📋 Key Information Summary
- Iron deficiency is the most common nutritional deficiency worldwide and the leading cause of anaemia in Australia, particularly affecting premenopausal women, Aboriginal and Torres Strait Islander peoples, the elderly, and those with chronic disease.
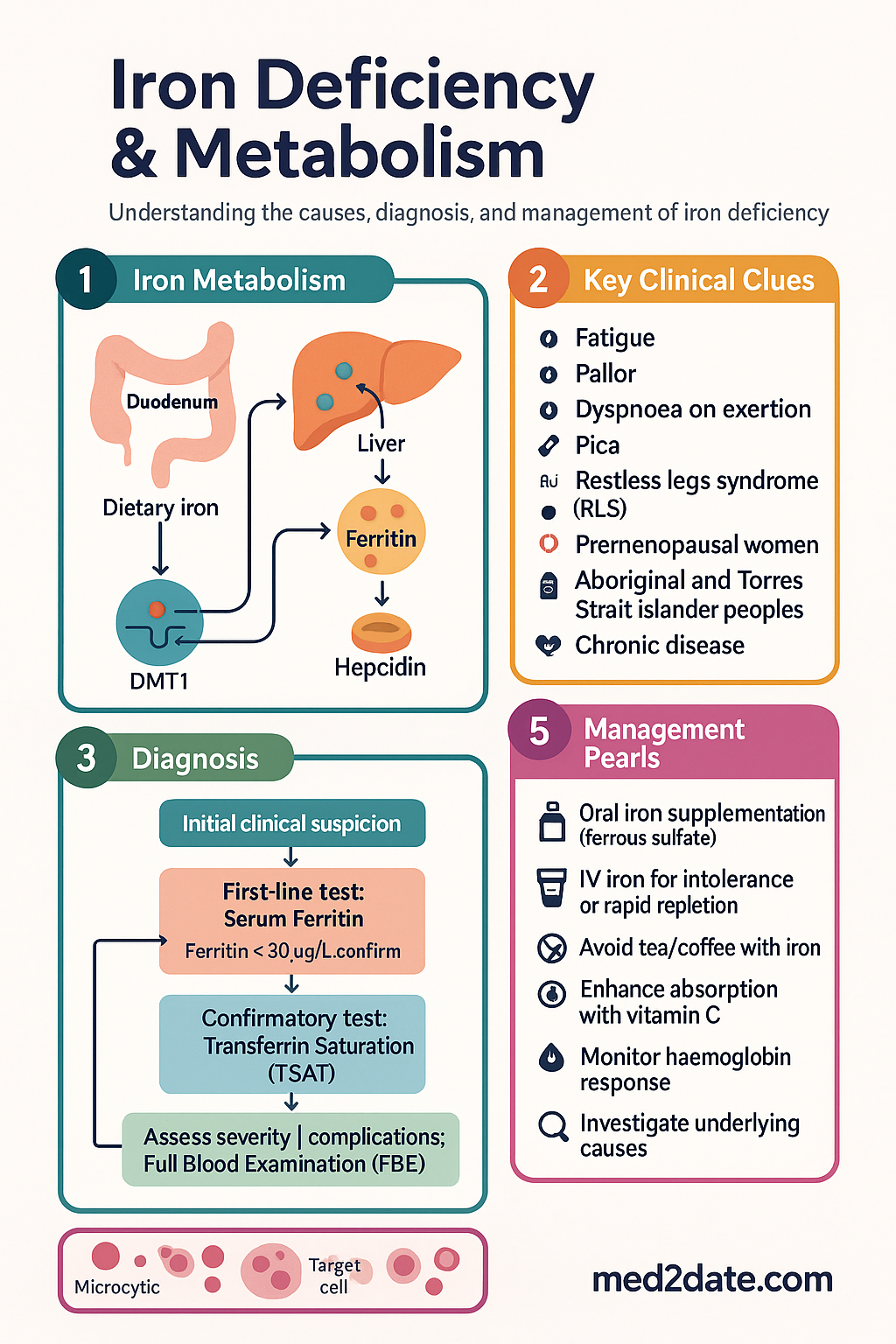
- Diagnosis requires a combination of tests: serum ferritin (most sensitive single test), serum iron, transferrin saturation (TSAT), and total iron-binding capacity (TIBC). Ferritin <30 µg/L confirms iron deficiency; ferritin 30–100 µg/L with TSAT <20% is suggestive.
- Ferritin is an acute-phase reactant — in the setting of inflammation, infection, or liver disease, a ferritin level <100 µg/L may still indicate true iron deficiency.
- Investigation of the underlying cause is mandatory, not optional. In men and postmenopausal women, gastrointestinal blood loss must be excluded with bidirectional endoscopy.
- Oral iron (ferrous sulfate 325 mg [~65 mg elemental iron] PO daily to TDS) is first-line for non-severe deficiency without malabsorption or intolerance. Alternate-day dosing may improve absorption and reduce side effects.
- IV iron is indicated when oral iron is ineffective, poorly tolerated, contraindicated (e.g., IBD flare, CKD on ESA), or when rapid repletion is needed (e.g., perioperative, pregnancy in third trimester).
- Ferric carboxymaltose (Ferinject®) and iron polymaltose (Ferrosig®) are commonly used IV iron preparations in Australia. Ferric carboxymaltose allows up to 1000 mg in a single infusion.
- Expected haemoglobin rise: 10–20 g/L over 2–4 weeks with adequate treatment. Reticulocyte response peaks at days 5–10. Aim to replenish iron stores (target ferritin >100 µg/L) even after haemoglobin normalises.
- Iron requirements increase substantially in pregnancy (additional ~1000 mg total), rapid growth periods (infancy, adolescence), and chronic blood loss (menorrhagia, GI bleeding).
- Oral iron should not be taken with tea, coffee, calcium supplements, proton pump inhibitors, or antacids — all reduce absorption. Vitamin C (ascorbic acid) enhances non-haem iron absorption.
- IV iron carries a small risk of anaphylaxis (estimated <1:200,000 for ferric carboxymaltose), hypophosphataemia (particularly ferric carboxymaltose), and infusion reactions. Monitoring during and after infusion is essential.
- Aboriginal and Torres Strait Islander peoples have disproportionately higher rates of iron deficiency driven by nutritional inadequacy, chronic infection, hookworm infestation in remote communities, and barriers to healthcare access.
Introduction & Australian Epidemiology
Iron deficiency is the most common cause of anaemia worldwide and a leading contributor to the global burden of disease. It presents classically with microcytic hypochromic anaemia and manifests clinically with fatigue, pallor, dyspnoea on exertion, pica, restless legs syndrome, koilonychia, and angular cheilitis. In Australia, iron deficiency affects approximately 12% of premenopausal women, 5–8% of men, and up to 20% of Aboriginal and Torres Strait Islander women of reproductive age.
The Australian Institute of Health and Welfare (AIHW) estimates that iron deficiency anaemia contributes to significant healthcare utilisation, particularly in primary care and emergency departments. Populations at greatest risk include premenopausal women (due to menstrual losses), pregnant women (increased fetal and placental demands), infants and adolescents (rapid growth), the elderly (chronic disease, nutritional inadequacy, occult GI blood loss), blood donors, vegetarians and vegans, and individuals with chronic gastrointestinal conditions such as coeliac disease or inflammatory bowel disease.
Iron deficiency exists on a spectrum: depleted iron stores precede iron-deficient erythropoiesis, which in turn precedes frank iron deficiency anaemia (IDA). Early identification and treatment of iron deficiency — before anaemia develops — is important to prevent symptomatic morbidity, impaired cognitive function in children, adverse pregnancy outcomes, and reduced quality of life. This guideline provides a comprehensive overview of iron metabolism, causes, investigation, and management aligned with Australian practice.
Iron Metabolism & Stores
Iron is an essential element required for oxygen transport (haemoglobin and myoglobin), electron transfer in the mitochondrial respiratory chain (cytochromes), DNA synthesis, and numerous enzymatic reactions. Total body iron in a healthy adult is approximately 3–4 g, distributed as follows:
| Compartment | Amount (approx.) | % of Total | Function |
|---|---|---|---|
| Haemoglobin iron | 2.0–2.5 g | ~65% | Oxygen transport |
| Storage iron (ferritin, haemosiderin) | 0.5–1.0 g | ~20–25% | Reserve pool (liver, spleen, bone marrow macrophages) |
| Myoglobin iron | ~200 mg | ~5% | Muscle oxygen storage |
| Tissue iron (cytochromes, enzymes) | ~150 mg | ~4% | Cellular respiration, enzymatic function |
| Transport iron (transferrin-bound) | ~3 mg | <1% | Iron delivery to erythroid precursors |
Key Regulatory Proteins
- Divalent metal transporter 1 (DMT1): Located on the apical membrane of duodenal enterocytes; mediates uptake of non-haem (ferrous) iron.
- Ferroportin: The sole known cellular iron exporter, located on the basolateral membrane of enterocytes and on macrophages. Regulated by hepcidin.
- Hepcidin: A 25-amino-acid peptide hormone synthesised by the liver. The master regulator of systemic iron homeostasis. Hepcidin binds to ferroportin, triggering its internalisation and degradation, thereby reducing iron absorption from the gut and iron release from macrophages.
- Transferrin: The plasma iron transport glycoprotein. Each molecule binds two ferric (Fe³⁺) ions. Transferrin saturation (TSAT) reflects the proportion of transferrin binding sites occupied by iron.
- Ferritin: An intracellular iron storage protein; serum ferritin is proportional to total body iron stores (in the absence of inflammation).
- Hephaestin and caeruloplasmin: Ferroxidases that oxidise Fe²⁺ to Fe³⁺ for loading onto transferrin.
Iron Absorption
Dietary iron exists in two forms: haem iron (from animal sources: red meat, poultry, fish) and non-haem iron (from plant sources, fortified foods). Haem iron is absorbed intact via the haem carrier protein 1 (HCP1) at 15–35% efficiency. Non-haem iron must be reduced from Fe³⁺ to Fe²⁺ by duodenal cytochrome b (DcytB) and then absorbed via DMT1 at 2–20% efficiency. Non-haem iron absorption is enhanced by ascorbic acid, citric acid, and animal protein, and inhibited by phytates, polyphenols (tea, coffee), calcium, and certain medications (PPIs, antacids).
Daily iron losses are approximately 1–2 mg/day (desquamation of GI mucosal cells, skin, urinary losses). Menstruating women lose an additional 0.5–1 mg/day on average (higher with heavy menstrual bleeding). The recommended daily intake (NHMRC Nutrient Reference Values) is 8 mg/day for adult men, 18 mg/day for premenopausal women, 27 mg/day in pregnancy, and 9 mg/day for lactating women.
Causes of Iron Deficiency
Iron deficiency results from an imbalance between iron intake/absorption and iron losses/demand. The three principal aetiological categories are blood loss, malabsorption, and increased physiological demand. In clinical practice, multiple factors often coexist.
1. Blood Loss (Most Common Cause)
- Gastrointestinal blood loss: Colorectal cancer, gastric cancer, oesophagitis/gastritis, peptic ulcer disease, angiodysplasia, inflammatory bowel disease, NSAID gastropathy, hookworm infestation (particularly in ATSI remote communities), hereditary haemorrhagic telangiectasia, Meckel's diverticulum.
- Gynaecological: Heavy menstrual bleeding (HMB) — the most common cause in premenopausal women. Defined as >80 mL blood loss per cycle or symptoms of excessive menstrual flow. Causes include fibroids, adenomyosis, endometrial polyps, coagulopathy (e.g., von Willebrand disease), and anovulatory cycles.
- Other: Frequent blood donation, chronic haematuria (e.g., IgA nephropathy), intravascular haemolysis (e.g., mechanical heart valves, paroxysmal nocturnal haemoglobinuria), post-surgical blood loss.
2. Malabsorption
- Coeliac disease: Affects ~1% of the Australian population; frequently presents with iron deficiency as the sole manifestation. All patients with unexplained iron deficiency should be screened with tissue transglutaminase (tTG) IgA and total IgA.
- Helicobacter pylori infection: Causes iron deficiency through altered gastric acid secretion (impairing non-haem iron absorption), increased iron utilisation by the bacterium, and chronic blood loss from gastritis.
- Atrophic gastritis / auto-immune gastritis: Reduced gastric acid impairs Fe³⁺ → Fe²⁺ conversion. May coexist with pernicious anaemia (vitamin B12 deficiency).
- Inflammatory bowel disease: Active inflammation of the duodenum/proximal ileum, chronic blood loss, and hepcidin-mediated iron sequestration.
- Bariatric surgery: Roux-en-Y gastric bypass and sleeve gastrectomy reduce the absorptive surface and bypass the duodenum (primary site of iron absorption).
- Medications: Proton pump inhibitors (PPIs), H2-receptor antagonists, calcium supplements, and antacids reduce non-haem iron absorption by raising gastric pH.
- Other: Chronic diarrhoea, previous gastrectomy, small bowel resection.
3. Increased Demand
- Pregnancy: Total iron requirement ~1000 mg (expanded maternal red cell mass ~450 mg, fetal/placental iron ~300 mg, blood loss at delivery ~250 mg). Without supplementation, most women become iron deficient.
- Lactation: Additional 0.5–1 mg/day lost in breast milk.
- Rapid growth periods: Infancy (particularly premature neonates with low iron stores), adolescence (especially with HMB onset).
- Athletes: Endurance athletes with increased GI losses (runner's colitis), haemolysis (foot-strike), and sweat iron losses.
4. Reduced Dietary Intake
- Vegetarian and vegan diets (non-haem iron with lower bioavailability ~5–12%).
- Restricted diets — elderly living alone, food insecurity, eating disorders.
- Inadequate dietary diversity in remote ATSI communities.
5. Functional Iron Deficiency
In chronic inflammatory conditions (CKD, CHF, cancer, chronic infections), elevated hepcidin impairs iron absorption and macrophage iron release, leading to iron-restricted erythropoiesis despite adequate or even elevated iron stores. This is termed functional iron deficiency and is distinct from true (absolute) iron deficiency. TSAT <20% with ferritin >100 µg/L in the setting of inflammation suggests functional deficiency.
Investigations
Iron Studies — Core Tests
| Test | Normal Range | Iron Deficiency | Notes |
|---|---|---|---|
| Serum Ferritin | 20–300 µg/L (M) 20–200 µg/L (F) |
<30 µg/L (definite) 30–100 µg/L (probable, if TSAT <20%) |
Best single marker of iron stores. Acute-phase reactant — may be falsely normal/elevated with inflammation. |
| Serum Iron | 10–30 µmol/L | ↓ Low (often <10 µmol/L) | Diurnal variation (higher in AM). Non-specific — low in inflammation, infection. |
| TIBC | 45–80 µmol/L | ↑ High (>80 µmol/L) | Reflects transferrin concentration. Rises in iron deficiency as liver produces more transferrin. |
| Transferrin Saturation (TSAT) | 20–50% | <20% (often <15%) | Calculated: (serum iron ÷ TIBC) × 100. Key indicator of iron availability for erythropoiesis. |
| Soluble Transferrin Receptor (sTfR) | 0.8–1.8 mg/L | ↑ Elevated | Not affected by inflammation. Useful to distinguish true iron deficiency from anaemia of chronic disease. sTfR/log ferritin index >2 suggests true ID. |
Interpreting Iron Studies in the Setting of Inflammation
- Ferritin <30 µg/L: Confirms iron deficiency regardless of CRP.
- Ferritin 30–100 µg/L with TSAT <20% and elevated CRP: Probable iron deficiency in the setting of coexisting inflammation.
- Ferritin >100 µg/L with TSAT <20%: Functional iron deficiency (CKD, CHF, cancer) — iron stores present but inaccessible to erythroid precursors.
- When ferritin interpretation is uncertain, sTfR or the sTfR/ferritin index can help distinguish true deficiency from anaemia of chronic disease.
Full Blood Examination (FBE)
- Haemoglobin: Low (anaemia); normal in early iron depletion.
- MCV: Low (<80 fL) — microcytosis (late finding).
- MCH: Low (<27 pg) — hypochromia.
- RDW: Elevated — anisocytosis (helps distinguish from thalassaemia trait where RDW is typically normal).
- Blood film: Microcytic hypochromic red cells, pencil cells (elliptocytes), target cells.
- Reticulocyte count: Low or inappropriately normal relative to degree of anaemia.
MBS-Itemised Investigations for Underlying Cause
Pathophysiology
Iron deficiency develops through a predictable sequence of depletion:
- Stage 1 — Iron store depletion: Storage iron (ferritin) is consumed to meet ongoing erythropoietic demand. Ferritin falls below normal. No functional deficit yet — haemoglobin and TSAT remain normal.
- Stage 2 — Iron-deficient erythropoiesis: Iron supply to the erythroid marrow becomes insufficient. TSAT falls below 20%. RBC precursors show impaired haem synthesis. Haemoglobin may remain normal or begin to decline.
- Stage 3 — Iron deficiency anaemia: Haemoglobin falls below sex-specific reference ranges. Microcytic, hypochromic anaemia develops. Marrow erythroid hyperplasia with absent stainable iron. Clinical symptoms (fatigue, dyspnoea, pallor) become apparent.
At the cellular level, iron deficiency impairs:
- Haem synthesis: Reduced haem leads to decreased haemoglobin production, smaller RBCs, and impaired oxygen delivery.
- Myoglobin synthesis: Results in impaired muscle function and exercise intolerance.
- Mitochondrial function: Iron-containing cytochromes and iron-sulphur cluster proteins are essential for oxidative phosphorylation. Deficiency causes cellular energy deficit.
- Immune function: Impaired lymphocyte proliferation and neutrophil bactericidal activity.
- Neurological function: Iron is a cofactor for tyrosine hydroxylase and tryptophan hydroxylase (dopamine and serotonin synthesis). Deficiency causes cognitive impairment, restless legs syndrome, and pica.
- Epithelial integrity: Glossitis, angular cheilitis, koilonychia, Plummer–Vinson syndrome (oesophageal web, dysphagia, iron deficiency triad).
Hepcidin–Ferroportin Axis
Hepcidin is the central regulator of iron homeostasis. In iron-replete states, hepcidin binds ferroportin on enterocytes and macrophages, causing its internalisation and lysosomal degradation, thereby reducing iron absorption and release. In iron deficiency, hepcidin production is suppressed (mediated by decreased BMP-SMAD signalling and increased erythroferrone from erythroid precursors), allowing maximal iron absorption and macrophage iron recycling. In inflammation, IL-6 drives hepcidin production via the JAK-STAT3 pathway, leading to functional iron deficiency — iron is trapped in macrophages and enterocytes, unavailable for erythropoiesis.
Clinical Presentation & Diagnostic Criteria
Symptoms
Iron deficiency may be asymptomatic in early stages. Symptoms include:
- General: Fatigue, weakness, lethargy, reduced exercise tolerance, dyspnoea on exertion.
- Neurological: Poor concentration, impaired memory, irritability, restless legs syndrome (up to 25% of patients with IDA).
- Pica/pagophagia: Compulsive craving for ice, starch, or dirt — highly specific for iron deficiency.
- Dermatological: Pallor (conjunctival, palmar), koilonychia (spoon nails), angular cheilitis, hair loss.
- Oral: Glossitis, atrophic tongue papillae.
- ENT: Dysphagia (Plummer–Vinson syndrome — oesophageal web, typically postmenopausal women).
- Gynaecological: Menorrhagia (may be both cause and consequence).
- Cardiovascular: Tachycardia, palpitations, flow murmur (with severe anaemia).
Diagnostic Criteria
- Iron deficiency: Ferritin <30 µg/L (or ferritin 30–100 µg/L with TSAT <20% and elevated CRP).
- Iron deficiency anaemia: Iron deficiency (as above) PLUS haemoglobin below reference range: <120 g/L (non-pregnant women), <110 g/L (pregnant women), <130 g/L (men).
- Functional iron deficiency: TSAT <20% with ferritin >100 µg/L in the context of chronic inflammation or erythropoiesis-stimulating agent (ESA) therapy.
Differential Diagnosis of Microcytic Anaemia
| Condition | Ferritin | TSAT | RDW | Hb Electrophoresis |
|---|---|---|---|---|
| Iron deficiency anaemia | ↓ | ↓ | ↑ | Normal |
| Thalassaemia trait (α or β) | Normal/↑ | Normal | Normal/↑ slightly | ↑ HbA2 (β), abnormal (α) |
| Anaemia of chronic disease | Normal/↑ | ↓ | Normal | Normal |
| Sideroblastic anaemia | ↑ | ↑ | ↑ | Normal |
| Lead poisoning | Normal/↑ | Normal/↓ | ↑ | Normal |
Management — Oral & IV Iron Replacement
The goals of iron replacement therapy are: (1) correct anaemia and restore haemoglobin to target; (2) replenish iron stores (ferritin >100 µg/L); and (3) identify and treat the underlying cause. Concurrent investigation and treatment of the underlying cause is essential — iron replacement alone without addressing ongoing losses or malabsorption will result in recurrent deficiency.
Oral Iron — First-Line Therapy
Oral iron is the initial treatment for most patients with iron deficiency without severe anaemia, malabsorption, intolerance, or need for rapid repletion.
- Take on an empty stomach (1 hour before or 2 hours after food) for maximal absorption.
- Pair with vitamin C (250–500 mg ascorbic acid) to enhance non-haem iron absorption.
- Separate from tea, coffee, calcium supplements, and antacids/PPIs by at least 2 hours.
- Alternate-day dosing (once every 2 days) reduces hepcidin-mediated suppression and improves fractional absorption by up to 40%, while halving GI side effects.
- Expect reticulocyte rise by days 5–10 and haemoglobin rise of 10–20 g/L by 2–4 weeks. Recheck FBE and iron studies at 4–8 weeks.
When to Consider IV Iron
- Oral iron intolerance (refractory GI side effects).
- Inadequate response to oral iron after 4–8 weeks (haemoglobin rise <10 g/L).
- Malabsorption (coeliac disease, IBD, bariatric surgery, atrophic gastritis).
- Chronic kidney disease (stage 4–5, particularly on erythropoiesis-stimulating agents).
- Need for rapid repletion: perioperative, severe anaemia (Hb <70–80 g/L), late pregnancy (3rd trimester), chronic heart failure.
- Ongoing blood loss exceeding oral iron replacement capacity.
- Inflammatory bowel disease with active disease.
IV Iron Preparations — Australian Formulary
Monitoring Response to Treatment
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Pasricha S-R, Tye-Din J, Muckenthaler MU, Swinkels DW. Iron deficiency. Lancet. 2021;397(10270):233–248.
- 2. Lopez A, Cacoub P, Macdougall IC, Peyrin-Biroulet L. Iron deficiency anaemia. Lancet. 2016;387(10021):907–916.
- 3. National Health and Medical Research Council. Nutrient Reference Values for Australia and New Zealand: Iron. Canberra: NHMRC; 2006 (updated 2020).
- 4. Australian Institute of Health and Welfare. Iron deficiency anaemia in Australia. Cat. no. PHE 262. Canberra: AIHW; 2020.
- 5. RACGP. Iron deficiency: investigation and management. Red Book — Guidelines for preventive activities in general practice. 9th edition. Melbourne: RACGP; 2016.
- 6. Goddard AF, James MW, McIntyre AS, Scott BB. Guidelines for the management of iron deficiency anaemia. Gut. 2011;60(10):1309–1316.
- 7. Stoffel NU, Cercamondi CI, Brittenham G, et al. Iron absorption from oral iron supplements given on consecutive versus alternate days and as single morning doses versus twice-daily split dosing in iron-depleted women: two open-label, randomised controlled trials. Lancet Haematol. 2017;4(11):e524–e533.
- 8. Kidney Disease: Improving Global Outcomes (KDIGO). KDIGO 2012 clinical practice guideline for anemia in CKD. Kidney Int Suppl. 2012;2(4):279–335.
- 9. Dignass AU, Gasche C, Bettenworth D, et al. European consensus on the diagnosis and management of iron deficiency and anaemia in inflammatory bowel diseases. J Crohns Colitis. 2015;9(3):211–222.
- 10. RHDAustralia. Diagnosis, management and prevention of hookworm infection in Aboriginal and Torres Strait Islander communities. Darwin: Menzies School of Health Research; 2021.
- 11. Quek J, Tay D, Allard S, et al. Intravenous iron: a practical guide for Australia. Intern Med J. 2023;53(5):670–678.
- 12. Australian Commission on Safety and Quality in Health Care. Blood and Blood Products Clinical Care Standard. Sydney: ACSQHC; 2022.
- 13. NHMRC. Clinical Practice Guidelines: Pregnancy Care. Canberra: Australian Government Department of Health; 2018.
- 14. Ziegler EE. Consumption of cow's milk as a cause of iron deficiency in infants and toddlers. Nutr Rev. 2011;69(Suppl 1):S37–S42.