📋 Key Information Summary
- Haemolytic uraemic syndrome (HUS) is a thrombotic microangiopathy (TMA) defined by the triad of microangiopathic haemolytic anaemia (MAHA), thrombocytopenia, and acute kidney injury (AKI).
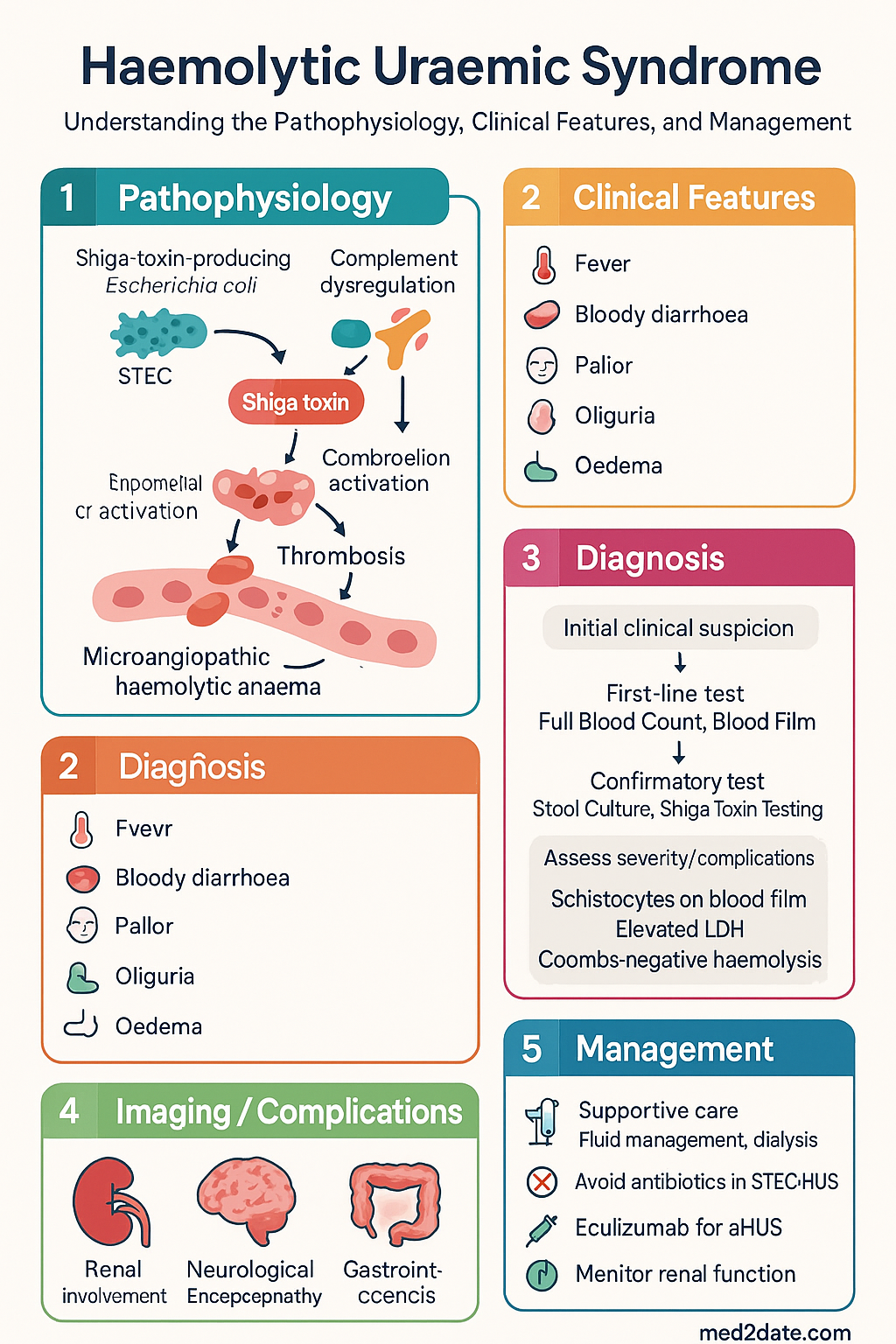
- Stx-HUS (typical HUS) accounts for ~90% of paediatric cases; triggered by Shiga toxin-producing Escherichia coli (STEC), predominantly serotype O157:H7.
- Atypical HUS (aHUS) is driven by uncontrolled complement activation due to genetic or acquired complement dysregulation; accounts for ~10% of cases but carries higher morbidity.
- In Australia, STEC infection is nationally notifiable; serotype O157 and non-O157 (O26, O111, O145) isolates are reported to state/territory health departments and OzFoodNet.
- Fever, bloody diarrhoea, pallor, oliguria, and oedema are the most common presenting features in children; adults present with more severe renal impairment.
- Peripheral blood film showing schistocytes, elevated LDH, low haptoglobin, and Coombs-negative haemolysis confirm MAHA.
- Supportive management is the cornerstone: careful fluid and electrolyte management, renal replacement therapy when indicated, and red cell / platelet transfusion as needed.
- Antibiotics are not recommended for STEC-HUS as they may increase the risk of developing HUS by promoting Shiga toxin release.
- Eculizumab (Soliris®) is the treatment of choice for confirmed or suspected complement-mediated aHUS; PBS Authority Required listing in Australia.
- Haemolytic uraemic syndrome following STEC infection is a notifiable condition under state and territory public health legislation.
- Mortality in typical HUS is ~1–5%; the majority of survivors recover renal function, but 5–15% develop chronic kidney disease.
- Differentiation between STEC-HUS and aHUS is critical because treatment strategies diverge fundamentally — targeted complement inhibition versus supportive care.
- Aboriginal and Torres Strait Islander children have higher rates of STEC-HUS, driven by environmental exposures, remoteness, and access to clean water.
Introduction & Australian Epidemiology
Haemolytic uraemic syndrome (HUS) is the most common cause of acute kidney injury in young children and is classified among the thrombotic microangiopathies (TMAs). The hallmark triad comprises microangiopathic haemolytic anaemia (MAHA), thrombocytopenia, and acute kidney injury. The syndrome is broadly divided into two categories: Shiga toxin-producing Escherichia coli HUS (Stx-HUS, also termed "typical HUS") and complement-mediated atypical HUS (aHUS). A third category encompasses HUS related to secondary causes such as Streptococcus pneumoniae infection, drugs, transplantation, and pregnancy.
In Australia, STEC-HUS is the dominant form. The Australian Paediatric Surveillance Unit (APSU) and OzFoodNet sentinel surveillance identify approximately 2–6 cases of STEC-HUS per 100,000 children under 5 years annually, with seasonal peaks in summer and autumn linked to undercooked meat, contaminated produce, and recreational water exposure. STEC O157:H7 remains the predominant serotype nationally, although non-O157 strains (particularly O26, O111, and O145) are increasingly recognised. Several large outbreaks in Australia have been traced to petting farms, contaminated salad vegetables, and community barbecues.
Atypical HUS is rare, with an estimated incidence of 2–3 per million population. Genetic studies in Australian cohorts have identified pathogenic variants in CFH, CFI, MCP/CD46, CFB, and THBD, as well as anti-factor H autoantibodies. The median age at presentation is lower than Stx-HUS but aHUS may present at any age. Approximately 50–60% of aHUS patients progress to end-stage kidney disease (ESKD) without complement inhibitor therapy.
This guideline covers the pathogenesis, clinical features, investigation, and management of both typical and atypical HUS with an emphasis on Australian diagnostic resources, PBS-listed therapies, and paediatric-focused management.
Pathogenesis — STEC O157:H7 & Shiga Toxin
Stx-HUS (Typical HUS)
The pathogenesis of STEC-HUS follows a well-characterised sequence beginning with ingestion of the organism, progressing to intestinal colonisation, toxin elaboration, and systemic endothelial injury.
Step 1 — Ingestion & Colonisation
Transmission occurs via contaminated food (undercooked beef mince, unpasteurised dairy, raw sprouts, leafy greens), contaminated water, direct animal contact (petting zoos, farm visits), and person-to-person faecal-oral spread. STEC O157:H7 colonises the terminal ileum and colon by adhering to the intestinal epithelium via attaching and effacing (A/E) lesions mediated by the locus of enterocyte effacement (LEE) pathogenicity island and the adhesin intimin.
Step 2 — Shiga Toxin Production
STEC strains produce Shiga toxin type 1 (Stx1) and/or type 2 (Stx2). Stx2 is more commonly associated with HUS development and carries a worse prognosis. The toxin is encoded on lambdoid prophages and its expression is upregulated by phage induction triggered by SOS response to DNA damage (e.g., from antibiotic exposure — fluoroquinolones and beta-lactams). This is the rationale for avoiding antibiotics in suspected STEC infection.
Shiga toxin is an AB₅ toxin. The B subunit binds to globotriaosylceramide (Gb3/CD77) receptors on endothelial cells, primarily in the glomerular microvasculature. After receptor-mediated endocytosis, the A subunit depurinates a specific adenine residue on the 28S rRNA of the eukaryotic 60S ribosomal subunit, halting protein synthesis and triggering apoptosis.
Step 3 — Endothelial Injury & Thrombotic Microangiopathy
Shiga toxin-mediated endothelial damage triggers a cascade:
- Endothelial cell swelling, apoptosis, and detachment from the basement membrane.
- Exposure of subendothelial collagen, activating platelets via von Willebrand factor (vWF) and tissue factor.
- Secretion of ultra-large vWF multimers from injured endothelium; failure of ADAMTS13-mediated cleavage (ADAMTS13 activity is typically mildly reduced, not absent — this distinguishes HUS from thrombotic thrombocytopenic purpura).
- Formation of microthrombi in arterioles and capillaries of the kidney, leading to ischaemia and AKI.
- Mechanical fragmentation of red blood cells passing through partially occluded vessels produces schistocytes (MAHA).
- Platelet consumption in microthrombi leads to thrombocytopenia without significant bleeding tendency.
- Complement activation via the alternative pathway amplifies tissue injury; C3 consumption is frequently observed.
Atypical HUS (Complement-Mediated)
In aHUS, the inciting event may be absent or non-specific (upper respiratory infection, diarrhoeal illness, pregnancy, or drug exposure). The fundamental defect is uncontrolled activation of the alternative complement pathway due to loss-of-function mutations in complement regulatory proteins (Factor H, Factor I, MCP/CD46) or gain-of-function mutations in complement effectors (Factor B, C3). Anti-factor H autoantibodies account for 5–10% of aHUS cases.
Without intact complement regulation, C3b is deposited on endothelial surfaces, promoting formation of the membrane attack complex (C5b-9) and amplifying the prothrombotic cascade. This leads to the same microangiopathic injury pattern as Stx-HUS but without the antecedent STEC infection.
| Feature | Stx-HUS (Typical) | aHUS (Atypical) |
|---|---|---|
| Trigger | STEC infection (usually O157:H7) | Complement gene mutation / anti-FH Ab / precipitant |
| Diarrhoeal prodrome | Present in >90% | Absent or non-specific (~30%) |
| Age peak | 6 months – 5 years | Any age; bimodal (children & adults 20–40 yr) |
| ADAMTS13 activity | >10% | >10% |
| Renal involvement | Usually recoverable | Often severe; 50–60% to ESKD without treatment |
| Stool STEC / Stx positive | Yes | No |
| First-line therapy | Supportive care | Eculizumab (Soliris®) |
| Plasma exchange | Not routinely recommended | Consider if eculizumab unavailable or diagnostic uncertainty |
Clinical Features & The HUS Triad
The Classical Triad
HUS is defined by the simultaneous or sequential occurrence of three core features:
Stages of Presentation — Typical STEC-HUS
Extra-Renal Manifestations
- Neurological: Seizures (10–20%), encephalopathy, stroke, cerebral oedema — most common cause of death in HUS.
- Gastrointestinal: Colonic necrosis, perforation, intussusception, pancreatitis (elevated lipase/amylase).
- Cardiac: Myocardial ischaemia, arrhythmias from electrolyte derangement (hyperkalaemia).
- Pulmonary: Pulmonary oedema from fluid overload and capillary leak.
- Haematological: Disseminated intravascular coagulation (rare); haemorrhage if severe thrombocytopenia.
Investigations
Investigations serve three purposes: (1) confirming the diagnosis of TMA / HUS, (2) identifying the aetiology (STEC vs complement-mediated vs secondary), and (3) assessing end-organ damage.
Essential First-Line Investigations
Second-Line & Specialist Investigations
Risk Stratification & Severity Scoring
Risk stratification guides the intensity of monitoring and the threshold for escalation to dialysis or complement inhibition. The following factors identify high-risk patients at presentation.
Poor Prognostic Factors in STEC-HUS
- Age <2 years (higher rates of dialysis and neurological complications).
- Leucocytosis >20 × 10⁹/L at presentation.
- Stx2-producing strain (associated with worse renal and neurological outcomes than Stx1).
- Prolonged anuria (>7 days) — strongest predictor of long-term CKD.
- Neurological involvement at any point — highest mortality risk.
- Antibiotic exposure in the prodromal diarrhoeal phase.
Management — Supportive Care (Stx-HUS)
Supportive management is the foundation of care for STEC-HUS. There is no specific antitoxin therapy with proven efficacy in large randomised trials.
Fluid & Electrolyte Management
- Early, cautious fluid resuscitation in the diarrhoeal phase (before HUS onset) may reduce severity — isotonic saline bolus 20 mL/kg if clinically dehydrated, then maintenance.
- Once HUS established, restrict fluid to insensible losses + urine output (usually 60–80% of maintenance).
- Monitor electrolytes 4–6 hourly: potassium, phosphate, calcium, bicarbonate.
- Treat hyperkalaemia urgently (calcium gluconate, insulin/dextrose, salbutamol nebuliser, sodium bicarbonate, calcium resonium). Dialysis for refractory hyperkalaemia.
- Correct metabolic acidosis with sodium bicarbonate if pH <7.2 or HCO₃⁻ <15 mmol/L.
- Monitor strict fluid balance — weigh nappies, urine output catheterisation if anuric.
Renal Replacement Therapy (Dialysis)
Indications for dialysis in paediatric HUS include:
- Anuria >24 hours with fluid overload or rising creatinine.
- Refractory hyperkalaemia (>6.5 mmol/L despite medical therapy).
- Severe metabolic acidosis (pH <7.1).
- Uraemic encephalopathy or uraemic symptoms (vomiting, pericarditis).
- Severe fluid overload with pulmonary oedema.
Peritoneal dialysis (PD) is the preferred modality in children — avoids anticoagulation in the setting of thrombocytopenia and is readily available at tertiary paediatric centres. Temporary Tenckhoff catheter insertion may be performed at the bedside. Intermittent haemodialysis (IHD) or continuous renal replacement therapy (CRRT) is used when PD is contraindicated (recent abdominal surgery, peritonitis) or in haemodynamically unstable patients.
Blood Product Support
- Packed red blood cells (pRBCs): Transfuse when Hb <60 g/L or symptomatic anaemia (pallor, tachycardia, respiratory distress). Irradiated and CMV-safe products preferred for immunocompromised patients. Avoid rapid transfusion in hypertensive patients.
- Platelets: Platelet transfusion is generally avoided unless there is active, life-threatening bleeding or prior to an essential invasive procedure. Transfused platelets may worsen microthrombi formation.
- Fresh frozen plasma: Not indicated for STEC-HUS in isolation. May be considered in the rare scenario of concurrent DIC with coagulopathy.
Antihypertensive Therapy
Hypertension is common in HUS (30–60% of cases) and may result from fluid overload and/or activation of the renin-angiotensin system.
- Nifedipine: 0.25–0.5 mg/kg PO (maximum 10 mg) for acute hypertension. PBS General Benefit.
- Enalaprilat / Enalapril: IV enalaprilat 5–10 μg/kg (max 1.25 mg) for hypertensive emergency. Oral enalapril for ongoing management. PBS General Benefit.
- Avoid aggressive reduction — target <95th percentile for age/height/sex (or <130/80 if >13 years).
Anti-Diarrhoeal & Anti-Motility Agents
- Loperamide and other anti-motility agents are contraindicated in suspected STEC infection — they prolong toxin exposure and may increase the risk of HUS.
Management — Eculizumab for Atypical HUS
Eculizumab (Soliris®)
Eculizumab is a humanised monoclonal antibody that binds complement protein C5, preventing cleavage to C5a and C5b and blocking formation of the membrane attack complex. It is the first-line treatment for complement-mediated aHUS and has transformed outcomes — reducing progression to ESKD from ~50–60% to <20%.
Meningococcal Vaccination Protocol (Pre-Eculizumab)
| Vaccine | Schedule | Timing |
|---|---|---|
| MenACWY (Nimenrix®) | Single dose (≥12 months of age); two doses 8 weeks apart if <12 months | ≥2 weeks before first eculizumab dose |
| MenB (Bexsero®) | Two doses, ≥1 month apart (≥2 months of age) | Begin at least 2 weeks before first eculizumab dose |
| Booster MenACWY | Every 3–5 years while on eculizumab | Per ATAGI/RACGP schedule |
| Emergency prophylaxis | Ciprofloxacin 500 mg PO stat (adults) or rifampicin if ciprofloxacin contraindicated | Carry at all times; take immediately if fever occurs |
Plasma Exchange (PLEX) / Plasma Infusion
Plasma exchange is the historical mainstay of TTP management and has limited evidence in HUS. Its role in aHUS has been superseded by eculizumab. Consider PLEX when:
- Diagnostic uncertainty between TTP and aHUS (ADAMTS13 result pending).
- Eculizumab is not immediately available.
- Anti-Factor H autoantibody-mediated aHUS (PLEX to remove antibodies + immunosuppression).
- Do not delay eculizumab initiation for PLEX in suspected aHUS.
Immunosuppression for Anti-Factor H Autoantibody-Mediated aHUS
- Mycophenolate mofetil (CellCept®): 600 mg/m²/day PO in divided doses (adults: 1 g BD). PBS Authority Required.
- Rituximab: 375 mg/m² IV weekly × 4 doses for refractory anti-FH antibodies. PBS Restricted Benefit.
- Combination with PLEX and eculizumab in severe presentations.
Special Populations
Aboriginal and Torres Strait Islander Health
Monitoring & Follow-Up
Acute Phase Monitoring (Inpatient)
| Parameter | Frequency | Target / Action |
|---|---|---|
| Full blood count + blood film | 12–24 hourly | Platelet recovery = resolving TMA. Persistent schistocytes = ongoing disease. |
| EUC, phosphate, calcium, urate | 6–12 hourly | Trend creatinine; manage electrolyte derangements. |
| LDH, haptoglobin | 24–48 hourly | Declining LDH / rising haptoglobin = resolving haemolysis. |
| Blood pressure | 4–6 hourly (minimum) | Target <95th centile for age. Antihypertensive therapy if persistent. |
| Strict fluid balance + weight | Continuous | Daily weight; urine output >0.5 mL/kg/h indicates renal recovery. |
| Neurological observations | 2–4 hourly | GCS, pupil reactivity, seizure monitoring. Urgent CT/MRI if deterioration. |
| Stool culture (clearance) | Two consecutive negatives before discharge from isolation | Contact precautions until two negative stool cultures. |
Eculizumab Monitoring (aHUS)
- CH50 / haemolytic complement assay: Monitor before each infusion — target <10% of normal confirms adequate C5 blockade.
- Clinical response: Expect platelet count normalisation within 1–2 weeks and creatinine improvement within 2–4 weeks of eculizumab initiation.
- Infection surveillance: Maintain high index of suspicion for meningococcal disease (fever, rash, myalgia) — instruct patients to present immediately if fever develops.
- Pregnancy planning: Discuss contraception and pregnancy planning with women of childbearing age on eculizumab.
Long-Term Follow-Up (All HUS Survivors)
- Annual renal function tests (eGFR, urine albumin-creatinine ratio) for ≥5 years (ideally lifelong).
- Annual blood pressure measurement — hypertension may develop years after acute episode.
- Urinalysis for proteinuria and haematuria.
- Refer to nephrology if eGFR declining, proteinuria >30 mg/mmol, or new hypertension.
- Educate families on food safety, hand hygiene, and avoiding high-risk exposures (raw/undercooked meat, unpasteurised dairy).
- Consider genetic counselling for aHUS patients and first-degree relatives.
⚡ Quick Reference — Clinical Decision Summary
📚 References
- 1. Karpman D, Loos S, Tati R, Arvidsson I. Haemolytic uraemic syndrome. Journal of Internal Medicine. 2017;281(2):123–148. doi:10.1111/joim.12546
- 2. Walsh PR, Johnson S. Treatment and management of children with haemolytic uraemic syndrome. Archives of Disease in Childhood. 2018;103(3):285–291. doi:10.1136/archdischild-2016-311354
- 3. Nester CM, Barbour T, de Cordoba SR, et al. Atypical aHUS: state of the art. Molecular Immunology. 2015;67(1):31–42. doi:10.1016/j.molimm.2015.03.246
- 4. Wijnsma KL, Duineveld C, Wetzels JFM, van de Kar NCAJ. Eculizumab in atypical hemolytic uremic syndrome: strategies toward restrictive use. Pediatric Nephrology. 2019;34(10):1761–1770. doi:10.1007/s00467-018-4092-2
- 5. Shane AL, Mody RK, Crump JA, et al. 2017 Infectious Diseases Society of America clinical practice guidelines for the diagnosis and management of infectious diarrhea. Clinical Infectious Diseases. 2017;65(12):e45–e80. doi:10.1093/cid/cix669
- 6. Scheiring J, Andreoli SP, Zimmerhackl LB. Treatment and outcome of Shiga-toxin-associated hemolytic uremic syndrome (HUS). Pediatric Nephrology. 2008;23(10):1749–1760. doi:10.1007/s00467-008-0935-6
- 7. Australian Government Department of Health. OzFoodNet — enhancing foodborne disease surveillance across Australia. Communicable Diseases Intelligence. Annual reports 2018–2023. Available at: www.health.gov.au
- 8. Loirat C, Frémeaux-Bacchi V. Atypical hemolytic uremic syndrome. Orphanet Journal of Rare Diseases. 2011;6:60. doi:10.1186/1750-1172-6-60
- 9. Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook. Australian Government Department of Health, Canberra. 2022. Available at: immunisationhandbook.health.gov.au
- 10. Ray PE, Xu L, Rakusan TA, Liu XH. A 20-year history of hemolytic uremic syndrome: an update on complement activation and future therapies. Pediatric Nephrology. 2024;39(1):23–42. doi:10.1007/s00467-023-06042-6
- 11. The Royal Australasian College of Physicians (RACP). Guideline for the management of haemolytic uraemic syndrome in children. Paediatrics & Child Health Division. Sydney; 2019.
- 12. Rizzari G, Giannattasio A, Tafuri S, et al. Antibiotic use and risk of hemolytic uremic syndrome. Pediatric Nephrology. 2020;35(10):1881–1891. doi:10.1007/s00467-020-04546-y
- 13. Services Australia. Pharmaceutical Benefits Scheme — Eculizumab (Soliris®). Available at: pbs.gov.au. Accessed 2024.