📋 Key Information Summary
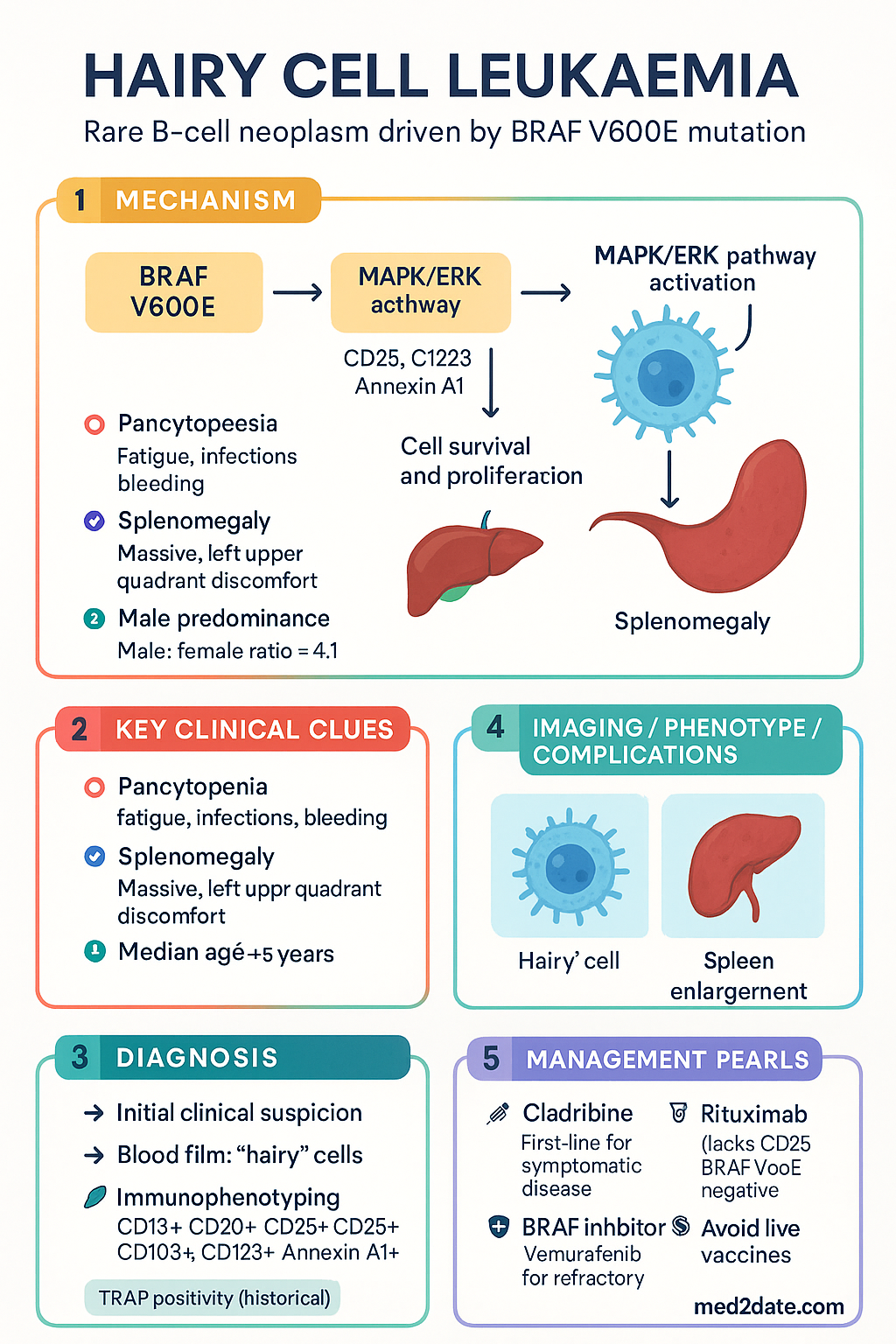
- Rare, indolent B-cell neoplasm (≈2% of lymphoid leukaemias) defined by the BRAF V600E mutation in >90% of classical cases.
- Classic presentation: pancytopenia, splenomegaly (often massive), and circulating 'hairy' lymphoid cells with cytoplasmic projections.
- Diagnosis requires immunophenotyping: CD19+, CD20+, CD22+, CD25+, CD103+, CD123+, Annexin A1+; and may show TRAP positivity.
- First-line treatment for symptomatic or cytopenic disease: purine analogue cladribine (2-CdA). Single-course achieves durable complete remission in >80%.
- Pentostatin is an alternative purine analogue; choice depends on comorbidities and local protocols.
- Anti-CD20 monoclonal antibody rituximab is used as consolidation for residual disease, or in relapsed/refractory settings.
- BRAF inhibitors (vemurafenib, dabrafenib ± trametinib) are effective in multiply relapsed/refractory BRAF V600E-mutated HCL.
- Asymptomatic patients with minimal cytopenias may be observed with regular monitoring.
- Major risk is profound, prolonged immunosuppression post-purine analogue therapy; prophylactic antimicrobials and live vaccine avoidance are essential.
- Median age at diagnosis ~55 years; male:female ratio ≈4:1. No established screening; diagnosed via blood film and bone marrow biopsy.
- ATSI considerations: address geographic barriers to specialist care, ensure culturally safe communication, and consider higher risk of infections in remote communities.
Introduction & Australian Epidemiology
Hairy cell leukaemia (HCL) is a rare, indolent B-cell lymphoproliferative neoplasm accounting for approximately 2% of all leukaemias. It is characterised by the accumulation of small B-lymphocytes with circumferential cytoplasmic projections ('hairy' cells) in the peripheral blood, bone marrow, and spleen. The disease has a distinctive molecular signature, with the BRAF V600E mutation present in the vast majority of classical cases.
In Australia, the age-standardised incidence is estimated at 0.3–0.4 per 100,000 population per year. The disease predominantly affects middle-aged to older adults, with a median age at diagnosis of approximately 55 years. There is a marked male predominance, with a male-to-female ratio of about 4:1. While rare, its high responsiveness to specific therapies makes accurate diagnosis and management crucial. The majority of patients present with symptoms related to cytopenias (fatigue, infection, bleeding) or splenomegaly.
Pathogenesis (BRAF V600E Mutation)
The discovery of the BRAF V600E mutation has revolutionised the understanding of HCL pathogenesis and provided a targeted therapeutic avenue.
The mutation promotes cell survival, proliferation, and the characteristic morphology and immunophenotype of the hairy cell. It is highly specific for classical HCL and is not found in HCL-variant (HCL-v) or most other B-cell lymphomas, making it a key diagnostic marker.
The downstream signalling results in expression of specific markers (CD25, CD123) and cytokine production contributing to the fibrotic marrow environment and pancytopenia. Understanding this pathway underpins the use of BRAF inhibitors in relapsed disease.
Clinical Features & Blood Film
Presentation is often insidious. Symptoms are primarily due to bone marrow failure and splenomegaly.
Typical Clinical Features
- Constitutional: Fatigue, weakness, weight loss, night sweats (less common than in aggressive lymphomas).
- Due to pancytopenia: Recurrent infections (neutropenia), bleeding/bruising (thrombocytopenia), pallor (anaemia).
- Splenomegaly: Present in >80% of cases, often massive and causing left upper quadrant discomfort or early satiety. Hepatomegaly is less common.
- Autoimmune complications: Vasculitis, polyarthritis, and immune-mediated haemolytic anaemia may occur.
Peripheral Blood Film Findings
The blood film is a critical first clue to diagnosis.
- Pancytopenia: Typical, though some patients may have only one or two lineages affected.
- 'Hairy' cells: Mononuclear cells with abundant cytoplasm and irregular, 'hairy' projections. They are often present in low numbers (may be <10% of circulating leucocytes).
- Monocytopenia: An almost universal and characteristic feature, helping to distinguish HCL from other low-grade lymphomas.
Diagnosis (TRAP Stain, Immunophenotyping)
Diagnosis is made by a combination of morphology, cytochemistry, immunophenotyping, and molecular testing. Bone marrow biopsy is usually required.
Key Diagnostic Investigations
Risk Stratification / Severity Scoring
HCL is generally indolent, but stratification guides treatment timing and choice.
Management (Cladribine, Rituximab)
First-Line Therapy: Purine Analogues
Treatment is indicated for symptomatic disease or significant cytopenias. Purine analogues are the standard of care.
- Pneumocystis jirovecii prophylaxis (e.g., trimethoprim/sulfamethoxazole 3 times/week) for at least 3-6 months post-therapy.
- Antiviral prophylaxis (e.g., valaciclovir) for at least 3 months.
- Avoidance of live vaccines indefinitely.
Consolidation & Relapsed/Refractory Therapy
Rituximab plays a key role in managing residual disease and relapse.
Monitoring
Response assessment and long-term follow-up are critical.
- Response Assessment: Blood counts at 3-6 months post-therapy. Bone marrow biopsy and imaging (CT for splenomegaly) are performed if blood counts do not normalise, to assess for complete remission (CR).
- Definition of CR: Absence of hairy cells in blood/bone marrow, resolution of splenomegaly, and recovery of counts (Hb >110 g/L, platelets >100 x 10⁹/L, neutrophils >1.5 x 10⁹/L) for at least 4 weeks.
- Long-term Follow-up: Clinical review and FBC every 3-6 months for the first 2 years, then annually. Monitor for late relapse (can occur >10 years post-treatment) and long-term complications (secondary malignancies, infections).
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Tiacci E, Trifonov V, Schiavoni G, et al. BRAF mutations in hairy-cell leukemia. N Engl J Med. 2011;364(24):2305-2315.
- 2. Pede V, Rombout A, Verhoef G, et al. Hairy cell leukaemia: a retrospective review of 110 cases. Eur J Haematol. 2013;91(3):259-265.
- 3. Grever MR, Abdel-Wahab O, Andritsos LA, et al. Consensus guidelines for the diagnosis and management of patients with classic hairy cell leukemia. Blood. 2017;129(5):553-560.
- 4. Robak T, Matutes E, Catovsky D, et al. Hairy cell leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015;26(Suppl 5):v100-v107.
- 5. Australian Government, Cancer Australia. Hairy cell leukaemia statistics. Available at: cancer.gov.au. [Accessed 2024].
- 6. Kreitman RJ, Arons E, Stetler-Stevenson M, et al. Response to cladribine of hairy cell leukemia with variant morphology and CD25 negativity. Leuk Lymphoma. 2019;60(7):1788-1791.
- 7. Dietrich S, Pircher A, Endris V, et al. BRAF inhibition in hairy cell leukemia with vemurafenib. Blood. 2016;127(13):1656-1659.
- 8. Pharmaceutical Benefits Scheme (PBS). Cladribine injection. Available at: pbs.gov.au. [Accessed 2024].
- 9. Therapeutic Guidelines Ltd. eTG complete [digital]. Melbourne: Therapeutic Guidelines Limited; 2024.
- 10. Australian Institute of Health and Welfare (AIHW). Cancer in Aboriginal and Torres Strait Islander people of Australia. Cat. no. CAN 110. Canberra: AIHW; 2018.
- 11. Tallman MS, Hakimian D, Rademaker AW, et al. Relapse of hairy cell leukemia after 2-chlorodeoxyadenosine: long-term follow-up of 123 patients. Cancer. 2017;123(12):2329-2337.