📋 Key Information Summary
- Blood transfusion reactions are classified by timing (acute ≤24 h vs delayed >24 h) and mechanism (immune vs non-immune); systematic classification guides investigation and management.
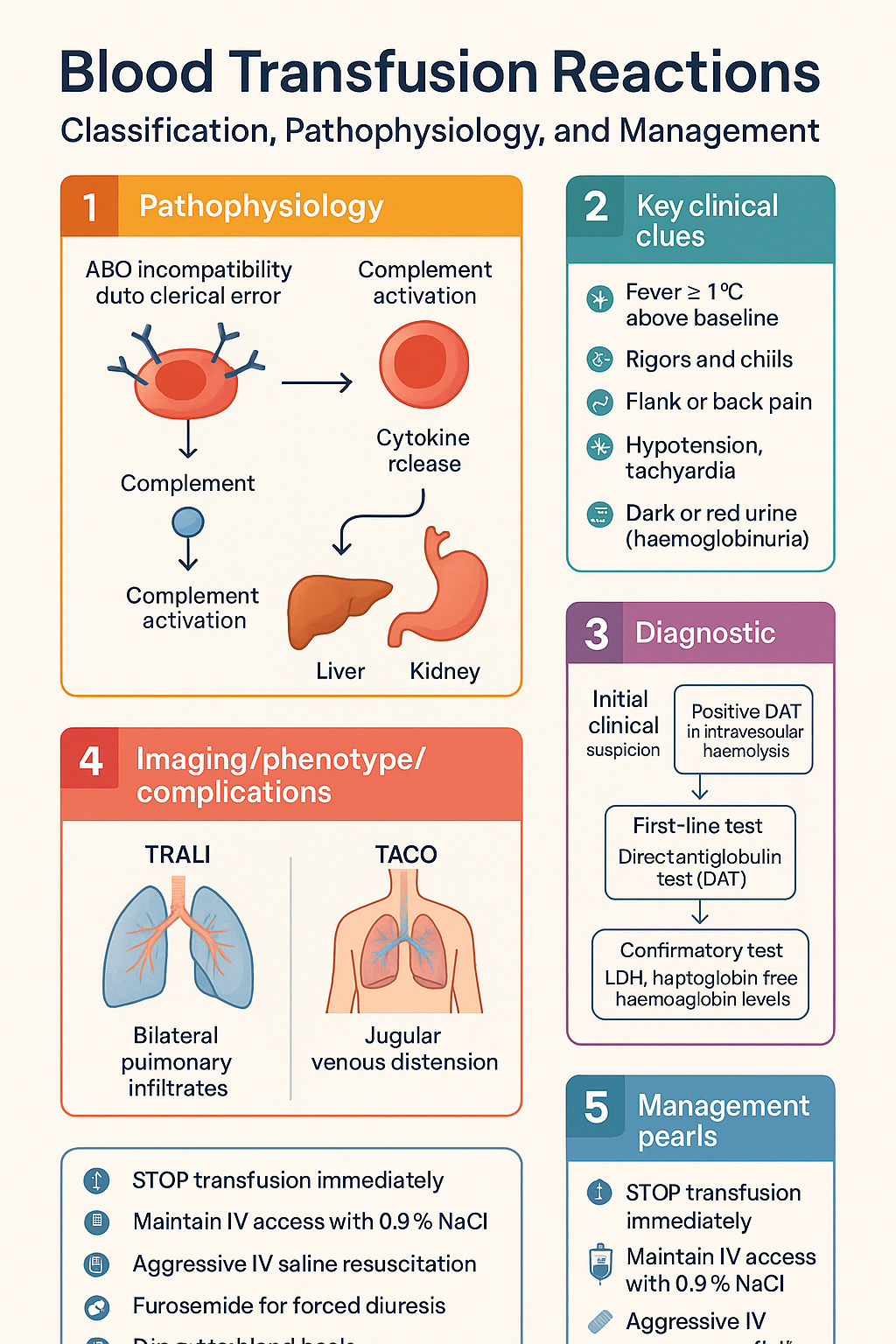
- Acute haemolytic transfusion reaction (AHTR) is most commonly caused by ABO incompatibility due to clerical error and remains the leading cause of transfusion-related death in Australia.
- STOP the transfusion immediately for any suspected reaction — maintain IV access with 0.9% NaCl, do NOT use dextrose-containing solutions.
- Febrile non-haemolytic transfusion reaction (FNHTR) is the most common immunological reaction, occurring in 0.5–3% of transfusions; fever ≥1°C above baseline with rigors is typical.
- Differentiate TRALI (onset ≤6 h, bilateral pulmonary infiltrates, no volume overload) from TACO (jugular venous distension, raised BNP, pulmonary oedema with fluid overload).
- AHTR management centres on aggressive IV 0.9% saline resuscitation, forced diuresis (furosemide 40–80 mg IV), and renal protection; consider sodium bicarbonate if haemoglobinuria causes tubular obstruction.
- FNHTR is managed with paracetamol 1 g PO (500 mg if <50 kg) ± meperidine 25–50 mg IV for rigors; antipyretic premedication is controversial and not universally recommended.
- All suspected reactions must be reported to the blood bank and hospital transfusion committee; nationally, reports feed into the National Blood Authority Haemovigilance Programme.
- Leucoreduction and pre-storage filtration significantly reduce FNHTR risk; leucoreduced components are standard practice across Australian blood services.
- Transfusion-associated bacterial contamination (especially platelets) presents with fever, rigors, hypotension, and requires broad-spectrum antibiotics and blood culture before antibiotics.
- Aboriginal and Torres Strait Islander patients may face delayed diagnosis of transfusion complications due to geographic remoteness from major blood services and limited access to specialist haematology input.
- Always perform a bedside identity check (two patient identifiers), check the compatibility label, and observe the patient during the first 15 minutes of each unit.
Introduction & Australian Epidemiology
Blood transfusion is a common and life-saving intervention, with approximately 1.4 million blood components issued annually in Australia by the Australian Red Cross Lifeblood. Transfusion reactions range from mild febrile or urticarial events to life-threatening haemolytic, anaphylactic, and pulmonary syndromes. Prompt recognition, systematic classification, and evidence-based management are essential to minimise morbidity and mortality.
Haemovigilance data from the National Blood Authority (NBA) Haemovigilance Programme indicate that adverse transfusion reactions are reported in approximately 0.5–1.0% of all transfusion episodes. Serious adverse events, including AHTR, TRALI, and deaths, remain rare but carry significant consequences. The majority of AHTRs in Australia result from clerical or identification errors at the bedside, underscoring the critical importance of the National Safety and Quality Health Service (NSQHS) Standards — Standard 7: Blood and Blood Products.
This guideline covers the classification, pathophysiology, diagnosis, and evidence-based management of acute blood transfusion reactions encountered in Australian clinical practice, with attention to acute haemolytic reactions and febrile non-haemolytic transfusion reactions.
Classification of Reactions
Transfusion reactions are classified by timing (acute ≤24 hours vs delayed >24 hours) and mechanism (immune-mediated vs non-immune). Understanding the classification framework enables systematic evaluation and appropriate management.
| Category | Acute (≤24 h) | Delayed (>24 h) |
|---|---|---|
| Immune-mediated | Acute haemolytic (AHTR), febrile non-haemolytic (FNHTR), allergic/anaphylactic, TRALI, TACO | Delayed haemolytic (DHTR), transfusion-associated GVHD, post-transfusion purpura, transfusion-related alloimmunisation |
| Non-immune | Bacterial contamination, hypothermia (massive transfusion), citrate toxicity, metabolic (hyperkalaemia, hypocalcaemia) | Transfusion-transmitted infection (viral, parasitic, prion), iron overload (chronic transfusion) |
Key clinical features for differentiation at the bedside include timing of onset, presence of fever, rigors, hypotension, respiratory distress, flank or back pain, and urine discolouration. A systematic approach — beginning with stopping the transfusion and notifying the blood bank — is essential for all suspected reactions.
Acute Haemolytic Transfusion Reaction (AHTR)
AHTR is the most dangerous acute transfusion reaction, most commonly caused by ABO-incompatible red cell transfusion resulting from identification or clerical errors. Intravascular haemolysis is mediated by complement activation (IgM antibodies), leading to disseminated intravascular coagulation (DIC), acute kidney injury, and potentially death.
Pathophysiology
Recipient antibodies (typically anti-A or anti-B IgM) bind donor red cell surface antigens, activating the classical complement pathway. C3a and C5a anaphylatoxins trigger cytokine release (TNF-α, IL-1, IL-6, IL-8), causing systemic inflammatory response. Free haemoglobin binds nitric oxide causing vasoconstriction, and Hb/haem released into plasma is nephrotoxic, precipitating in the renal tubules. Activation of the coagulation cascade leads to DIC with consumption of clotting factors and fibrinogen.
Clinical Presentation
Symptoms typically appear within minutes to hours of starting the transfusion:
- Fever ≥1°C above baseline, rigors, chills
- Flank or back pain (classic presentation)
- Hypotension, tachycardia, anxiety, feeling of "impending doom"
- Dark or red urine (haemoglobinuria) — may not be present early
- Oozing from IV sites or surgical wounds (DIC)
- Chest pain, dyspnoea, pulmonary oedema (severe cases)
- Oliguria progressing to anuric renal failure
Investigations
Differential Diagnosis
- Bacterial contamination of blood product (sepsis)
- TRALI (respiratory distress without haemolysis)
- Anaphylaxis (without haemolysis markers)
- Massive transfusion — hypothermia, citrate toxicity, hyperkalaemia
Febrile Non-Haemolytic Transfusion Reaction (FNHTR)
FNHTR is the most common immunological transfusion reaction, occurring in approximately 0.5–3% of transfusions. It is characterised by fever without evidence of haemolysis or infection. FNHTR is more common with platelet transfusions than red cell transfusions.
Pathophysiology
FNHTR is mediated by recipient antibodies reacting to donor leucocyte antigens or by cytokines accumulated in stored blood components. Pre-storage leucoreduction (filtering white blood cells before storage) reduces cytokine accumulation and has significantly decreased FNHTR rates in Australia, where leucoreduced components are standard. The inflammatory mediators involved include IL-1, IL-6, IL-8, and TNF-α released from residual leucocytes.
Clinical Presentation
Onset is typically during or within 4 hours of transfusion completion:
- Fever ≥1°C (or ≥2°F) rise above pre-transfusion temperature
- Rigors and chills (may be severe)
- Headache, myalgia, malaise
- Nausea may be present
- Tachycardia, but typically no hypotension (unless severe)
- Absence of: haemoglobinuria, flank pain, urticaria, angioedema, bronchospasm (helps distinguish from AHTR and anaphylaxis)
Diagnostic Criteria
- Temperature rise ≥1°C during or within 4 hours of transfusion
- No other explanation for fever (e.g., sepsis, medication)
- Negative DAT and no evidence of haemolysis (normal LDH, haptoglobin)
- Negative blood cultures (at 48 hours)
- Normal blood bank compatibility testing (re-crossmatch of post-reaction sample)
Risk Factors
| Risk Factor | Mechanism |
|---|---|
| Repeated transfusions | Alloimmunisation to leucocyte antigens |
| Female sex / multiparity | HLA sensitisation from pregnancy |
| Non-leucoreduced components | Higher leucocyte load and cytokine accumulation |
| Platelet transfusions | Stored at 22°C — more cytokine accumulation than RBCs stored at 4°C |
| Prolonged storage duration | Increased cytokine levels in stored components |
Management & Prevention
Immediate Management — All Suspected Reactions
Management of Acute Haemolytic Transfusion Reaction
Resuscitation and Supportive Care
- IV 0.9% NaCl: Rapid infusion to maintain renal perfusion and blood pressure; target urine output >100 mL/h in adults to flush free haemoglobin through renal tubules
- Furosemide: 40–80 mg IV bolus to promote forced diuresis and protect renal function
- Sodium bicarbonate: 50–100 mmol IV if urine is dark/acidic — alkalinises urine to reduce haemoglobin/tamm-Horsfall protein precipitation (evidence limited; use based on clinical judgement)
- Vasopressors: Noradrenaline infusion if refractory hypotension despite volume resuscitation
- Monitor: Continuous cardiac monitoring, hourly urine output, serial FBC/coagulation/creatinine
- DIC management: Cryoprecipitate if fibrinogen <1.0 g/L; platelets if <50 × 10⁹/L with active bleeding; FFP for active coagulopathy
- Renal replacement therapy: Initiate haemodialysis or CRRT if anuric renal failure develops
Management of FNHTR
- Stop the transfusion and investigate to exclude AHTR and sepsis as per protocol
- Paracetamol: 1 g PO (or 500 mg if <50 kg) — avoid aspirin/NSAIDs (may worsen bleeding if occult DIC)
- Meperidine (pethidine): 25–50 mg IV slow push for severe rigors — use with caution in renal impairment and elderly
- Physical cooling measures for high fever
- The transfusion may be restarted cautiously if AHTR and sepsis are excluded and symptoms resolve with treatment — administer at a slower rate with close observation
Management of Other Acute Reactions
| Reaction | Key Management |
|---|---|
| Allergic / Urticarial | Stop transfusion. Antihistamine — cetirizine 10 mg PO or chlorphenamine 10 mg IV. Restart cautiously if isolated urticaria resolves; premedicate subsequent transfusions with antihistamine. |
| Anaphylaxis | IM adrenaline 500 µg (0.5 mL of 1:1000) anterolateral thigh. Repeat q5min. IV adrenaline infusion if refractory. IV fluids. Chlorphenamine 10 mg IV. Hydrocortisone 200 mg IV. IgA-deficient patients: use washed RBCs and IgA-depleted plasma. |
| TRALI | Supportive — oxygen, NIV or mechanical ventilation. NO diuretics (unlike TACO). Most resolve within 72–96 h. Corticosteroids not proven. Report to haemovigilance (serious adverse event). |
| TACO | Sit upright. Oxygen. Furosemide 40–80 mg IV. Slow transfusion rate or stop. Consider NIV (CPAP/BiPAP). BNP to differentiate from TRALI. |
| Bacterial contamination | Broad-spectrum IV antibiotics (e.g., piperacillin-tazobactam 4.5 g IV + vancomycin 25–30 mg/kg IV). Blood cultures × 2 (patient + unit). Aggressive resuscitation. ICU admission if septic shock. |
| Transfusion-related hypothermia | Use blood warmer for rapid/massive transfusion. Warm blankets. Monitor core temperature. Avoid warming blood above 42°C. |
Prevention Strategies
| Strategy | Target Reaction | Evidence |
|---|---|---|
| Strict bedside identity check (two patient identifiers) | AHTR (clerical error prevention) | NSQHS Standard 7; mandatory in all Australian facilities |
| Leucoreduction (pre-storage filtration) | FNHTR, CMV transmission | Standard practice — Lifeblood provides universal leucoreduced components in Australia |
| Paracetamol premedication | FNHTR (secondary prevention) | Reasonable for patients with prior FNHTR; not recommended as routine primary prevention |
| Antihistamine premedication | Allergic / urticarial | Effective for secondary prevention of recurrent allergic reactions |
| Washed RBC components | FNHTR (recurrent), anaphylaxis (IgA-deficient) | Removes plasma proteins and residual antibodies |
| Irradiated components | Transfusion-associated GVHD | Indicated for immunocompromised recipients, directed donations, HLA-matched components |
| Blood warmers (≤42°C) | Hypothermia (massive transfusion) | Standard in massive transfusion protocols |
| Bacterial screening of platelets | Bacterial contamination | Routine in Australia; Lifeblood screens all platelet components |
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. National Blood Authority Australia. National Safety and Quality Health Service Standards — Standard 7: Blood and Blood Products. Australian Commission on Safety and Quality in Health Care; 2021.
- 2. Australian Red Cross Lifeblood. Blood Component Information. Melbourne: Lifeblood; 2024. Available from: www.lifeblood.com.au
- 3. Delaney M, Wendel S, Bercovitz RS, et al. Transfusion reactions: prevention, diagnosis, and treatment. Lancet. 2016;388(10061):2825–2836.
- 4. National Blood Authority. Australia's Haemovigilance Framework. Canberra: NBA; 2019.
- 5. Callum JL, Pinkerton PH, Lima A, et al. Bloody Easy 4: Blood Transfusions, Blood Alternatives and Transfusion Reactions — A Guide to Transfusion Medicine. 4th ed. Toronto: Ontario Regional Blood Coordinating Network; 2016.
- 6. Bassett HF, Bhatt N, Stanworth SJ. Transfusion-related adverse events: recognition and management. Br J Hosp Med. 2022;83(6):1–10.
- 7. Australian Institute of Health and Welfare. Blood and blood products — Australian hospital statistics. Canberra: AIHW; 2023.
- 8. AABB (Association for the Advancement of Blood & Biotherapies). AABB Technical Manual. 20th ed. Bethesda: AABB; 2020.
- 9. National Health and Medical Research Council. Clinical Practice Guidelines: Perinatal Care. Canberra: NHMRC; 2022.
- 10. RHDAustralia (RHD Australia — Menzies School of Health Research). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Darwin; 2020.
- 11. Tobian AAR, Heddle NM, Wiegmann TLJ, Carson JL. Red blood cell transfusion: 2016 clinical practice guidelines from the AABB. Transfusion. 2016;56(10):2627–2630.
- 12. Stainsby D, Jones H, Asher D, et al. Serious hazards of transfusion: a decade of haemovigilance in the UK. Transfus Med Rev. 2006;20(4):273–282.