO / ICC Criteria)
| Feature | Chronic Phase (CP) | Accelerated Phase (AP) | Blast Phase (BP) |
|---|---|---|---|
| Blasts (blood + marrow) | <10% | 10–19% | ≥20% |
| Basophils (blood) | <20% | ≥20% | Any |
| Platelets | Normal or ↑ | <100 × 10⁹/L (unrelated to therapy) or >1000 × 10⁹/L unresponsive | Any |
| Additional cytogenetic abnormalities | None or minor | ACA in clonal evolution (trisomy 8, i(17q), +Ph, +19) | ACA may be present |
| Extramedullary disease | No | Granulocytic sarcoma possible | Yes; may have CNS or other extramedullary blast infiltration |
| Morphology | Mature differentiation | Increasing dysplasia, clusters of small megakaryocytes | Myeloid (60%), lymphoid (20–30%), mixed |
Prognostic Scoring Systems
Variables: age, spleen size (cm below costal margin), platelet count, peripheral blood blasts (%).
Low risk: Consider imatinib first-line.
Intermediate/high risk: Consider second-generation TKI (dasatinib or nilotinib) first-line for deeper/faster responses.
Management (Imatinib, Nilotinib, Dasatinib, SCT)
First-Line TKI Therapy — Chronic Phase
TKI therapy is the standard of care for all patients with CP-CML. The choice of first-line TKI is based on risk stratification, comorbidities, patient preference, and drug interaction profile.
Treatment Response Milestones (ELN 2020)
Response to TKI therapy is assessed at defined time points using BCR-ABL1 quantitative RT-PCR (International Scale) and, in some cases, cytogenetics:
| Time Point | Optimal Response | Warning | Failure |
|---|---|---|---|
| Baseline | — | High-risk (ELTS); ACA | — |
| 3 months | BCR-ABL1 ≤10% IS | >10% IS | No CHR or >95% Ph+ (if tested) |
| 6 months | BCR-ABL1 ≤1% IS | 1–10% IS | >10% IS or Ph+ >35% |
| 12 months | BCR-ABL1 ≤0.1% IS (MMR/MR3) | >0.1–1% IS | >1% IS or Ph+ >0% |
| Then every 3 months | MMR or better | Loss of MMR; rising transcript | Loss of CHR, CCyR, or confirmed MMR loss; mutations |
Management of Accelerated & Blast Phase
Accelerated phase (AP) and blast phase (BP) require more aggressive strategies:
- AP-CML: TKI therapy (second-generation preferred) with the goal of returning to chronic phase; allo-SCT should be discussed early.
- BP-CML: If myeloid blast crisis — TKI + AML-type induction chemotherapy (e.g., cytarabine + anthracycline). If lymphoid blast crisis — ALL-type induction (e.g., hyper-CVAD) + TKI. Allo-SCT is the only potentially curative option and should be pursued in fit patients once second chronic phase is achieved.
- Ponatinib has particular efficacy in advanced-phase CML and should be considered early in BP.
Allogeneic Stem Cell Transplantation
Allo-SCT was the standard curative therapy before TKIs and remains an important option for selected patients:
- Current indications: Failure of ≥2 TKIs; T315I mutation (if ponatinib unavailable or contraindicated); blast phase CML; patients with compound mutations resistant to all available TKIs.
- Donor source: Matched sibling donor preferred; matched unrelated donor, haploidentical, or cord blood are alternatives. Australian Bone Marrow Donor Registry (ABMDR) facilitates unrelated donor searches.
- Conditioning: Reduced-intensity conditioning (RIC) increasingly used given older age of many CML patients.
- Outcomes: 3-year OS approximately 50–70% for CP-CML post-TKI failure; worse for advanced phases.
- Post-SCT: TKI may be used as maintenance post-transplant if molecular relapse occurs; donor lymphocyte infusion (DLI) is an alternative for relapse.
Treatment-Free Remission (TFR)
Selected patients with deep, sustained molecular responses may be candidates for supervised TKI cessation:
- Eligibility: CP-CML treated with TKI for ≥5 years; sustained MR4 (BCR-ABL1 ≤0.01% IS) or MR4.5 (≤0.0032% IS) for ≥2 years; access to reliable qRT-PCR.
- Monitoring: qRT-PCR monthly for 6 months, then every 2–3 months for at least 5 years (some centres continue indefinitely).
- Outcome: Approximately 40–60% maintain undetectable molecular residual disease (UMRD); 30–50% experience molecular relapse (loss of MMR) and require TKI re-initiation — typically with rapid return to DMR.
- Withdrawal symptoms: Musculoskeletal pain (TKI withdrawal syndrome) occurs in 20–30% of patients stopping imatinib; usually self-limiting.
Monitoring & Long-Term Follow-Up
Molecular Monitoring
Quantitative BCR-ABL1 RT-PCR on the International Scale (IS) is the primary tool for monitoring TKI response. Testing should be performed:
- Every 3 months until MMR (≤0.1% IS) is achieved, then every 3 months for the first 3 years.
- Every 3–6 months thereafter in stable responders.
- Monthly during TFR.
- Any confirmed >1-log increase in transcript level should prompt mutation testing and clinical reassessment.
Australian laboratories participating in the international BCR-ABL1 standardisation programme ensure results are comparable across centres. MBS Item 73304 covers quantitative BCR-ABL1 monitoring.
Laboratory Monitoring for TKI Toxicity
| Test | Frequency | Relevance |
|---|---|---|
| FBC with differential | Weekly × 1 month → fortnightly × 2 months → monthly → 3-monthly | Cytopenias (all TKIs); monitor for disease progression |
| LFTs (ALT, AST, bilirubin) | Monthly × 3 months → 3-monthly | Hepatotoxicity (imatinib, nilotinib) |
| Lipid profile | Baseline, 3-monthly on nilotinib | Nilotinib-associated dyslipidaemia and accelerated atherosclerosis |
| Fasting glucose / HbA1c | Baseline, 3–6-monthly on nilotinib | Hyperglycaemia with nilotinib |
| ECG (12-lead) | Baseline, day 3 & 7 with nilotinib; as clinically indicated with dasatinib | QTc prolongation (nilotinib); pleural effusion screening (dasatinib) |
| CXR | If respiratory symptoms on dasatinib | Pulmonary arterial hypertension (rare but serious with dasatinib) |
| Echocardiogram | Baseline and as indicated (ponatinib) | Vascular events screening with ponatinib |
Cardiovascular Risk Management
Second-generation TKIs (particularly nilotinib and ponatinib) are associated with increased cardiovascular risk. All patients should have:
- Baseline cardiovascular risk assessment (Australian absolute CVD risk calculator).
- Aggressive management of modifiable risk factors: smoking cessation, hypertension control, statin therapy for dyslipidaemia, diabetes management.
- Nilotinib is generally avoided in patients with significant pre-existing cardiovascular or peripheral vascular disease.
- Ponatinib requires careful cardiovascular risk–benefit assessment; dose reduction strategies (30 mg or 15 mg in responders) mitigate vascular risk.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
While CML incidence among Aboriginal and Torres Strait Islander Australians appears broadly comparable to the non-Indigenous population, significant disparities exist in presentation stage, access to haematology care, and long-term outcomes. The following considerations are essential for equitable CML management.
📚 References
- 1. Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34(4):966–984.
- 2. Baccarani M, Deininger MW, Rosti G, et al. European LeukemiaNet recommendations for the management of chronic myeloid leukemia: 2013. Blood. 2013;122(6):872–884.
- 3. National Comprehensive Cancer Network (NCCN). Clinical Practice Guidelines in Oncology: Chronic Myeloid Leukemia. Version 3.2024. Fort Washington, PA: NCCN; 2024.
- 4. Cortes JE, Saglio G, Kantarjian HM, et al. Final 5-year study results of DASISION: the dasatinib versus imatinib study in treatment-naïve chronic myeloid leukemia patients trial. J Clin Oncol. 2016;34(20):2333–2340.
- 5. Hughes TP, Saglio G, Quintás-Cardama A, et al. BCR-ABL1 mutation development during first-line treatment with dasatinib or imatinib for chronic myeloid leukemia in chronic phase. Leukemia. 2015;29(9):1832–1838.
- 6. Lipton JH, Chuah C, Guerci-Bresler A, et al. Ponatinib versus imatinib for newly diagnosed chronic myeloid leukaemia: an international, randomised, open-label, phase 3 trial. Lancet Oncol. 2016;17(5):612–621.
- 7. Mahon FX, Réa D, Guilhot J, et al. Discontinuation of imatinib in patients with chronic myeloid leukaemia who have maintained complete molecular remission for at least 2 years: the prospective, multicentre Stop Imatinib (STIM) trial. Lancet Oncol. 2010;11(11):1029–1035.
- 8. Ross DM, Branford S, Seymour JF, et al. Safety and efficacy of imatinib cessation for CML patients with stable undetectable minimal residual disease: results from the TWISTER study. Blood. 2013;122(4):515–522.
- 9. Australian Institute of Health and Welfare (AIHW). Cancer in Australia 2021. Cancer Series No. 133. Cat. no. CAN 144. Canberra: AIHW; 2021.
- 10. Cancer Australia. Optimal care pathway for Aboriginal and Torres Strait Islander people with cancer. Sydney: Cancer Australia; 2018.
- 11. Geissler J, Gil-Fernández JJ, Olavarria E, et al. Management of adverse events associated with bosutinib treatment of chronic-phase chronic myeloid leukemia: expert panel review. J Hematol Oncol. 2020;13(1):142.
- 12. Pfirrmann M, Baccarani M, Saussele S, et al. Prognosis of long-term survival considering disease-specific death in patients with chronic myeloid leukemia. Leukemia. 2016;30(1):48–56.
- 13. Branford S, Fletcher L, Cross NC, et al. Desirable performance characteristics for BCR-ABL measurement on an international reporting scale to allow consistent assessment of molecular response. Leukemia. 2008;22(4):732–738.
- 14. Nicolini FE, Basak GW, Soverini S, et al. Allogeneic stem cell transplantation for patients harboring T315I BCR-ABL. Leukemia. 2021;35(7):1997–2005.
- 15. Pharmaceutical Benefits Scheme (PBS). Schedule of Pharmaceutical Benefits. Australian Government Department of Health. Available at: https://www.pbs.gov.au. Accessed 2024.