📋 Key Information Summary
- Burkitt lymphoma (BL) is the most rapidly proliferating human malignancy — tumour doubling time is approximately 24 hours.
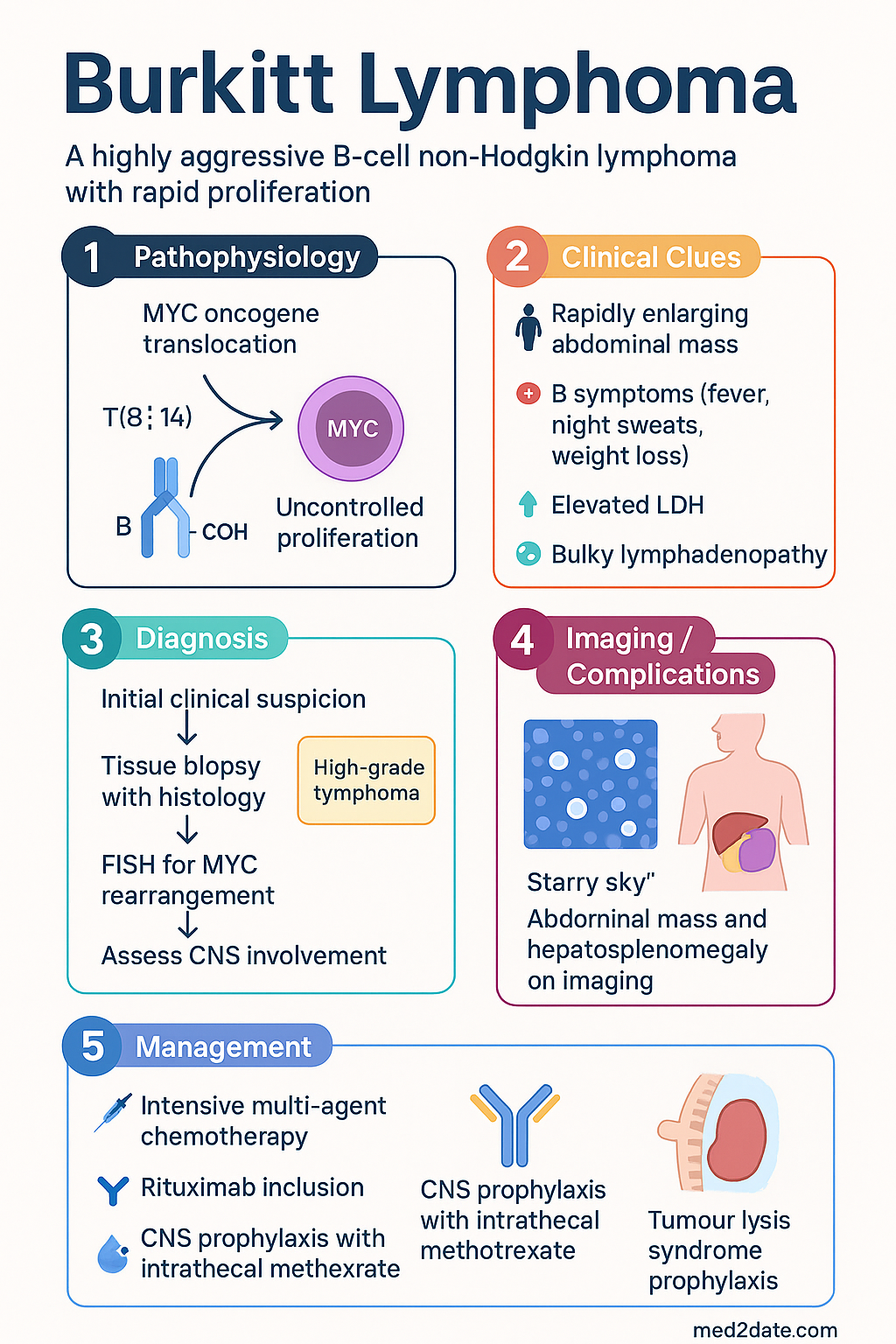
- Hallmark genetic abnormality is translocation of the MYC oncogene on chromosome 8 to the immunoglobulin heavy chain locus on chromosome 14 (t(8;14)) or, less commonly, to the κ or λ light chain loci (t(2;8) or t(8;22)).
- Epstein–Barr virus (EBV) is present in virtually all endemic BL cases, ~30% of sporadic BL cases, and ~40% of immunodeficiency-associated BL cases.
- Three clinical variants are recognised: endemic (equatorial Africa), sporadic (rest of world including Australia), and immunodeficiency-associated (HIV, post-transplant).
- In Australia, sporadic BL is the most common variant, with an annual incidence of approximately 0.2–0.3 per 100,000; paediatric cases predominate.
- Rapidly enlarging abdominal mass, B symptoms, elevated LDH, and bulky lymphadenopathy are typical clinical features at presentation.
- Diagnosis requires tissue biopsy with histology showing a "starry sky" pattern, positive CD20/CD10/BCL6 immunophenotyping, high Ki-67 (≈100%), and confirmed MYC rearrangement by FISH.
- Management centres on intensive, dose-dense multi-agent chemotherapy — CODOX-M/IVAC (Magrath regimen) or hyper-CVAD — with rituximab incorporated in current Australian protocols.
- CNS prophylaxis with intrathecal methotrexate and/or cytarabine is mandatory due to the high risk of CNS involvement (13–17% at diagnosis).
- Tumour lysis syndrome (TLS) is a medical emergency — prophylaxis with rasburicase and aggressive IV hydration must begin before or at initiation of chemotherapy.
- Prognosis is favourable with modern intensive regimens: paediatric BL achieves 85–90% overall survival; adult BL approximately 70–80% in the rituximab era.
- Aboriginal and Torres Strait Islander patients may present with more advanced disease due to access barriers — early referral to tertiary haematology is critical.
Introduction & Australian Epidemiology
Burkitt lymphoma (BL) is a highly aggressive B-cell non-Hodgkin lymphoma characterised by uncontrolled cellular proliferation driven by constitutive activation of the MYC oncogene. It represents the fastest-growing human malignancy with a tumour doubling time of approximately 24 hours, necessitating urgent diagnosis and immediate therapeutic intervention. BL accounts for 1–2% of adult non-Hodgkin lymphomas in Australia but is considerably more common in the paediatric population, representing approximately 40% of childhood non-Hodgkin lymphomas.
In Australia, the annual incidence of BL is estimated at 0.2–0.3 per 100,000 population, with a bimodal age distribution peaking in children aged 4–7 years and a second peak in young adults aged 20–34 years. The male-to-female ratio is approximately 3:1 in sporadic cases. The Cancer Council Australia and Australian Institute of Health and Welfare (AIHW) data indicate that non-Hodgkin lymphoma is the sixth most common cancer nationally, with BL constituting a small but clinically significant proportion requiring distinct management pathways.
Unlike the endemic variant found in equatorial Africa, where BL is the most common childhood malignancy and is almost universally associated with Epstein–Barr virus (EBV) and chronic malaria co-infection, the sporadic variant seen in Australia has a lower but significant EBV association (~30% of cases). Immunodeficiency-associated BL is increasingly recognised in the context of HIV infection and post-transplant immunosuppression, with particular relevance to Australia's solid organ transplantation programme.
Despite its aggressive nature, BL is one of the most curable malignancies when treated with appropriate intensive chemotherapy regimens. Five-year overall survival rates exceed 85–90% in paediatric populations and 70–80% in adults when treated with modern rituximab-containing protocols. Early recognition, prompt initiation of therapy, and rigorous tumour lysis syndrome prophylaxis are the cornerstones of successful outcomes in the Australian healthcare setting.
Pathogenesis — MYC Translocation & EBV
MYC Oncogene Translocation
The molecular hallmark of BL is translocation of the MYC proto-oncogene (chromosome 8q24) into one of the immunoglobulin (Ig) gene loci, resulting in constitutive overexpression of the MYC transcription factor. MYC is a master regulator of cell cycle progression, ribosomal biogenesis, metabolism, and apoptosis. Its deregulation drives the extraordinary proliferative rate characteristic of BL.
| Translocation | Frequency | Mechanism | Variant Association |
|---|---|---|---|
| t(8;14)(q24;q32) | ~80% | MYC → Ig heavy chain locus | All variants |
| t(2;8)(p12;q24) | ~5–15% | MYC → Ig κ light chain | Sporadic, endemic |
| t(8;22)(q24;q11) | ~5–15% | MYC → Ig λ light chain | Sporadic, endemic |
In endemic BL, the translocation breakpoint typically occurs far upstream of the MYC gene, whereas in sporadic BL it tends to lie within the gene body or its first intron. These differences likely reflect distinct mechanisms of somatic hypermutation and class switch recombination errors during B-cell development in germinal centres.
Epstein–Barr Virus
EBV plays an important but variable oncogenic role across the three BL variants:
- Endemic BL: EBV genome is present in virtually 100% of cases. Chronic malaria drives polyclonal B-cell expansion and immunosuppression, creating a large pool of EBV-infected B cells at risk of MYC translocation during Ig gene rearrangement.
- Sporadic BL: EBV is detected in approximately 20–30% of cases. The role of EBV is less clearly defined; MYC translocation may be the primary driver with EBV contributing to immune evasion.
- Immunodeficiency-associated BL: EBV is present in ~40% of cases. Impaired T-cell surveillance allows survival and expansion of EBV-infected clones bearing MYC rearrangements.
EBV-encoded proteins (particularly EBNA-1 and LMP-1 in latency type I) contribute to tumour cell survival by upregulating anti-apoptotic pathways (BCL-2, survivin) and promoting genomic instability. In endemic regions, EBV may act synergistically with MYC deregulation to achieve full malignant transformation.
Additional Molecular Features
True BL is defined by the 2017 WHO classification (updated in the 2022 ICC 5th edition) as having:
- MYC rearrangement as the sole driver abnormality (no BCL2 or BCL6 rearrangements)
- Expression of germinal centre markers: CD10+, BCL6+, MUM1−
- CD20+ (targetable with rituximab)
- Ki-67 proliferation index approaching 100%
- TP53 mutations present in ~30–40% of cases at diagnosis
- ID3 and TCF3 (E2A) mutations in ~70% of cases, enhancing B-cell receptor signalling
Cases harbouring concurrent MYC and BCL2 and/or BCL6 rearrangements are now classified as high-grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements ("double-hit" or "triple-hit" lymphoma), and are managed differently to BL.
Clinical Variants
The predominant variant in Australia. Occurs worldwide outside malaria-endemic regions. Median age at diagnosis is approximately 30 years, with a paediatric peak at 4–7 years. Male predominance (3:1).
Most common presentation: Abdominal mass (ileocaecal region, ~70%), with bowel obstruction, intussusception (especially in children), or abdominal pain with rapidly enlarging hepatosplenomegaly. Jaw involvement is uncommon (<10%) compared to the endemic variant.
Bone marrow involvement in ~20–30% at presentation; CSF involvement in ~13–17%. B symptoms (fever, night sweats, weight loss) are present in ~40% of patients.
EBV association: ~20–30%
The most common childhood cancer in equatorial Africa and Papua New Guinea. Typically affects children aged 4–7 years with a male predominance. Strongly associated with holoendemic Plasmodium falciparum malaria and EBV co-infection.
Classic presentation: Jaw and facial bone involvement (~50–60%), orbital tumours causing proptosis, and bilateral parotid gland enlargement. Abdominal disease (kidneys, ovaries, retroperitoneum) is also common. Distinct from sporadic BL in its propensity for extranodal head and neck sites.
EBV association: ~100% (EBER-positive in virtually all cases)
Arises in the context of immunosuppression: HIV/AIDS (particularly with CD4 count <200 cells/µL), post-solid organ transplant, or iatrogenic immunosuppression (e.g., methotrexate-associated lymphoproliferative disorders).
Presentation: Similar to sporadic BL with abdominal masses, lymphadenopathy, and bone marrow involvement. May present with more advanced stage disease. Unlike other HIV-associated lymphomas, BL in HIV is not classified as an AIDS-defining illness in Australia, but frequently occurs in the setting of low CD4 counts.
EBV association: ~40%
Australian context: With effective antiretroviral therapy (ART), HIV-associated BL incidence has declined but remains a significant consideration in people living with HIV. Post-transplant BL occurs in approximately 1–2% of transplant recipients on calcineurin inhibitor-based regimens.
Clinical Presentation & Diagnostic Criteria
Typical Presentations
Patients with BL typically present with rapidly enlarging masses over days to weeks. The clinical presentation varies by age and anatomical site:
| Feature | Paediatric BL | Adult BL |
|---|---|---|
| Most common site | Ileocaecal mass / abdominal | Abdominal, nodal |
| GI involvement | ~70% (intussusception common) | ~50–60% |
| B symptoms | ~30% | ~40–50% |
| Bone marrow | ~20% | ~30% |
| CNS involvement | ~13% | ~15–17% |
| LDH elevation | >90% | >90% |
| Head/neck (endemic pattern) | <10% in Australia | Rare |
WHO/ICC 5th Edition Diagnostic Criteria for BL
Definitive diagnosis of BL requires integration of morphology, immunophenotyping, cytogenetics, and molecular studies:
- Morphology: Medium-sized, monomorphic B cells with round nuclei, clumped chromatin, multiple small nucleoli, and deeply basophilic cytoplasm with lipid vacuoles on Wright–Giemsa-stained imprints. Characteristic "starry sky" pattern on low-power histology due to tingible body macrophages engulfing apoptotic tumour debris.
- Immunophenotype: CD20+, CD10+, BCL6+, BCL2−/weak, MUM1−, TdT−. Ki-67 proliferation index ≥95% (typically ~100%). Surface immunoglobulin M (sIgM) positive.
- Cytogenetics/Molecular: MYC rearrangement confirmed by fluorescence in situ hybridisation (FISH) — mandatory for diagnosis. Absence of BCL2 and BCL6 rearrangements (to exclude high-grade B-cell lymphoma with double/triple-hit).
- EBV: EBV-encoded small RNA (EBER) in situ hybridisation — positive in ~100% endemic, ~20–30% sporadic, ~40% immunodeficiency-associated BL.
Investigations
Baseline Investigations
Risk Stratification & Staging
St Ann's Staging System (Modified)
BL is staged using the Ann Arbor system, though the Murphy/St Jude staging system is used in paediatric practice:
| Stage | Definition | Treatment Intensity |
|---|---|---|
| Stage I | Single nodal/extranodal site (not abdomen) | Intensive short-course (CODOX-M) |
| Stage II | Two or more nodal sites, same side of diaphragm; or single extranodal with regional nodes | Full intensive regimen |
| Stage III | Nodes on both sides of diaphragm; or any thoracic/abdominal primary | Full intensive regimen |
| Stage IV | Bone marrow (>25%) or CNS involvement | Full intensive regimen + enhanced CNS therapy |
Prognostic Risk Factors
| Good Prognosis | Poor Prognosis |
|---|---|
| Stage I–II | Stage III–IV |
| LDH ≤2× ULN | LDH >3× ULN |
| Complete resection | Incomplete resection / bulky unresectable disease |
| No CNS involvement | CNS involvement at diagnosis |
| No bone marrow involvement | Bone marrow >25% blasts |
| Age <60 years | Age ≥60 years |
| ECOG 0–1 | ECOG ≥2 / poor performance status |
| Wild-type TP53 | TP53 mutation / deletion (17p−) |
Management — Intensive Chemotherapy & CNS Prophylaxis
Tumour Lysis Syndrome Prophylaxis (Before Chemotherapy)
TLS prophylaxis must be initiated immediately upon diagnosis and before any chemotherapy is administered:
First-Line Chemotherapy Regimens
Current Australian practice for BL chemotherapy is based on intensive, dose-dense multi-agent regimens. Rituximab is now incorporated into frontline protocols:
Treatment Protocols by Stage
| Stage | Regimen | Cycles | Duration |
|---|---|---|---|
| I–II (low risk) | CODOX-M/IVAC + Rituximab | 3 cycles (CODOX-M × 2, IVAC × 1) | ~3 months |
| III–IV (high risk) | CODOX-M/IVAC + Rituximab | 4 cycles alternating | ~4–5 months |
| CNS-positive | CODOX-M/IVAC + Rituximab + intensive IT + consider systemic high-dose cytarabine | 4+ cycles; IT therapy in every cycle | ~5–6 months |
Alternative Regimens
CNS Prophylaxis & Treatment
CNS-directed therapy includes:
- Intrathecal methotrexate: 12 mg (adults) IT, given via Ommaya reservoir or lumbar puncture. Doses in CODOX-M cycles on D1 and D3; in IVAC cycles on D5.
- Intrathecal cytarabine: 30 mg (adults) IT, given concurrently with IT methotrexate in CODOX-M cycles.
- Systemic high-dose methotrexate: 1200 mg/m² IV in CODOX-M achieves therapeutic CSF levels (with leucovorin rescue).
- Systemic high-dose cytarabine: 2000 mg/m² IV in IVAC achieves therapeutic CSF levels.
- For confirmed CNS disease: Intensify IT therapy to twice weekly until CSF clears, then weekly × 4, then per protocol. Consider high-dose systemic methotrexate (3–8 g/m²) and/or autologous SCT in fit patients with isolated CNS relapse.
Relapsed/Refractory Disease
Relapsed or refractory BL has a very poor prognosis. Management strategies in Australia include:
- Salvage chemotherapy: R-ICE (rituximab, ifosfamide, carboplatin, etoposide) or R-DHAP (rituximab, dexamethasone, high-dose cytarabine, cisplatin) — PBS General Benefit.
- Autologous stem cell transplant: Only if chemosensitive disease demonstrated after salvage. Limited role due to aggressive nature of relapsed BL.
- Allogeneic stem cell transplant: Considered in young, fit patients with chemosensitive relapse. Available at major Australian transplant centres (Westmead, Peter Mac, RCH Melbourne).
- CAR-T therapy: Tisagenlecleucel (Kymriah®) is PBS-listed for relapsed/refractory DLBCL; may be considered in BL on a case-by-case basis. Refer to specialised CAR-T centres.
- Bispecific antibodies: Glofitamab (Columvi®) — T-cell engaging bispecific antibody. TGA-approved for relapsed/refractory DLBCL. Emerging data in BL. PBS: check current listing.
Monitoring
During Treatment
- TLS monitoring: K⁺, PO₄³⁻, Ca²⁺, uric acid, creatinine, LDH every 6–8 hours for the first 72 hours of each cycle, then daily.
- FBC: Monitor full blood count twice weekly during nadir periods. Expect nadir ANC <0.5 × 10⁹/L by day 10–14 of each cycle.
- LFTs, renal function: Baseline and before each cycle. Methotrexate levels at 24 and 48 hours post-infusion (target <0.05 µmol/L at 48h).
- CSF monitoring: Repeat lumbar puncture if CNS-positive at diagnosis — confirm clearance before stopping intensive IT therapy.
- Echocardiogram: Baseline before doxorubicin-containing therapy; repeat if cumulative doxorubicin >300 mg/m² or if clinical concern.
- Fertility counselling: All patients of reproductive age should be referred for fertility preservation before commencing chemotherapy. Sperm cryopreservation and oocyte/embryo freezing available at Australian fertility centres.
Response Assessment
- Interim PET-CT: After 2 cycles (mid-treatment). Deauville score used for response assessment. Score 1–3 = complete metabolic response; 4–5 = consider biopsy to distinguish residual disease from inflammation.
- End-of-treatment PET-CT: 6–8 weeks after final cycle. Complete metabolic response (Deauville 1–3) is the goal.
- LDH trend: Serial LDH measurement is a useful surrogate marker. Normalisation of LDH is a favourable prognostic sign.
Post-Treatment Surveillance
- Clinical review every 3 months for 2 years, then every 6 months for 3 years, then annually.
- PET-CT at 3 and 12 months post-treatment (if indicated), then as clinically indicated.
- Ongoing monitoring for late effects: secondary malignancies, cardiotoxicity (doxorubicin), infertility, peripheral neuropathy (vincristine).
- Psychosocial support and survivorship care plan — referral to Cancer Council Australia survivorship programmes.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Revised 4th ed. Lyon: IARC Press; 2017.
- 2. Alaggio R, Amador C, Anagnostopoulos I, et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia. 2022;36(7):1720–1748.
- 3. Magrath I, Adde M, Shad A, et al. Adults and children with small non-cleaved-cell lymphoma have a similar excellent outcome when treated with the same chemotherapy regimen. J Clin Oncol. 1996;14(3):925–934.
- 4. Dunleavy K, Pittaluga S, Shovlin M, et al. Low-intensity therapy in adults with Burkitt's lymphoma. N Engl J Med. 2013;369(20):1915–1925.
- 5. Ribrag V, Koscielny S, Bosq J, et al. Rituximab and dose-dense chemotherapy for adults with Burkitt's lymphoma: a randomised, controlled, open-label, phase 3 trial. Lancet. 2016;387(10036):2402–2411.
- 6. Molyneux EM, Rochford R, Griffin B, et al. Burkitt's lymphoma. Lancet. 2012;379(9822):1234–1244.
- 7. Blum KA, Lozanski G, Byrd JC. Adult Burkitt leukaemia and lymphoma. Blood. 2004;104(10):3009–3020.
- 8. Roschewski M, Dunleavy K, Abramson JS, et al. Multicenter study of risk-adapted therapy with dose-adjusted EPOCH-R in adults with untreated Burkitt lymphoma. J Clin Oncol. 2020;38(26):3005–3015.
- 9. Cairo MS, Gerrard M, Sposto R, et al. Results of a randomized international study of high-risk central nervous system B non-Hodgkin lymphoma and B acute lymphoblastic leukemia in children and adolescents. Blood. 2007;109(7):2736–2743.
- 10. Australian Institute of Health and Welfare. Cancer in Aboriginal & Torres Strait Islander people of Australia. Cat. no. CAN 115. Canberra: AIHW; 2018.
- 11. Condon JR, Zhang X, Baade P, et al. Cancer survival for Aboriginal and Torres Strait Islander Australians: a national study of survival indices and predictors. Aust NZ J Public Health. 2014;38(6):547–553.
- 12. National Cancer Control Network (NCCN). Clinical Practice Guidelines in Oncology: B-Cell Lymphomas. Version 5.2024. Available at: nccn.org.
- 13. Australian Commission on Safety and Quality in Health Care. National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2017.
- 14. Muffly L, Bhatt A, Hoeg R, et al. Tumour lysis syndrome in Burkitt lymphoma: the role of rasburicase. Leuk Lymphoma. 2018;59(10):2313–2320.