📋 Key Information Summary
- Allogeneic haematopoietic stem cell transplantation (allo-HSCT) is a potentially curative procedure for high-risk haematological malignancies, bone marrow failure syndromes, and certain immunodeficiencies.
- Donor selection prioritises HLA-matched related donors (MRD), followed by matched unrelated donors (MUD) via national/international registries, with haploidentical and cord blood as alternatives.
- Conditioning regimens (myeloablative, reduced-intensity, non-myeloablative) are tailored to disease risk and patient fitness, aiming for engraftment within 14–21 days.
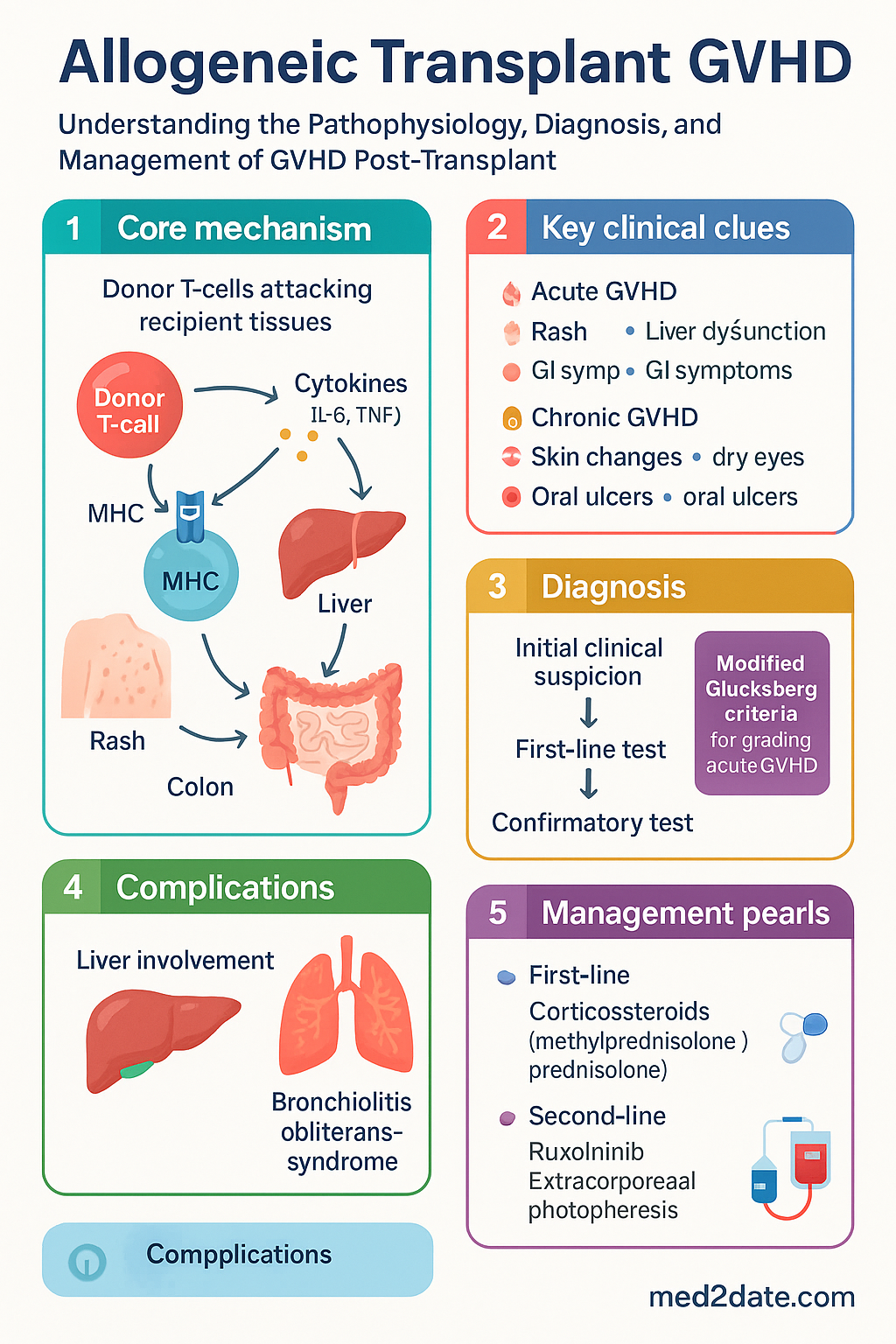
- Graft-versus-host disease (GVHD) is the major cause of non-relapse morbidity and mortality, mediated by donor T-cells attacking recipient tissues.
- Acute GVHD typically occurs within 100 days post-transplant, targeting skin, liver, and gastrointestinal tract; graded I–IV by modified Glucksberg criteria.
- Chronic GVHD resembles autoimmune disorders, can be limited or extensive, and is a leading cause of late transplant-related death.
- First-line systemic therapy for both acute and chronic GVHD is corticosteroids (methylprednisolone 2 mg/kg/day IV or prednisolone 1 mg/kg/day PO).
- Second-line options for steroid-refractory GVHD include ruxolitinib (PBS Authority Required for acute), extracorporeal photopheresis, mycophenolate, and calcineurin inhibitors.
- Supportive care is critical: infection prophylaxis (antiviral, antifungal, PJP), organ protection, nutritional support, and management of late effects (endocrine, musculoskeletal, secondary malignancies).
- Australian practice adheres to international guidelines (ASBMT/CIBMTR, EBMT) with local adaptations for antimicrobial prophylaxis (ASID/TSANZ) and PBS access.
- Aboriginal and Torres Strait Islander patients face barriers to transplant referral and access; culturally safe care and remote monitoring are essential.
- Long-term follow-up in a multidisciplinary transplant clinic is mandatory for surveillance of relapse, GVHD, infections, and late effects.
Introduction & Australian Epidemiology
Allogeneic haematopoietic stem cell transplantation (allo-HSCT) involves the infusion of haematopoietic progenitor cells from a related or unrelated donor to reconstitute the recipient's marrow and immune system. It provides a potent graft-versus-leukaemia (GvL) effect, reducing relapse risk in high-risk haematological malignancies, but carries the inherent risk of graft-versus-host disease (GVHD), a significant cause of transplant-related morbidity and mortality.
In Australia, approximately 500–600 allogeneic transplants are performed annually across 18 specialised centres. The Australian Bone Marrow Transplant Recipient (ABMTRR) registry data indicate that the most common indications are acute leukaemias (AML, ALL), myelodysplastic syndromes (MDS), lymphomas, and myeloproliferative neoplasms. The use of alternative donors (haploidentical, cord blood) has increased, now accounting for over 30% of procedures, expanding access but altering GVHD and infection profiles.
Transplant-related mortality has declined due to improved conditioning, supportive care, and GVHD prophylaxis, yet GVHD remains the leading cause of non-relapse death, affecting 30–50% of recipients. Chronic GVHD is a particular burden, impacting long-term quality of life and requiring prolonged immunosuppression.
Indications & Donor Matching (HLA)
Indications for Allogeneic Transplant
Allo-HSCT is indicated for diseases where the GvL effect is critical for cure or where non-malignant disorders require immune or marrow reconstitution. Key indications include:
- Acute myeloid leukaemia (AML): Intermediate or adverse risk in first complete remission (CR1), or any risk in second or subsequent remission.
- Acute lymphoblastic leukaemia (ALL): High-risk features (e.g., Philadelphia chromosome-positive, MLL rearrangement, poor early response) in CR1, or any ALL in CR2+.
- Myelodysplastic syndromes (MDS): Higher-risk MDS (IPSS-R Int-2 or High) or lower-risk MDS with severe cytopenias or transfusion dependence.
- Myeloproliferative neoplasms: Primary myelofibrosis (intermediate-2 or high risk), blast-phase CML.
- Lymphomas: Relapsed/refractory aggressive lymphomas (e.g., DLBCL) chemosensitive to salvage, or mantle cell lymphoma in CR1.
- Bone marrow failure syndromes: Severe aplastic anemia (especially young patients, or after immunosuppressive failure), Fanconi anaemia, paroxysmal nocturnal haemoglobinuria.
- Severe immunodeficiencies: Severe combined immunodeficiency (SCID), Wiskott-Aldrich syndrome.
- Haemoglobinopathies: Transfusion-dependent thalassaemia major, severe sickle cell disease with complications.
Donor Selection & HLA Matching
Donor selection is a critical determinant of transplant outcomes. The hierarchy of preferred donors is:
Umbilical Cord Blood (UCB): One or two units. Lower GVHD risk despite HLA mismatch, but slower engraftment and higher graft failure.
Conditioning & Engraftment
Conditioning Regimens
Conditioning therapy aims to eradicate the underlying disease and suppress the recipient's immune system to prevent graft rejection. Regimen intensity is classified as:
Engraftment
Engraftment is defined as the first of three consecutive days with an absolute neutrophil count (ANC) >0.5 x 109/L. Platelet engraftment is >20 x 109/L without transfusion for 7 days.
- Expected timeline: Neutrophil engraftment typically occurs by day +14 to +21 (earlier with peripheral blood grafts). Platelet recovery may take 4–6 weeks.
- Graft failure: Primary (no engraftment by day +28) or secondary (loss after initial engraftment). Causes include HLA mismatch, infection, drugs, and GVHD.
- Graft source: Peripheral blood stem cells (PBSC) lead to faster engraftment but higher chronic GVHD risk; bone marrow grafts have slower engraftment but lower chronic GVHD risk.
Acute vs Chronic GVHD
GVHD is classified by time of onset, clinical features, and pathology, though overlap syndromes exist. The 2014 NIH Consensus Criteria are the current standard.
Acute GVHD
Typically occurs within 100 days post-transplant, but can occur later (especially with RIC or DLI). Driven by donor T-cell response to host alloantigens.
| Organ | Clinical Stage | Modified Glucksberg Grade |
|---|---|---|
| Skin | Stage 1: Rash <25% BSA Stage 2: Rash 25-50% BSA Stage 3: Rash >50% BSA Stage 4: Bullae/desquamation | Grade I: Stage 1-2 skin only Grade II: Stage 3 skin or Stage 1 GI/liver Grade III: Stage 2-3 GI/liver Grade IV: Stage 4 any organ |
| Liver (bilirubin) | Stage 1: 34-51 µmol/L Stage 2: 51-102 µmol/L Stage 3: 102-255 µmol/L Stage 4: >255 µmol/L | |
| GI (volume/day) | Stage 1: 500-1000 mL Stage 2: 1000-1500 mL Stage 3: >1500 mL Stage 4: Severe pain ± ileus |
Chronic GVHD
Can occur at any time after transplant, often following acute GVHD. Presents with features resembling autoimmune/connective tissue disorders. Classified as:
- Classic chronic GVHD: No features of acute GVHD.
- Overlap syndrome: Features of both acute and chronic GVHD present simultaneously.
Severity (mild, moderate, severe) is scored based on the number of organs involved and the degree of functional impairment. Common manifestations include:
- Skin: Lichen planus-like, sclerodermatous, poikiloderma.
- Mouth: Lichenoid changes, xerostomia, oral ulcers.
- Eyes: Dry eyes (keratoconjunctivitis sicca).
- Liver: Cholestatic hepatitis.
- Lungs: Bronchiolitis obliterans syndrome (BOS) – poor prognosis.
- Joints/Fascia: Fasciitis, contractures.
Management of GVHD & Late Effects
GVHD Prophylaxis
Standard prophylaxis is a calcineurin inhibitor (CNI: cyclosporine or tacrolimus) combined with a short course of methotrexate (MTX) or mycophenolate mofetil (MMF). Haploidentical transplants typically use post-transplant cyclophosphamide (PTCy) plus a CNI/MMF.
First-Line Therapy for GVHD
Second-Line & Salvage Therapies for Steroid-Refractory GVHD
Other options include: MMF (PBS General Benefit), Sirolimus (PBS Authority Required for chronic GVHD), Infliximab (PBS Authority Required), Etanercept, and low-dose Alemtuzumab.
Supportive Care & Infection Prophylaxis
| Phase | Key Prophylaxis | Australian Recommendation |
|---|---|---|
| Pre-engraftment (Day 0 to +30) | Antibacterial, Antifungal, Antiviral (HSV/VZV) | Ciprofloxacin or Penicillin. Fluconazole or an echinocandin. Aciclovir 200-400 mg PO BD (or IV if intolerant). |
| Post-engraftment (Day +30 to +100) | Antifungal, Antiviral (CMV, VZV), PJP | Posaconazole or itraconazole. Valganciclovir for high-risk CMV. Continue aciclovir. Trimethoprim/sulfamethoxazole (TMP/SMX) 3 times weekly. |
| Late (>Day +100) | Antiviral, PJP, Encapsulated organisms | Continue aciclovir/valaciclovir for 12 months. Continue TMP/SMX for 6-12 months. Penicillin V if chronic GVHD or asplenia. |
Late Effects of Transplant
Survivors require lifelong monitoring. Key late effects include:
- Endocrine: Hypothyroidism, gonadal failure (require hormone replacement), metabolic syndrome.
- Musculoskeletal: Osteoporosis (steroid use), avascular necrosis.
- Pulmonary: Restrictive or obstructive lung disease (often due to chronic GVHD).
- Cardiovascular: Premature atherosclerosis, cardiomyopathy (from prior anthracyclines/chest radiation).
- Secondary malignancies: Increased risk of solid tumours (skin, head/neck), post-transplant lymphoproliferative disorder (PTLD).
- Psychosocial: Fatigue, depression, anxiety, cognitive impairment ("chemo brain").
Special Populations
📚 References
-
1.
D'Souza A, Fretham C. Current Uses and Outcomes of Hematopoietic Cell Transplantation (HCT): CIBMTR Summary Slides, 2023. Available at:
- 2. Penack O, Peczynski C, Mohty M, et al. How much has allogeneic stem cell transplant-related mortality improved since the 1990s? A retrospective analysis from the EBMT. Blood Adv. 2020;4(24):6283-6290.
- 3. Jagasia MH, Greinix HT, Arora M, et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group report. Biol Blood Marrow Transplant. 2015;21(3):389-401.e1.
- 4. Australasian Society of Blood and Marrow Transplantation (ASBMT). Guidelines for Referral for Allogeneic Stem Cell Transplant. 2022.
- 5. Australian Bone Marrow Donor Recipient Registry (ABMTRR). Annual Report 2022. National Blood Authority, Australia.
- 6. Curtin P, et al. Post-transplant cyclophosphamide for graft-versus-host disease prophylaxis in haploidentical transplantation: a systematic review and meta-analysis. Transplant Cell Ther. 2023.
- 7. Australasian Society for Infectious Diseases (ASID) & Transplantation Society of Australia and New Zealand (TSANZ). Guidelines for the Prevention of Infection in Hematopoietic Stem Cell Transplant Recipients. 2023.
- 8. The Royal Australian College of General Practitioners (RACGP). Post-transplant care in general practice. Red Book, 2023.
- 9. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework 2023 summary report.
- 10. Martin PJ, et al. First- and second-line systemic treatment of acute graft-versus-host disease: recommendations of the American Society of Blood and Marrow Transplantation. Biol Blood Marrow Transplant. 2012;18(8):1150-1163.
- 11. Carpenter PA, et al. Post-transplant cyclophosphamide for prevention of graft-versus-host disease. N Engl J Med. 2023;389:1075-1087.