📋 Key Information Summary
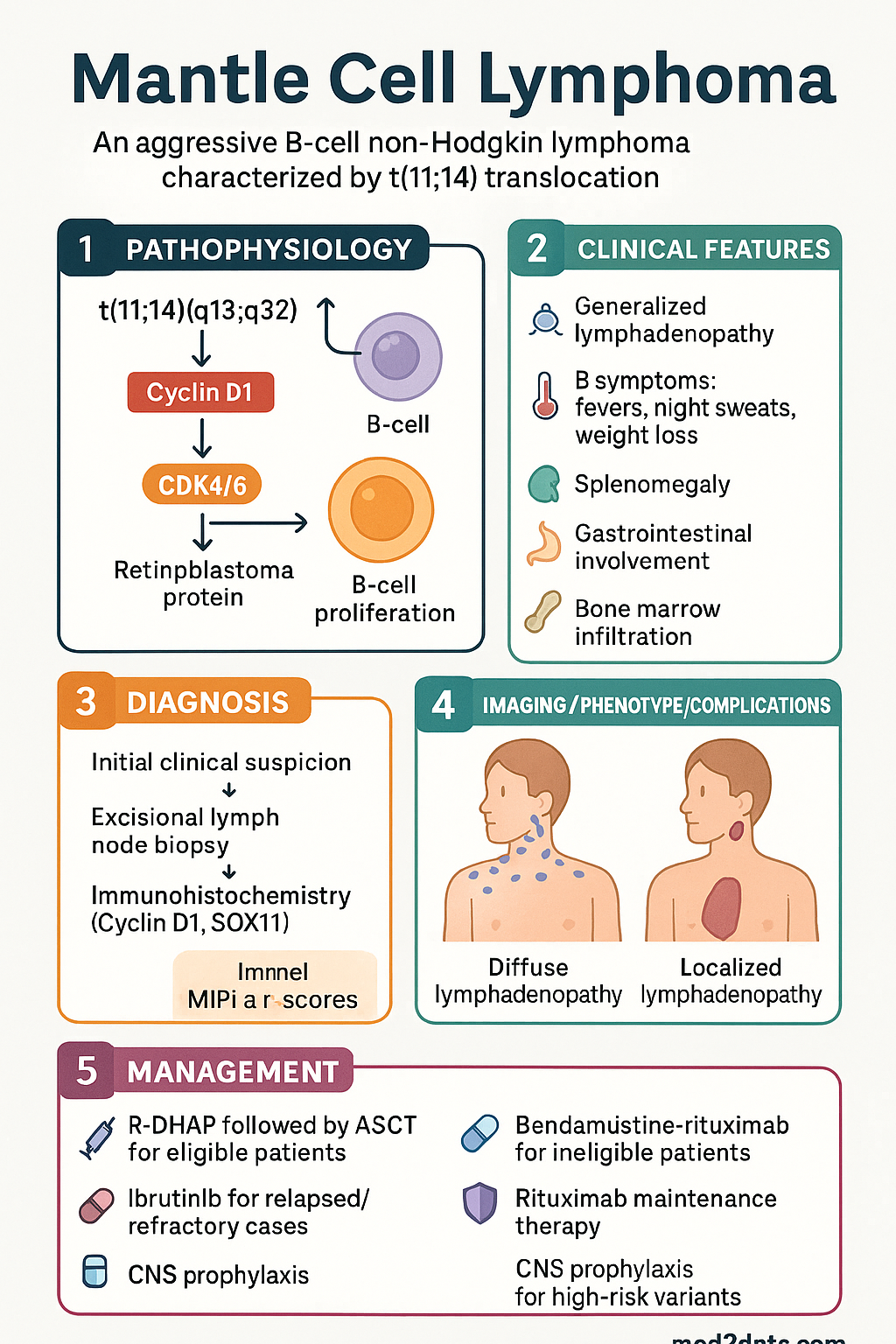
- Mantle cell lymphoma (MCL) is an aggressive B-cell non-Hodgkin lymphoma driven by the t(11;14)(q13;q32) translocation causing cyclin D1 (CCND1) overexpression; accounts for 3–10 % of all NHL in Australia.
- Median age at diagnosis 65–70 years; male-to-female ratio approximately 3:1. Most patients present with Ann Arbor Stage III–IV disease with widespread lymphadenopathy and extranodal involvement.
- SOX11 positivity by immunohistochemistry is present in ~90 % of conventional MCL and helps distinguish MCL from other CD5-positive B-cell lymphomas, particularly when cyclin D1 is equivocal.
- Blastoid and pleomorphic morphological variants carry significantly worse prognosis (median OS 1–2 years) and mandate CNS prophylaxis and more intensive regimens.
- For transplant-eligible patients, R-DHAP ×3 followed by autologous stem-cell transplant (ASCT) with rituximab maintenance is the standard-of-care consolidation approach.
- For transplant-ineligible (elderly/unfit) patients, bendamustine-rituximab (BR) or R-CHOP/R-CVP followed by rituximab maintenance is preferred.
- Ibrutinib (Imbruvica®), a BTK inhibitor, is PBS Authority Required in Australia for relapsed/refractory MCL after ≥1 prior therapy; it has transformed salvage outcomes.
- Rituximab maintenance (every 2 months for 3 years) after induction improves progression-free survival and is standard for all fit patients.
- MIPI (MCL International Prognostic Index) and MIPI-c (combined with Ki-67) stratify risk and guide treatment intensity, including consideration of early ASCT or novel agents.
- CNS prophylaxis with intrathecal methotrexate or high-dose systemic methotrexate is recommended for blastoid variant, elevated LDH with Ki-67 >30 %, or CNS-IPI ≥4.
- Aboriginal and Torres Strait Islander peoples may face barriers to timely specialist referral and access to SCT or novel agents; equitable pathways should be proactively established.
- Treatment must be delivered in a multidisciplinary haematology setting; refer all patients to an accredited haematologist and consider clinical trial enrolment at every stage.
Introduction & Australian Epidemiology
Mantle cell lymphoma (MCL) is an uncommon but clinically significant B-cell non-Hodgkin lymphoma (NHL) that represents approximately 3–10 % of all NHL diagnoses. It is defined by a characteristic chromosomal translocation, t(11;14)(q13;q32), which juxtaposes the CCND1 (cyclin D1) gene under the immunoglobulin heavy-chain enhancer, resulting in constitutive cyclin D1 overexpression and dysregulated cell-cycle progression through the G1/S checkpoint.
In Australia, the estimated age-standardised incidence is 0.7–1.0 per 100 000 person-years. There were approximately 400–500 new diagnoses nationally in recent Cancer Australia data. MCL shows a striking male predominance (male:female ratio ~3:1) and a median age at diagnosis of 65–70 years. The disease has a heterogeneous clinical course: although historically considered uniformly aggressive, a subset of patients with non-nodal leukaemic MCL, SOX11-negative disease, and low Ki-67 proliferative index may follow an indolent course lasting years before requiring treatment.
Despite advances in therapy—particularly the introduction of Bruton tyrosine kinase (BTK) inhibitors such as ibrutinib—MCL remains incurable for the majority of patients, with median overall survival approximately 5–7 years in the modern era. Ongoing clinical trials investigating chimeric antigen receptor T-cell (CAR-T) therapy, bispecific antibodies, and next-generation BTK inhibitors offer hope for further improvement. This guideline provides an evidence-based overview of MCL pathogenesis, diagnosis, staging, and management in the Australian context, with attention to PBS-listed agents, MBS-funded investigations, and equity considerations for Aboriginal and Torres Strait Islander peoples.
Pathogenesis (Cyclin D1, t(11;14))
The t(11;14)(q13;q32) Translocation
The defining molecular event in MCL is the balanced chromosomal translocation t(11;14)(q13;q32). This rearrangement places the CCND1 gene on chromosome 11q13 under the control of the immunoglobulin heavy-chain (IGH) enhancer on chromosome 14q32, resulting in constitutive overexpression of cyclin D1 protein. This translocation is detectable by fluorescence in situ hybridisation (FISH) in >95 % of MCL cases and is considered the hallmark genetic abnormality.
Cyclin D1 and Cell-Cycle Dysregulation
Cyclin D1 is a regulatory subunit of cyclin-dependent kinases CDK4 and CDK6. Overexpression of cyclin D1 promotes phosphorylation of the retinoblastoma (Rb) protein, releasing E2F transcription factors and driving uncontrolled G1-to-S phase transition. This bypasses normal cell-cycle checkpoints, facilitating unrestrained proliferation of the malignant B-cell clone. Additional cooperating mutations in DNA damage response pathways (e.g., TP53, ATM) and cell survival pathways (NOTCH1, NF-κB) further contribute to disease aggressiveness and treatment resistance.
SOX11 and Subtypes
SOX11 (SRY-box transcription factor 11) is expressed in approximately 90 % of conventional MCL. SOX11-positive tumours typically follow an aggressive clinical course with nodal presentation. Conversely, SOX11-negative MCL, which often presents with peripheral blood involvement (leukaemic non-nodal MCL), bone marrow infiltration, and splenomegaly without significant lymphadenopathy, may pursue an indolent course for years. SOX11-negative cases frequently harbour fewer additional genetic aberrations and have a more favourable prognosis if monitored with a watch-and-wait approach.
Key Additional Genetic Alterations
| Gene / Alteration | Frequency in MCL | Functional Consequence |
|---|---|---|
| t(11;14) / CCND1 | >95 % | Cyclin D1 overexpression; cell-cycle drive |
| TP53 mutation / del(17p) | 15–30 % | Loss of tumour suppressor; chemoresistance; worst prognosis |
| ATM mutation / del(11q) | 40–75 % | Impaired DNA damage response; genomic instability |
| NOTCH1 mutation | 10–15 % | Constitutive NOTCH activation; poorer outcome |
| CDKN2A loss | 20–40 % | Loss of p16; enhanced CDK4/6 activity |
| Complex karyotype | 50–70 % | Genomic instability; associated with blastoid variant |
Clinical Features & Staging
Clinical Presentation
MCL most commonly presents in men aged >60 years with advanced-stage disease. Key presenting features include:
- Generalised lymphadenopathy — cervical, axillary, inguinal; often painless and progressive.
- B symptoms — fevers, night sweats, unintentional weight loss >10 % over 6 months; present in 30–50 %.
- Splenomegaly — often massive; more prominent in leukaemic non-nodal variant.
- Gastrointestinal involvement — lymphomatous polyposis of the bowel is a recognised presentation; upper and lower GI endoscopy is recommended at staging even if asymptomatic.
- Bone marrow infiltration — present in >70 % at diagnosis.
- Peripheral blood involvement — circulating lymphoma cells seen in 20–30 %; higher in blastoid and leukaemic variants.
- CNS involvement — rare at presentation (<5 %) but seen in blastoid variant and relapsed disease; symptoms include headache, cranial nerve palsies, altered consciousness.
Morphological Variants
| Variant | Frequency | Features | Prognosis |
|---|---|---|---|
| Classical (small-to-medium cells) | ~75 % | Irregular nuclear contours, dispersed chromatin | Intermediate |
| Blastoid | ~15 % | Larger cells, fine chromatin, high mitotic rate, resembles lymphoblastic lymphoma | Very poor (median OS 1–2 years) |
| Pleomorphic | ~10 % | Marked variation in cell size and shape | Poor |
| Leukaemic non-nodal | ~5 % | Peripheral blood/bone marrow predominant; SOX11-negative; splenomegaly | Indolent course possible |
Ann Arbor Staging (Lugano Classification)
MCL is almost always Stage III or IV at presentation. The Ann Arbor system (modified by the 2014 Lugano Classification) is used:
| Stage | Distribution | Approximate % at Diagnosis |
|---|---|---|
| I | Single lymph node region | <5 % |
| II | ≥2 lymph node regions, same side of diaphragm | 5–10 % |
| III | Lymph node regions on both sides of diaphragm | 10–15 % |
| IV | Diffuse extranodal involvement (bone marrow, liver, GI) | ~75 % |
Prognostic Scoring — MIPI and MIPI-c
The MCL International Prognostic Index (MIPI) uses four variables—age, ECOG performance status, LDH/ULN ratio, and WBC count—to classify patients into low-, intermediate-, and high-risk groups. The MIPI-c incorporates Ki-67 proliferative index for refined stratification:
Investigations (SOX11, Cyclin D1 IHC)
Histopathology & Immunohistochemistry
Diagnosis of MCL requires an excisional lymph node biopsy reviewed by an experienced haematopathologist. Core-needle biopsy may be acceptable if excisional biopsy is not feasible, but diagnostic accuracy is reduced. The following immunohistochemical (IHC) panel is essential:
Cytogenetics & FISH
Molecular Studies
Baseline Staging Investigations
- CT chest/abdomen/pelvis with IV contrast (MBS item 56809) — standard anatomical staging.
- PET-CT (MBS item 61651) — recommended by Lugano Classification for FDG-avid lymphomas including MCL. Baseline SUVmax and Deauville score at interim scan inform response assessment.
- Bone marrow aspirate & trephine biopsy — confirm marrow involvement; morphology, IHC (cyclin D1, CD20, CD5), flow cytometry, and FISH on marrow sample.
- Upper & lower GI endoscopy — recommended for all patients given ~30 % GI involvement; lymphomatous polyposis may be present despite absence of GI symptoms.
- Laboratory panel: FBC, LDH, β2-microglobulin, albumin, LFTs, UEC, urate, CMV/EBV serology (pre-therapy).
- Echocardiogram or MUGA scan — baseline cardiac function prior to anthracycline-containing regimens.
- CNS assessment — MRI brain + lumbar puncture with CSF cytology/flow cytometry for blastoid variant, elevated LDH with Ki-67 >30 %, or CNS-IPI ≥4.
Management (R-CHOP, Ibrutinib, SCT)
Treatment Overview
Management of MCL is guided by patient age, fitness (assessed by comprehensive geriatric assessment or transplant eligibility criteria), morphological variant, MIPI/MIPI-c risk score, and TP53 status. The two broad treatment pathways are transplant-eligible (intensive) and transplant-ineligible (non-intensive).
Transplant-Eligible Patients (Age ≤65–70, Fit)
The Nordic MCL2 protocol or R-DHAP-based induction followed by ASCT is the standard-of-care for transplant-eligible patients:
Alternative induction for transplant-eligible patients: Nordic MCL3 protocol — R-maxi-CHOP alternating with R-HD-cytarabine × 6 cycles. Some Australian centres prefer this regimen when cisplatin is contraindicated.
Transplant-Ineligible Patients (Elderly or Comorbid)
Key Drug Cards
Relapsed / Refractory MCL
Relapsed MCL carries a poor prognosis with conventional salvage chemotherapy. BTK inhibitors have transformed outcomes:
- Ibrutinib monotherapy — first-choice salvage in R/R MCL; PBS Authority Required (≥1 prior line). ORR ~68 %, median PFS ~14 months.
- Acalabrutinib — second-generation BTK inhibitor with improved selectivity; similar efficacy, potentially fewer cardiac events. Not PBS-listed for MCL currently.
- Zanubrutinib — another next-generation BTK inhibitor; emerging data in MCL. Not PBS-listed for MCL.
- Lenalidomide + Rituximab (R²) — option for patients intolerant to BTK inhibitors. Lenalidomide is PBS-listed for myeloma; off-label use in MCL requires private script or authority negotiation.
- CAR-T cell therapy (brexucabtagene autoleucel, Tecartus®) — TGA-approved for R/R MCL after ≥2 prior lines including a BTK inhibitor. Available at selected Australian centres (e.g., Peter MacCallum, RPA, Royal Adelaide). Significant toxicity risk (CRS, ICANS) — specialised centre management required.
- Clinical trials — always consider enrolment for R/R MCL; bispecific antibodies (glofitamab, epcoritamab), ADCs, and combination BTK inhibitor trials are ongoing in Australia.
CNS Prophylaxis
Intrathecal methotrexate dose: 12–15 mg (adjust for body weight if <50 kg). Administer via lumbar puncture at each induction cycle. For patients receiving R-DHAP, intrathecal cytarabine 50 mg is an alternative. High-dose systemic methotrexate (3–3.5 g/m² IV) achieves therapeutic CSF levels and is preferred when blastoid morphology, high Ki-67, or elevated LDH with CNS-IPI ≥4.
Monitoring During & After Treatment
- Response assessment: PET-CT (Deauville criteria) at interim (after 2–3 cycles) and end-of-treatment. CT alone if PET unavailable.
- Minimal residual disease (MRD): Not yet standard-of-care but increasingly used. Sensitive PCR or NGS-based assays detect t(11;14) in blood/bone marrow. MRD negativity post-ASCT correlates with longer PFS. Consider at selected centres.
- Ongoing surveillance: Clinical review every 3 months for 2 years, then every 6 months for 3 years, then annually. CT every 6 months for 2 years, then annually for 3 years.
- Ibrutinib monitoring: FBC every 2 weeks for first 3 months, then monthly. Monitor for atrial fibrillation (ECG at baseline and periodically), bleeding, hypertension, arthralgia, infection risk. Manage drug interactions with pharmacist input.
- Rituximab maintenance: Monitor immunoglobulin levels; IV immunoglobulin replacement if IgG <4 g/L with recurrent infections.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Although specific incidence data for MCL in Aboriginal and Torres Strait Islander peoples are limited, NHL as a group is diagnosed at a younger age and at a more advanced stage in Indigenous Australians. Systemic barriers contribute to delayed diagnosis and reduced access to optimal therapy.
📚 References
- 1. Dreyling M, Campo E, Hermine O, et al. Newly diagnosed and relapsed mantle cell lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28(suppl_4):iv62–iv71.
- 2. Cheah CY, Seymour JF, Wang ML. Mantle cell lymphoma. J Clin Oncol. 2016;34(11):1256–1269.
- 3. Hermine O, Hoster E, Walewski J, et al. Addition of high-dose cytarabine to immunochemotherapy before autologous stem-cell transplantation in patients aged 65 years or younger with mantle cell lymphoma (MCL Younger): a randomised, open-label, phase 3 trial of the European Mantle Cell Lymphoma Network. Lancet. 2016;388(10044):565–575.
- 4. Wang ML, Rule S, Martin P, et al. Targeting BTK with ibrutinib in relapsed or refractory mantle-cell lymphoma. N Engl J Med. 2013;369(6):507–516.
- 5. Rummel MJ, Niederle N, Maschmeyer G, et al. Bendamustine plus rituximab versus CHOP plus rituximab as first-line treatment for patients with indolent and mantle-cell lymphomas: an open-label, multicentre, randomised, phase 3 non-inferiority trial. Lancet. 2013;381(9873):1203–1210.
- 6. Hoster E, Dreyling M, Klapper W, et al. A new prognostic index (MIPI) for patients with advanced-stage mantle cell lymphoma. Blood. 2008;111(2):558–565.
- 7. Hoster E, Rosenwald A, Berger F, et al. Prognostic value of Ki-67 index, cytology, and growth pattern in mantle-cell lymphoma: results from randomized trials of the European Mantle Cell Lymphoma Network. J Clin Oncol. 2016;34(12):1386–1394.
- 8. Wang ML, Shah NN, Jurczak W, et al. Efficacy of brexucabtagene autoleucel (KTE-X19) in patients with relapsed/refractory mantle cell lymphoma in the ZUMA-2 trial. J Clin Oncol. 2021;39(suppl 15):7544.
- 9. Australian Institute of Health and Welfare (AIHW). Cancer data in Australia. Canberra: AIHW; 2024. Available from: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia
- 10. Cancer Australia. Non-Hodgkin lymphoma — national cancer control indicators. Surry Hills, NSW: Cancer Australia; 2023.
- 11. Chan KL, Blombery P, Westerman D, et al. Genomic landscape and clinical outcomes of mantle cell lymphoma in the era of targeted therapy: an Australian multi-centre experience. Intern Med J. 2022;52(suppl 2):S45.
- 12. National Health and Medical Research Council (NHMRC). Ethical conduct in research with Aboriginal and Torres Strait Islander Peoples and communities: guidelines for researchers and stakeholders. Canberra: NHMRC; 2018.
- 13. Services Australia. Medicare Benefits Schedule (MBS). Canberra: Australian Government. Available from: https://www.mbsonline.gov.au
- 14. Australian Government Department of Health. Pharmaceutical Benefits Scheme (PBS). Available from: https://www.pbs.gov.au