📋 Key Information Summary
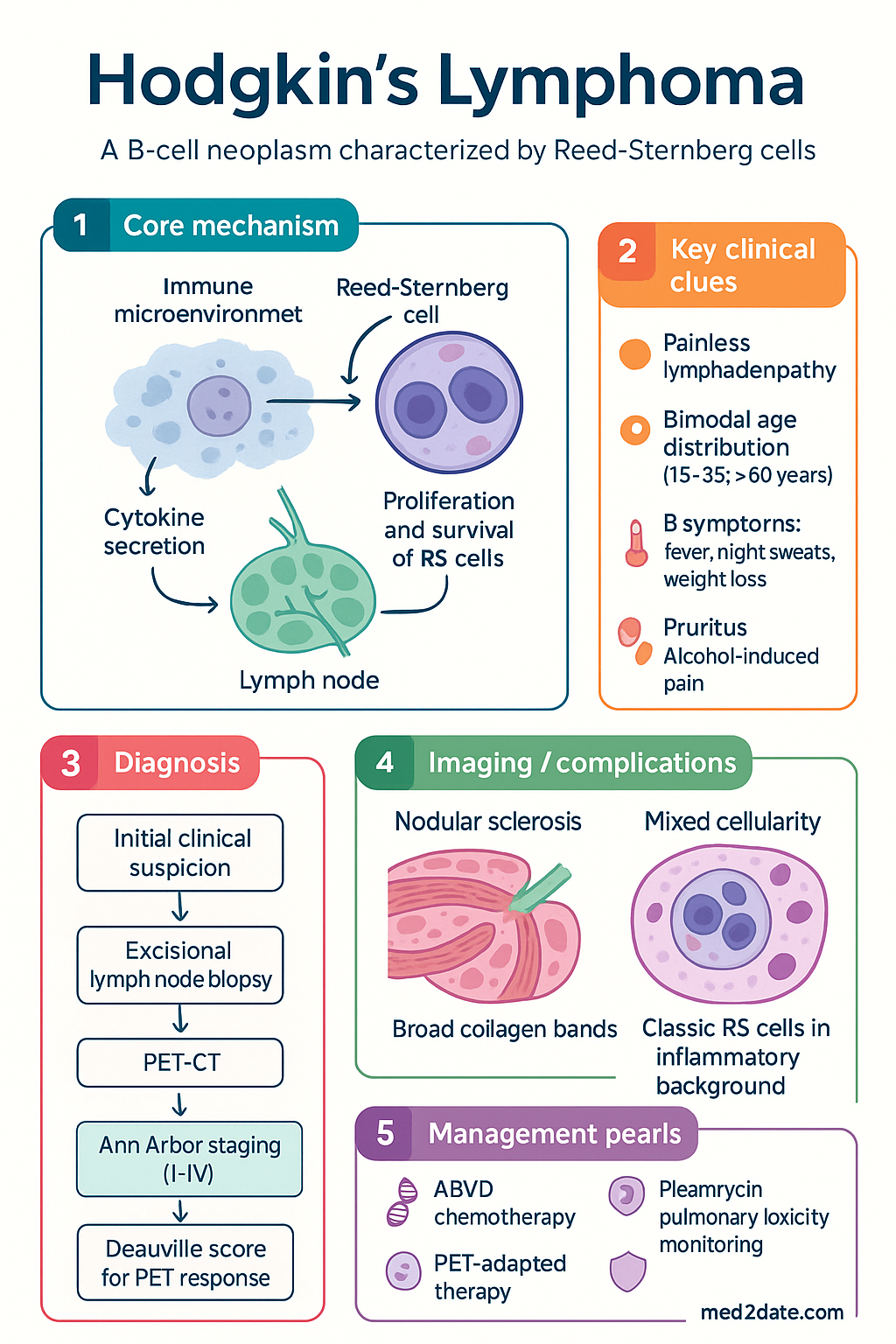
- Hodgkin lymphoma (HL) is a B-cell neoplasm characterised by the presence of Reed-Sternberg cells within an inflammatory microenvironment; accounts for approximately 10% of all lymphomas in Australia.
- Bimodal age distribution with peaks at 15–35 years and >60 years; median age at diagnosis in Australia is approximately 35 years.
- Two major histological subtypes: nodular sclerosis (most common, ~70%) and mixed cellularity (~25%); lymphocyte-rich and lymphocyte-depleted are rare.
- Ann Arbor staging (modified Lugano classification) determines treatment intensity: early-stage favourable (I–II), early-stage unfavourable (I–II with risk factors), and advanced-stage (III–IV).
- Essential investigations: excisional lymph node biopsy, contrast-enhanced CT, PET-CT (with Deauville scoring), bloods (FBC, ESR, LDV, albumin, LFTs), and echocardiography if anthracycline-based therapy planned.
- First-line chemotherapy: ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) remains the standard of care in Australia; escBEACOPP reserved for high-risk advanced disease.
- Early-stage favourable HL: 2 cycles ABVD + 20 Gy involved-site radiotherapy (ISRT) OR 3–4 cycles ABVD alone (PET-guided de-escalation).
- Advanced-stage HL: 6 cycles ABVD; PET-adapted strategy (omit bleomycin if PET-negative after 2 cycles) to reduce pulmonary toxicity.
- Bleomycin pulmonary toxicity (BPT) is the most clinically significant non-haematological ABVD adverse effect; baseline and serial pulmonary function tests (DLCO) are essential.
- Salvage chemotherapy for relapsed/refractory disease: ICE (ifosfamide, carboplatin, etoposide), DHAP, or GDP, followed by autologous stem-cell transplant (ASCT) in chemosensitive disease.
- Brentuximab vedotin (anti-CD30 antibody-drug conjugate) is PBS Authority Required for relapsed/refractory classical HL post-ASCT or post≥2 prior therapies.
- Checkpoint inhibitors (nivolumab, pembrolizumab) are TGA-approved for relapsed/refractory classical HL after ASCT and brentuximab vedotin failure.
- Five-year overall survival exceeds 85% for all stages in Australia; long-term survivors require surveillance for secondary malignancies, cardiovascular disease, and thyroid dysfunction.
- Aboriginal and Torres Strait Islander peoples may present with more advanced disease and have lower survival rates; culturally safe pathways and remote-area telehaematology are essential.
Introduction & Australian Epidemiology
Hodgkin lymphoma (HL) is a unique B-cell malignancy defined by the presence of Reed-Sternberg cells within a characteristic reactive inflammatory microenvironment. Despite its relative rarity—accounting for approximately 10–12% of all lymphomas—HL is one of the most curable haematological malignancies, with five-year overall survival exceeding 85% across all stages in high-income settings including Australia.
In Australia, approximately 700–800 new cases are diagnosed annually (age-standardised incidence ~4.5 per 100,000), with a slight male predominance (M:F ratio 1.3:1). The disease exhibits a distinctive bimodal age distribution with a first peak in adolescents and young adults (15–35 years) and a second, smaller peak in adults over 60 years. The median age at diagnosis in Australia is approximately 35 years, making HL one of the most common cancers in young adults aged 20–34 years.
Established risk factors include immunosuppression (HIV/AIDS, post-transplant), Epstein-Barr virus (EBV) infection (detected in ~40% of classical HL cases in Western populations, higher in mixed cellularity subtype), family history (first-degree relative risk increased 3–9 fold), and prior infectious mononucleosis.
The management of HL in Australia is guided by evidence-based protocols developed through international collaboration (including ANZLG trials) and adapted through Therapeutic Guidelines (eTG) and multidisciplinary team (MDT) consensus at designated cancer centres. PET-CT response-adapted therapy has become central to contemporary treatment algorithms, enabling de-escalation of therapy in good responders and intensification for those with suboptimal response.
Pathology — Reed-Sternberg Cells & Histological Subtypes
The pathological hallmark of Hodgkin lymphoma is the Reed-Sternberg (RS) cell: a large, binucleated or bilobed malignant cell with prominent eosinophilic nucleoli and abundant cytoplasm, giving an "owl-eye" appearance on histology. RS cells are clonally derived from germinal-centre or post-germinal-centre B-cells that have lost most of their B-cell identity gene-expression programme. They typically constitute only 1–5% of the tumour mass, with the remainder comprising a reactive infiltrate of T-lymphocytes, eosinophils, macrophages, neutrophils, plasma cells, and fibroblasts.
| Histological Subtype | Frequency | Key Histological Features | EBV Association |
|---|---|---|---|
| Nodular sclerosis (NS) | ~70% | Broad collagen bands dividing lymph node into nodules; lacunar cells (RS variant with artefactual retraction); prominent fibrosis | ~30–40% |
| Mixed cellularity (MC) | ~20–25% | Classic RS cells in a diffuse inflammatory background; eosinophils, plasma cells, histiocytes; no broad fibrosis | ~70–75% |
| Lymphocyte-rich (LR) | ~5% | Small lymphocyte-predominant background; rare classic RS cells; nodular or diffuse pattern | ~40% |
| Lymphocyte-depleted (LD) | <1–2% | Numerous RS cells; sparse lymphocytes; diffuse fibrosis or reticular pattern; aggressive clinical course | Variable |
Nodular lymphocyte-predominant HL (NLPHL) is now classified separately by the WHO (5th edition, 2022). It comprises ~5% of cases, is characterised by CD20⁺ "popcorn" (LP) cells within nodular backgrounds, and generally has an indolent course with different management paradigms (early-stage: radiotherapy alone; advanced-stage: R-CHOP-like regimens).
Clinical Features & Ann Arbor Staging
Clinical Presentation
The most common presentation is painless, progressive lymphadenopathy — typically cervical (60–70%) or supraclavicular. Mediastinal involvement is present in ~60–80% of nodular sclerosis cases and may cause cough, dyspnoea, or superior vena cava obstruction. Systemic "B" symptoms occur in approximately 30–40% of patients at diagnosis:
- Unexplained fever >38°C (Pel-Ebstein fever: cyclical fevers over 1–2 weeks)
- Drenching night sweats
- Unexplained weight loss >10% body weight over 6 months
Other features include generalised pruritus (may be severe), alcohol-induced pain at disease sites (pathognomonic but rare), and fatigue. Extranodal involvement at presentation is uncommon in classical HL (bone marrow ~5%, liver ~3–5%) but occurs more frequently in advanced or relapsed disease.
Ann Arbor Staging (Modified Lugano Classification, 2014)
Risk Stratification: Early-Stage Favourable vs Unfavourable
| Risk Category | Criteria (EORTC/GHSG) | Typical Approach |
|---|---|---|
| Early favourable (I–II) | No bulk (<10 cm), no B symptoms, no extranodal sites, ESR <50 (without B symptoms) or <30 (with B symptoms), ≤3 nodal sites, non-mediastinal | 2–4 cycles ABVD + 20 Gy ISRT (or PET-guided chemo-only) |
| Early unfavourable (I–II) | Bulk ≥10 cm, mediastinal bulk (MTR >0.33), B symptoms, ESR ≥50, ≥4 nodal sites, extranodal extension | 4–6 cycles ABVD + 30 Gy ISRT |
| Advanced (III–IV) | Stage III or IV; International Prognostic Score (IPS) for advanced stage | 6 cycles ABVD (PET-adapted) or escBEACOPP for high-risk |
International Prognostic Score (IPS) — Advanced Stage
One point each: albumin <40 g/L, Hb <105 g/L, male sex, stage IV disease, age ≥45 years, WCC ≥15 × 10⁹/L, lymphocytes <0.6 × 10⁹/L or <8% of WCC. Score ≥4 indicates high-risk advanced disease where escBEACOPP may be considered.
Investigations
Essential Baseline Investigations
Deauville 5-Point Scale (Interim PET Response Assessment)
| Score | FDG Uptake | Interpretation |
|---|---|---|
| 1 | No residual uptake above background | Complete metabolic response (CMR) |
| 2 | Uptake ≤ mediastinum | CMR |
| 3 | Uptake > mediastinum but ≤ liver | Likely CMR — PET-negative for treatment purposes |
| 4 | Uptake moderately > liver | PET-positive — consider treatment intensification |
| 5 | Uptake markedly > liver or new lesions | PET-positive — significant residual disease |
Management — Chemotherapy, Radiotherapy & Salvage
First-Line Chemotherapy Regimens
Treatment by Stage — PET-Adapted Strategy
- 2 cycles ABVD → iPET at cycle 2
- PET-negative (Deauville 1–3): 2 additional cycles ABVD + 20 Gy ISRT OR 2 additional cycles AVD (omitting radiotherapy — RATHL-based de-escalation)
- PET-positive (Deauville 4–5): Escalate to escBEACOPP × 4 + 30 Gy ISRT
- 4 cycles ABVD → iPET at cycle 4
- PET-negative: 2 additional cycles ABVD/AVD + 30 Gy ISRT
- PET-positive: Escalate to escBEACOPP × 2–4 + 30 Gy ISRT
- IPS <4: 6 cycles ABVD with PET-adapted bleomycin omission (iPET after cycle 2; if negative, AVD for cycles 3–6)
- IPS ≥4 or very bulky disease: Consider escBEACOPP × 6 (with PET-adapted de-escalation to ABVD if PET-negative after 2–4 cycles)
- Residual disease at end of treatment (PET-positive): Biopsy confirmation → salvage therapy
- ISRT (20–30 Gy) to residual PET-positive sites or initial bulky sites after chemotherapy
Involved-Site Radiotherapy (ISRT)
ISRT has replaced extended-field radiotherapy as the standard. Doses: 20 Gy (consolidation after complete response) to 30 Gy (residual disease). Modern techniques (3D-CRT, IMRT) minimise exposure to organs at risk (lungs, heart, breast, thyroid). All radiotherapy should be planned at designated radiation oncology centres with lymphoma experience. Cardiovascular and secondary malignancy risk must be discussed, particularly in young women (breast cancer screening commencing 8–10 years post-RT).
Salvage Therapy for Relapsed/Refractory Disease
Autologous Stem-Cell Transplant (ASCT)
ASCT is the standard-of-care consolidation for chemosensitive relapsed/refractory HL. Eligibility criteria: age generally <70 years, adequate organ function, chemosensitive disease on salvage chemotherapy (at least partial response). Conditioning regimens: BEAM (carmustine, etoposide, cytarabine, melphalan) is standard in Australia. All ASCT procedures are performed at designated transplant centres (e.g., Royal Adelaide Hospital, Peter MacCallum Cancer Centre, Westmead Hospital).
Monitoring During & After Treatment
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
- Engage Aboriginal Health Workers and Liaison Officers at all stages of the cancer pathway.
- Utilise telehaematology consultations to reduce travel burden for remote patients.
- Refer to culturally safe support services (e.g., Cancer Council, Leukaemia Foundation Indigenous support programmes).
- Ensure Yarning-based communication for treatment discussions; allow adequate time for family consultation.
- Partner with ACCHS for long-term follow-up and secondary prevention.
📚 References
- 1. Ansell SM. Hodgkin lymphoma: diagnosis and treatment. Mayo Clin Proc. 2015;90(11):1574–1583. doi:10.1016/j.mayocp.2015.07.005
- 2. Johnson P, Federico M, Kirkwood A, et al. Adapted treatment guided by interim PET-CT scan in advanced Hodgkin's lymphoma. N Engl J Med. 2016;374(25):2419–2429. doi:10.1056/NEJMoa1510093
- 3. Barrington SF, Kirkwood AA, Franceschetto A, et al. PET-CT for staging and early response: results from the Response-Adapted Therapy in Advanced Hodgkin Lymphoma (RATHL) study. Lancet Haematol. 2016;3(4):e167–e178. doi:10.1016/S2352-3026(16)00003-X
- 4. Connors JM, Jurczak W, Straus DJ, et al. Brentuximab vedotin with chemotherapy for stage III or IV Hodgkin's lymphoma. N Engl J Med. 2018;378(4):331–344. doi:10.1056/NEJMoa1708984
- 5. Ansell SM, Lesokhin AM, Borrello I, et al. PD-1 blockade with nivolumab in relapsed or refractory Hodgkin's lymphoma. N Engl J Med. 2015;372(4):311–319. doi:10.1056/NEJMoa1411087
- 6. Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014;32(27):3059–3067. doi:10.1200/JCO.2013.54.8802
- 7. Eichenauer DA, Aleman BMP, André M, et al. Hodgkin lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(Suppl 4):iv19–iv29. doi:10.1093/annonc/mdy080
- 8. Australian Institute of Health and Welfare (AIHW). Cancer in Australia 2021. Cancer Series No. 133. Canberra: AIHW; 2021.
- 9. Australian Government Department of Health. Pharmaceutical Benefits Schedule — Brentuximab vedotin (Adcetris) PBS listing. Available at: pbs.gov.au. Accessed 2024.
- 10. Cancer Australia. National Cancer Control Indicators: Hodgkin lymphoma survival. Available at: cancer-australia.gov.au. Accessed 2024.
- 11. Vassilakopoulos TP, Angelopoulou MK. Advanced and relapsed/refractory Hodgkin lymphoma: what has been achieved during the last two decades. Ther Adv Hematol. 2023;14:20406207221146826. doi:10.1177/20406207221146826
- 12. Cancer Australia. National Aboriginal and Torres Strait Islander Cancer Framework. Sydney: Cancer Australia; 2015.