📋 Key Information Summary
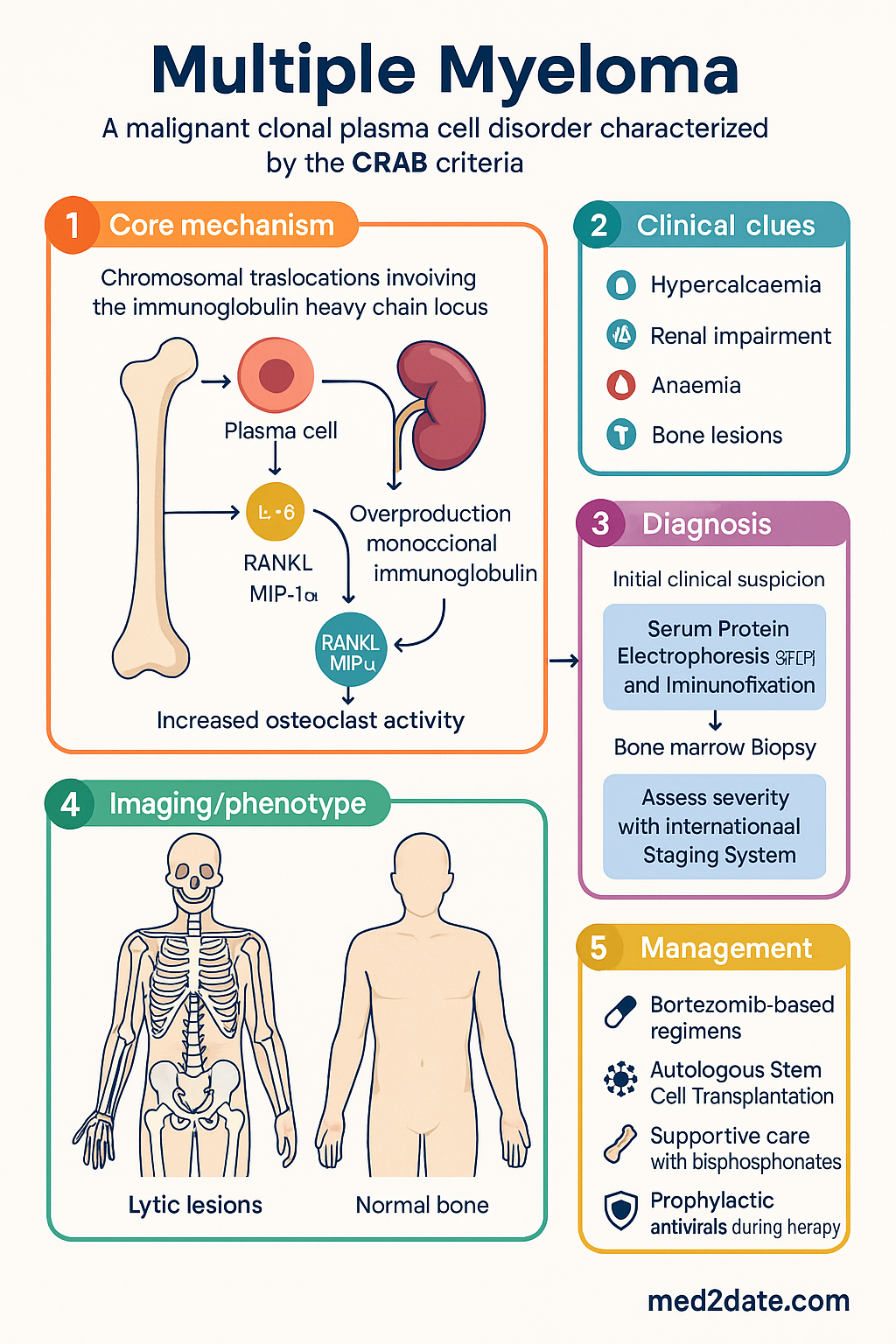
- Multiple myeloma (MM) is a malignant clonal plasma cell disorder characterised by end-organ damage defined by the CRAB criteria: hyperCalcaemia, Renal impairment, Anaemia, and Bone lesions.
- Approximately 1,800 new cases are diagnosed annually in Australia, with a median age at diagnosis of 69 years and a slight male predominance.
- Essential initial investigations include serum protein electrophoresis (SPEP) with immunofixation, serum free light chain (sFLC) assay, 24-hour urine protein electrophoresis, bone marrow biopsy, and whole-body low-dose CT (WBLDCT) or PET-CT.
- The International Staging System (ISS) and revised ISS (R-ISS) incorporating cytogenetics are standard for prognostication.
- Smouldering multiple myeloma (SMM) is an asymptomatic precursor state with a 10% annual progression risk in the first 5 years; close observation remains standard except for very high-risk cases.
- First-line therapy for transplant-eligible patients is induction with a bortezomib-based triplet (e.g., bortezomib, lenalidomide, dexamethasone [VRd]) followed by autologous stem cell transplantation (ASCT).
- For transplant-ineligible patients, continuous lenalidomide and dexamethasone (Rd) or bortezomib-based regimens are standard.
- The PBS lists bortezomib, lenalidomide, and dexamethasone as Authority Required items for first-line and relapsed MM.
- Supportive care is critical and includes bisphosphonates (zoledronic acid) for bone disease, prophylactic antivirals (aciclovir) during bortezomib therapy, and thromboprophylaxis with lenalidomide.
- Aboriginal and Torres Strait Islander peoples have a higher incidence and mortality from myeloma, often presenting at a younger age and with more advanced disease.
- Renal impairment is common; all nephrotoxic agents require dose adjustment, and hydration is paramount in hypercalcaemia.
Introduction & Australian Epidemiology
Multiple myeloma is a malignant proliferation of clonal plasma cells in the bone marrow, leading to the overproduction of monoclonal immunoglobulin (M-protein) or its components (free light chains). This results in a spectrum of clinical manifestations classically summarised by the CRAB criteria, which define end-organ damage: hypercalcaemia, renal insufficiency, anaemia, and bone lesions. It is part of a continuum of plasma cell disorders, ranging from monoclonal gammopathy of undetermined significance (MGUS) to smouldering myeloma and finally to symptomatic myeloma requiring therapy.
In Australia, multiple myeloma accounts for approximately 1.5% of all new cancer diagnoses and 2% of cancer deaths. The Australian Institute of Health and Welfare (AIHW) estimated 1,820 new cases in 2023 (1,020 males, 800 females), with an age-standardised incidence rate of 6.8 per 100,000 persons. The median age at diagnosis is 69 years. Prognosis has improved significantly over the past two decades with the introduction of novel agents, with 5-year relative survival now exceeding 55%.
Pathogenesis & CRAB Criteria
Multiple myeloma arises from a post-germinal centre B-cell that has undergone somatic hypermutation and class-switch recombination. Key oncogenic events include chromosomal translocations involving the immunoglobulin heavy chain locus (e.g., t(11;14), t(4;14), t(14;16)), hyperdiploidy, and mutations in genes such as NRAS, KRAS, TP53, and DIS3. The bone marrow microenvironment, including cytokines like IL-6 and interactions with stromal cells, plays a crucial role in tumour survival, drug resistance, and the development of osteolytic bone disease.
The CRAB criteria define the myeloma-defining events that necessitate the initiation of treatment:
| Criterion | Definition & Pathophysiology | Clinical Features |
|---|---|---|
| C - Hypercalcaemia | Corrected serum calcium >2.75 mmol/L. Caused by osteoclast-activating factors (e.g., RANKL, MIP-1α) produced by myeloma cells and stroma. | Polyuria, polydipsia, constipation, confusion, renal impairment, shortened QTc on ECG. |
| R - Renal Impairment | Creatinine clearance <40 mL/min or serum creatinine >177 μmol/L. Primarily due to cast nephropathy (light chain precipitation in tubules) and less commonly light chain deposition disease or amyloidosis. | Oedema, fatigue, elevated creatinine. Urine dipstick may be negative for protein as light chains are not detected. |
| A - Anaemia | Normocytic normochromic anaemia, typically haemoglobin <100 g/L or >20 g/L below normal. Caused by marrow infiltration, renal failure (reduced EPO), and chronic disease. | Fatigue, dyspnoea, pallor, tachycardia. |
| B - Bone Lesions | One or more osteolytic lesions on skeletal survey, WBLDCT, or PET-CT. Due to uncoupled bone remodelling with osteoclast activation and osteoblast suppression. | Bone pain (especially back/ribs), pathological fractures, spinal cord compression. Osteoporosis may also be present. |
The presence of one or more CRAB criteria in a patient with evidence of clonal plasma cells ≥10% in the bone marrow or a biopsy-proven plasmacytoma confirms the diagnosis of symptomatic multiple myeloma requiring treatment.
Investigations (SPEP, Biopsy, Skeletal Survey)
A comprehensive diagnostic workup is essential to confirm the diagnosis, assess tumour burden, and evaluate for end-organ damage.
- Serum Protein Electrophoresis (SPEP) and Immunofixation (sIFE): To detect and characterise the M-protein (IgG, IgA, or light chain only). Available in all major labs.
- Serum Free Light Chain (sFLC) Assay: Measures kappa and lambda free light chains and calculates the ratio. Essential for diagnosis and response assessment, especially in light-chain only disease. MBS item 69460.
- 24-hour Urine for Electrophoresis and Immunofixation (uIFE): Quantifies Bence Jones proteinuria. Critical for cast nephropathy risk assessment.
Assess plasma cell percentage (≥10% diagnostic, but ≥60% is a myeloma-defining event), morphology, and immunophenotype by flow cytometry (CD38+, CD138+, CD19-, CD56+). Cytogenetics by FISH on purified plasma cells is mandatory for risk stratification (del(17p), t(4;14), t(14;16), 1q gain).
Whole-Body Low-Dose CT (WBLDCT): Now the standard of care over plain skeletal survey (MBS item 56807). Superior sensitivity for detecting osteolytic lesions and assessing fracture risk. PET-CT (MBS item 61422): Useful for assessing metabolically active disease and extramedullary plasmacytomas.
Full blood count, serum calcium (corrected), renal function (eGFR), LDH, beta-2 microglobulin, albumin. Consider cardiac MRI if AL amyloidosis is suspected (NT-proBNP, troponin).
Staging (ISS) & Smouldering Myeloma
The International Staging System (ISS) and its revision (R-ISS) are the standard prognostic tools in multiple myeloma.
Revised ISS (R-ISS) incorporates high-risk cytogenetics (del(17p), t(4;14), t(14;16) by FISH) and elevated LDH to further refine risk.
Smouldering Multiple Myeloma (SMM)
SMM is an asymptomatic precursor state defined by serum M-protein ≥30 g/L and/or clonal bone marrow plasma cells 10-60% without CRAB criteria or myeloma-defining events. The standard of care is observation with 3-6 monthly clinical and laboratory review, as the risk of progression to symptomatic myeloma is approximately 10% per year for the first 5 years.
Management (Bortezomib, Lenalidomide, Dexamethasone, ASCT)
Treatment is stratified by transplant eligibility, patient fitness, and risk status. Goals are to achieve deep, durable remissions while maintaining quality of life.
First-Line Therapy for Transplant-Eligible Patients
The standard induction regimen is VRd (bortezomib, lenalidomide, dexamethasone) for 4-6 cycles, followed by stem cell harvest and high-dose melphalan with autologous stem cell transplantation (ASCT). Maintenance therapy with lenalidomide is standard post-ASCT.
First-Line Therapy for Transplant-Ineligible Patients
Continuous lenalidomide and low-dose dexamethasone (Rd) until progression is a standard regimen. For patients with renal impairment or high-risk disease, a bortezomib-based triplet (e.g., VMP: bortezomib, melphalan, prednisolone) is often preferred.
Autologous Stem Cell Transplantation (ASCT)
ASCT remains a standard consolidative therapy for eligible patients (typically age ≤70-75 with adequate organ function). It is not curative but improves progression-free survival. It involves high-dose melphalan (200 mg/m²) followed by re-infusion of previously harvested autologous CD34+ stem cells.
Relapsed/Refractory Disease
Choice of regimen at relapse depends on the nature of prior therapy, duration of remission, patient fitness, and risk status. Novel agents available via clinical trials or PBS (with authority) include carfilzomib, ixazomib, daratumumab (anti-CD38), elotuzumab, and pomalidomide.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Australian Institute of Health and Welfare (AIHW). Cancer data in Australia. Canberra: AIHW; 2023.
- 2. Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538-48.
- 3. Palumbo A, Avet-Loiseau H, Oliva S, et al. Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group. J Clin Oncol. 2015;33(26):2863-9.
- 4. Durie BGM, Hoering A, Abidi MH, et al. Bortezomib with lenalidomide and dexamethasone versus lenalidomide and dexamethasone alone in patients with newly diagnosed myeloma without intent for immediate autologous stem-cell transplant (SWOG S0777): a randomised, open-label, phase 3 trial. Lancet. 2017;389(10068):519-527.
- 5. Attal M, Lauwers-Cances V, Hulin C, et al. Lenalidomide, Bortezomib, and Dexamethasone with Transplantation for Myeloma. N Engl J Med. 2017;376(14):1311-1320.
- 6. Australian Government Department of Health. Pharmaceutical Benefits Scheme (PBS). Bortezomib, Lenalidomide. Canberra; 2024.
- 7. Sanchorawala V. Systemic Light Chain Amyloidosis. N Engl J Med. 2021;385(17):1582-1593.
- 8. Ludwig H, Delforge M, Facon T, et al. Prevention and management of adverse events of novel agents in multiple myeloma: a consensus of the European Myeloma Network. Leukemia. 2018;32(7):1542-1560.
- 9. Conyers R, Costello H, LaBrooy J, et al. Cancer outcomes for Aboriginal and Torres Strait Islander Australians: a national data linkage study. Med J Aust. 2022;216(1):30-35.
- 10. RACGP. Guidelines for preventive activities in general practice (The Red Book). 9th edn. East Melbourne: RACGP; 2016.