📋 Key Information Summary
- Factor V Leiden (FVL) is the most common inherited thrombophilia, present in ~5% of Australian Caucasians, causing resistance to activated protein C (APC).
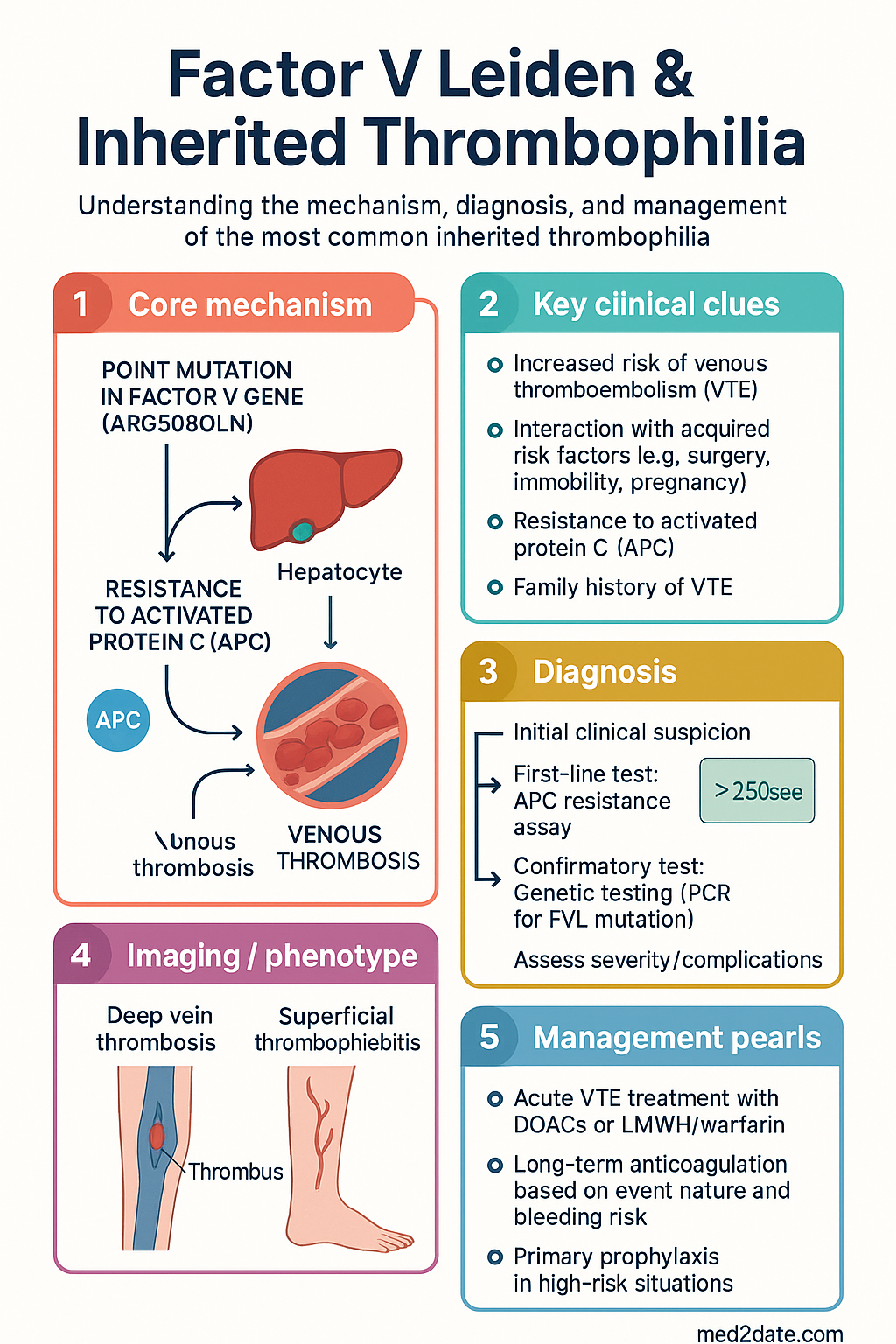
- Heterozygous FVL increases venous thromboembolism (VTE) risk 3–8 fold; homozygous increases risk 50–80 fold.
- Clinical expression of VTE requires interaction with acquired risk factors (e.g., surgery, immobility, pregnancy, OCP).
- Routine thrombophilia screening is NOT recommended for the general population or before starting combined oral contraception.
- Testing is indicated after a first unprovoked VTE, VTE at young age (<50), unusual site, strong family history, or pregnancy morbidity.
- Interpretation requires knowledge of acute thrombosis, anticoagulant therapy, and pregnancy status, which can affect results.
- Initial VTE treatment is with direct oral anticoagulants (DOACs) or low-molecular-weight heparin (LMWH)/warfarin, same as for non-carriers.
- Long-term anticoagulation duration depends on whether the VTE was provoked and bleeding risk, not solely on FVL status.
- For heterozygous FVL, primary prophylaxis with LMWH is recommended only in high-risk transient situations (e.g., major surgery with other risks).
- Homozygous FVL or compound heterozygosity requires more aggressive thromboprophylaxis in at-risk settings.
- Pregnancy management involves risk stratification; prophylactic LMWH is reserved for those with additional risk factors (e.g., personal VTE history).
- Education on modifiable risk factors (avoid dehydration, prolonged immobility, smoking cessation) is a cornerstone of management.
Introduction & Australian Epidemiology
Factor V Leiden (FVL) is the most common inherited thrombophilia, resulting from a point mutation in the Factor V gene (Arg506Gln) that renders Factor Va resistant to inactivation by activated protein C (APC). This leads to a prothrombotic state primarily affecting the venous system.
In Australia, the prevalence of heterozygous FVL is approximately 5% in individuals of Northern European (Caucasian) descent, mirroring rates in the UK and North America. It is rare in Indigenous Australians, Asian, and African populations. Homozygous FVL occurs in ~0.1% of the Caucasian population. It is a significant contributor to the burden of venous thromboembolism (VTE), which affects 1–2 per 1000 Australian adults annually. Understanding its mechanism, appropriate testing, and management is essential to balance thrombotic risk against the harms of unnecessary long-term anticoagulation.
Mechanism (APC Resistance)
The haemostatic system maintains a balance between pro-coagulant and anti-coagulant pathways. Activated protein C (APC) is a critical natural anticoagulant that, with its cofactor protein S, proteolytically inactivates Factors Va and VIIIa, thereby limiting thrombin generation.
The FVL mutation (a G-to-A substitution at nucleotide 1691) results in an arginine to glutamine substitution at position 506 of the Factor V molecule. This alters one of the key APC cleavage sites on Factor Va. While Factor Va still functions normally as a pro-cofactor, its inactivation by APC is markedly slowed. This leads to prolonged prothrombinase complex activity, enhanced thrombin generation, and a hypercoagulable state.
Prevalence & Risk of VTE
Population Prevalence
FVL is predominantly found in populations of Northern European origin. In Australia, this translates to a carrier frequency of approximately 1 in 20 in the Caucasian community. The mutation is largely absent in Indigenous Australian, East Asian, and African populations.
VTE Risk Quantification
The thrombotic risk is modulated by zygosity and the presence of acquired triggers.
| Genotype | Baseline Annual VTE Risk | Relative Risk (vs. non-carriers) | Interaction with OCP |
|---|---|---|---|
| Heterozygous FVL | ~0.5% | 3–8x | Multiplicative: ~35x increased risk |
| Homozygous FVL | ~1-2% | 50–80x | Very high risk; OCP contraindicated |
Most VTE events in FVL carriers occur in the context of additional acquired risk factors (e.g., surgery, trauma, immobilisation, long-haul travel, pregnancy, malignancy, OCP use). The lifetime risk of VTE is not 100%, and many carriers remain asymptomatic.
Testing & Interpretation
Indications for Testing
- First unprovoked VTE at any age.
- VTE at a young age (<50 years), even if provoked.
- VTE in an unusual site (cerebral, mesenteric, hepatic veins).
- Strong family history of VTE (first-degree relative with VTE <50y).
- Recurrent miscarriage (≥3 first trimester or ≥1 second trimester) after exclusion of other causes.
- Women with VTE in pregnancy or on OCP, to guide future management.
Testing Methodology & Pitfalls
Initial testing is with a functional clotting assay: the APC Resistance assay (with V-deficient plasma). If abnormal, confirmation is by genetic testing (PCR for the FVL mutation). MBS Item 65090 covers genetic testing for heritable thrombophilia when clinically indicated.
- Do NOT test during an acute thrombotic event or within 2-4 weeks of resolution.
- Do NOT test while on warfarin (DOACs may also interfere; seek haematology advice). LMWH does not interfere with genetic testing.
- Pregnancy and OCP use can affect functional APC resistance assays but not genetic tests.
Interpretation in Context
A positive result must be interpreted in conjunction with the clinical scenario. It does not prove causality for an individual event but informs lifetime risk and management of future risk situations. Genetic counselling is recommended for homozygous or compound heterozygous states. Cascade testing of first-degree relatives may be considered after discussion of implications.
Management (Anticoagulation & Prophylaxis)
Treatment of Acute VTE
Management of an acute VTE in a patient with FVL is identical to that for a patient without a known thrombophilia. First-line therapy in Australia is with a direct oral anticoagulant (DOAC: apixaban, rivaroxaban) or low-molecular-weight heparin (LMWH) bridging to warfarin. Choice depends on clinical context (e.g., cancer, renal function, patient preference).
Long-Term Anticoagulation & Secondary Prevention
The decision to continue anticoagulation beyond 3–6 months is based on the nature of the index event (provoked vs. unprovoked), bleeding risk (using a validated score like VTE-BLEED), and patient preference—not the presence of FVL alone.
- Provoked VTE: Usually 3–6 months of anticoagulation. FVL status does not typically mandate extension.
- Unprovoked VTE: Consider indefinite anticoagulation if bleeding risk is low. FVL heterozygosity is a weak argument for extension on its own; homozygosity may support indefinite therapy.
- Recurrent VTE: Generally warrants indefinite anticoagulation regardless of FVL status.
Primary Prophylaxis in At-Risk Situations
Prophylaxis is not recommended for asymptomatic carriers in low-risk daily life. It is targeted to high-risk transient periods.
| Clinical Scenario | Heterozygous FVL | Homozygous FVL |
|---|---|---|
| Major elective surgery (e.g., hip/knee replacement) | Standard VTE prophylaxis (LMWH/DOAC) as per hospital protocol. | Extended prophylaxis (e.g., 28-35 days post-op) with LMWH/DOAC. |
| Medical admission with acute illness & immobility | Standard prophylactic LMWH (e.g., enoxaparin 40 mg SC daily). | Consider higher prophylactic dose (e.g., enoxaparin 40 mg SC BD) or treatment-dose prophylaxis. |
| Long-haul travel (>8 hours) | General measures (hydration, mobility). No routine LMWH. | Consider a single dose of LMWH (e.g., enoxaparin 40 mg SC) pre-flight. |
Special Populations
Pregnancy
VTE risk is increased 5-10 fold in pregnancy. Management requires individual risk assessment.
- Heterozygous FVL, no personal VTE history: No routine thromboprophylaxis. Encourage mobilisation, hydration. Consider LMWH post-partum for 6 weeks if additional risk factors (e.g., BMI>30, age>35, pre-eclampsia).
- Heterozygous FVL with prior provoked VTE: Consider LMWH during pregnancy and 6 weeks post-partum.
- Heterozygous FVL with prior unprovoked VTE: Prophylactic or intermediate-dose LMWH throughout pregnancy and 6 weeks post-partum.
- Homozygous FVL: High risk. Prophylactic or intermediate-dose LMWH throughout pregnancy and 6-12 weeks post-partum.
Warfarin is teratogenic; DOACs are contraindicated. LMWH (e.g., enoxaparin) is the drug of choice.
Paediatrics
VTE in children is rare. Most paediatric VTE is provoked by central lines or other strong triggers. FVL testing should be considered in a child with a spontaneous VTE or strong family history. Management is guided by paediatric haematology. Prophylaxis is not routine for asymptomatic children with FVL.
Renal Impairment
For CrCl <30 mL/min, LMWH (enoxaparin) requires dose reduction (e.g., 20 mg daily for prophylaxis). Unfractionated heparin (UFH) may be preferred in severe renal failure. DOACs: Apixaban and rivaroxaban require dose adjustment in moderate-severe impairment; rivaroxaban is contraindicated if CrCl <15 mL/min.
Immunocompromised / Cancer
Cancer-associated VTE has a high recurrence risk. LMWH is often preferred over DOACs for long-term therapy, especially with mucosal tumours or GI lesions. FVL status does not change first-line management, which is driven by the cancer.
Aboriginal and Torres Strait Islander Health Considerations
Factor V Leiden prevalence is very low in Aboriginal and Torres Strait Islander populations. VTE in this population is more likely related to acquired risk factors (e.g., infections, trauma, post-partum state, chronic disease). Clinicians should:
📚 References
- 1. Kujovich JL. Factor V Leiden thrombophilia. Genet Med. 2011;13(1):1-16.
- 2. Tran HA, Gibbs H, Merriman E, et al. New guidelines from the Thrombosis and Haemostasis Society of Australia and New Zealand for the diagnosis and management of venous thromboembolism. Med J Aust. 2019;210(5):227-235.
- 3. Australian Institute of Health and Welfare (AIHW). Venous thromboembolism in Australia. Cat. no. PHE 268. Canberra: AIHW; 2021.
- 4. National Health and Medical Research Council (NHMRC). Clinical practice guideline for the diagnosis and management of venous thromboembolism. Canberra: NHMRC; 2019.
- 5. Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice. 10th edn. East Melbourne: RACGP; 2024.
- 6. Middeldorp S. Evidence-based approach to thrombophilia testing. J Thromb Thrombolysis. 2011;31(3):275-81.
- 7. Bates SM, et al. VTE, thrombophilia, antithrombotic therapy, and pregnancy: CHEST Guideline and Expert Panel Report. Chest. 2016;149(5):1128-1157.
- 8. Baglin T, et al. British Committee for Standards in Haematology. Guidelines on the investigation and management of venous thrombosis at unusual sites. Br J Haematol. 2012;159(1):28-38.
- 9. Australian Technical Advisory Group on Immunisation (ATAGI). Australian immunisation handbook. Australian Government Department of Health; 2024. (Referenced for timing of vaccination around LMWH injections).
- 10. The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG). Management of inherited thrombophilia in pregnancy. C-Obs 65. Melbourne: RANZCOG; 2020.
- 11. Eikelboom JW, Weitz JI. New anticoagulants. Circulation. 2010;121(13):1523-1532. (For DOAC mechanism and dosing context).
- 12. RHDAustralia (Australian Rheumatic Heart Disease Knowledge Hub). Culturally safe clinical guidelines. Darwin: Menzies School of Health Research; 2022. (Referenced for ATSI communication principles).