📋 Key Information Summary
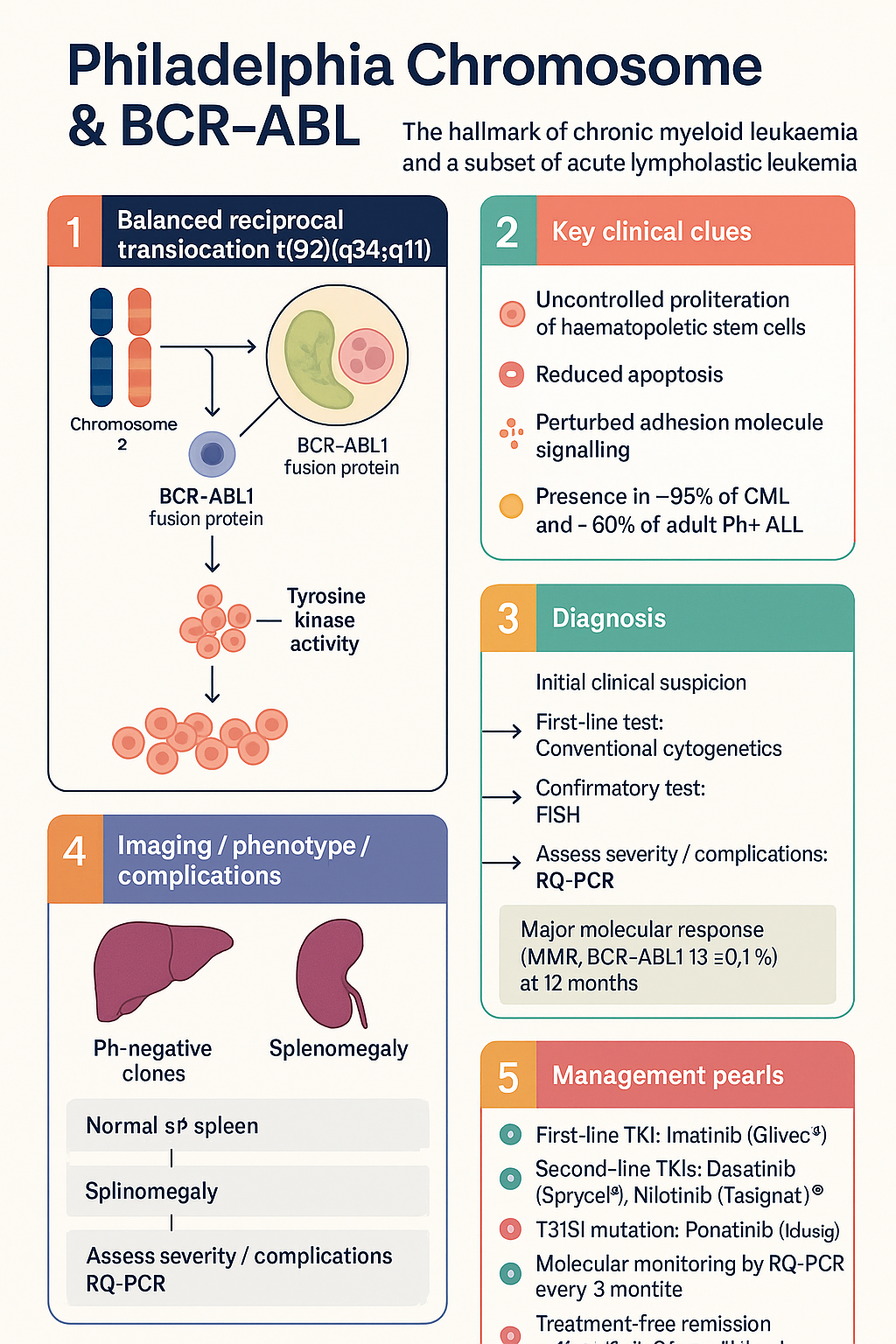
- The Philadelphia chromosome results from the balanced reciprocal translocation t(9;22)(q34;q11), creating the BCR-ABL1 fusion oncogene on the derivative chromosome 22 — the hallmark of chronic myeloid leukaemia (CML) and present in approximately 20–30% of adult and 2–5% of paediatric acute lymphoblastic leukaemia (ALL).
- The BCR-ABL1 fusion protein is a constitutively active tyrosine kinase that drives uncontrolled proliferation, reduces apoptosis, and perturbs adhesion molecule signalling in haematopoietic stem cells.
- Fusion transcript size determines disease biology: p210 BCR-ABL (e13a2 or e14a2) is typical of CML; p190 (e1a2) predominates in Ph+ ALL; p230 (e19a2) is associated with chronic neutrophilic leukaemia.
- Detection requires complementary methods: conventional cytogenetics (karyotyping) detects the translocation; fluorescence in situ hybridisation (FISH) confirms BCR-ABL1 rearrangement; real-time quantitative PCR (RQ-PCR) is the gold standard for monitoring molecular response and minimal residual disease.
- Tyrosine kinase inhibitors (TKIs) targeting the ABL1 kinase domain have transformed CML from a fatal disease to one with near-normal life expectancy — imatinib (Glivec®) is PBS-listed as the first-line agent.
- Second-generation TKIs — dasatinib (Sprycel®), nilotinib (Tasigna®) — are PBS-authority options for imatinib-resistant or intolerant CML; ponatinib (Iclusig®) is available for T315I-mutated disease.
- In Ph+ ALL, TKI therapy (dasatinib preferred) combined with intensive chemotherapy or corticosteroid-only regimens significantly improves complete remission rates and overall survival.
- Molecular monitoring by RQ-PCR every 3 months is mandatory in CML; achievement of major molecular response (MMR, BCR-ABL1 IS ≤0.1%) at 12 months is associated with excellent long-term outcomes.
- Resistance mechanisms include BCR-ABL1 kinase domain mutations (T315I the most refractory), BCR-ABL1 amplification, and clonal evolution; mutation analysis is essential when treatment milestones are not met.
- Treatment-free remission (TFR) is achievable in ~40–60% of patients with sustained deep molecular response (DMR, MR4 or better for ≥2 years) — TKI cessation must occur within a structured molecular monitoring programme.
- Aboriginal and Torres Strait Islander peoples may experience diagnostic delay and reduced access to molecular monitoring; engagement with local haematology services and culturally safe care pathways is essential.
- All TKI therapy must be managed by or in consultation with a haematologist; molecular response milestones are defined by the European LeukemiaNet (ELN) 2020 recommendations.
Introduction & Australian Epidemiology
The Philadelphia (Ph) chromosome — first described by Nowell and Hungerford in 1960 — is the product of a balanced reciprocal translocation between chromosomes 9 and 22, designated t(9;22)(q34;q11). This rearrangement fuses the ABL1 proto-oncogene (from 9q34) with the BCR gene (from 22q11), generating the BCR-ABL1 fusion oncogene on the derivative chromosome 22. The resulting fusion protein is a constitutively active tyrosine kinase that drives uncontrolled haematopoietic cell proliferation and is the central molecular lesion in chronic myeloid leukaemia (CML) and a proportion of acute lymphoblastic leukaemia (ALL).
The discovery of the Ph chromosome as the first consistent chromosomal abnormality in human cancer, and the subsequent development of targeted tyrosine kinase inhibitors (TKIs), represents one of the greatest successes of molecular oncology. Imatinib mesylate, introduced in clinical trials in the late 1990s, transformed CML from a disease with a median survival of 3–5 years to one in which most patients can expect a near-normal lifespan.
| Parameter | Value |
|---|---|
| Australian CML incidence | ~350–400 new cases per year (age-standardised rate ~1.6 per 100,000) |
| Median age at CML diagnosis | ~55–60 years; bimodal with a second peak in the 70s |
| Ph+ ALL proportion | ~20–30% of adult ALL; 2–5% of paediatric ALL |
| 5-year overall survival (CML, chronic phase, TKI era) | >90% in Australia |
| Aboriginal & Torres Strait Islander representation | Limited data; AIHW reports suggest later presentation and lower survival for haematological malignancies |
Understanding the molecular biology of the Ph chromosome and BCR-ABL1 is fundamental to rational use of TKIs, interpretation of molecular monitoring, and management of resistance. This guideline provides a comprehensive overview of the translocation, the molecular target, detection methodologies, and clinical significance with emphasis on the Australian therapeutic landscape.
Translocation & Molecular Biology
The t(9;22)(q34;q11) Rearrangement
The Philadelphia chromosome arises from a balanced reciprocal translocation between the long arms of chromosomes 9 and 22. During this rearrangement, the ABL1 gene (Abelson murine leukaemia viral oncogene homolog 1) is excised from its normal position at 9q34 and translocated to the breakpoint cluster region (BCR) gene at 22q11. The reciprocal translocation places a portion of BCR on the derivative chromosome 9, though the pathogenic fusion resides on the derivative chromosome 22 (the Ph chromosome).
BCR Gene Structure & Breakpoint Regions
The BCR gene spans approximately 135 kb and contains 23 exons. The breakpoint in BCR occurs within the major breakpoint cluster region (M-bcr), a 5.8 kb area spanning exons 12–16. Three principal breakpoint zones are recognised:
- M-bcr (major): Breakpoint between exons 13 and 14 (b2) or 14 and 15 (b3) — produces e13a2 (b2a2) or e14a2 (b3a2) transcripts encoding the p210 fusion protein. Found in ~95% of CML and ~60% of adult Ph+ ALL.
- m-bcr (minor): Breakpoint between exons 1 and 2 (e1) — produces e1a2 transcript encoding the p190 fusion protein. Predominant in ~60–80% of Ph+ ALL and a rare variant of CML.
- μ-bcr (micro): Breakpoint between exons 19 and 20 (e19) — produces e19a2 transcript encoding the p230 fusion protein. Associated with chronic neutrophilic leukaemia.
ABL1 Gene Structure
The ABL1 gene on chromosome 9 spans approximately 230 kb and contains 11 exons. The breakpoint in ABL1 is variable, occurring anywhere upstream of exon 2 (a2). All resulting BCR-ABL1 fusion transcripts retain exons 2–11 of ABL1, which encode the tyrosine kinase domain. The breakpoint variation in ABL1 does not significantly alter the fusion protein function.
Clonal Evolution & Additional Cytogenetic Abnormalities
CML in chronic phase typically shows the sole Ph chromosome abnormality. Disease progression is accompanied by clonal evolution — acquisition of additional cytogenetic abnormalities including trisomy 8, isochromosome 17q, double Ph chromosome, and trisomy 19. These secondary abnormalities correlate with accelerated phase and blast crisis, and may herald TKI resistance.
BCR-ABL Tyrosine Kinase Activity
Constitutive Kinase Activation
The BCR-ABL1 fusion protein retains the SH1 (kinase), SH2, and SH3 domains of ABL1, but the N-terminal BCR sequences replace the auto-inhibitory cap of native ABL1. The BCR coiled-coil oligomerisation domain promotes tetramerisation of BCR-ABL1, leading to trans-autophosphorylation and constitutive activation of the kinase domain. This results in ligand-independent phosphorylation of downstream substrates.
Downstream Signalling Pathways
Constitutively active BCR-ABL1 activates multiple oncogenic signalling cascades simultaneously:
- RAS/MAPK pathway: Drives cellular proliferation via GRB2-SOS-RAS-RAF-MEK-ERK signalling.
- PI3K/AKT/mTOR pathway: Promotes cell survival and inhibits apoptosis via phosphorylation of BAD, caspase-9, and FOXO transcription factors.
- JAK/STAT pathway: STAT5 phosphorylation is a major mediator of BCR-ABL1 transforming activity — drives expression of anti-apoptotic genes (BCL-XL) and cell cycle regulators.
- MYC activation: Transcriptional upregulation of MYC drives proliferation and stem cell self-renewal.
- CrkL phosphorylation: CrkL is a direct substrate of BCR-ABL1 and a surrogate marker of kinase activity; used in ex vivo drug sensitivity assays.
Impact on Haematopoietic Stem Cells
BCR-ABL1 confers several functional changes to the leukaemic stem cell:
- Reduced adhesion: Downregulation of integrins and cadherins disrupts normal stem cell–stroma interactions, releasing progenitors into the circulation.
- Increased proliferation: Shortened cell cycle duration in the progenitor compartment.
- Resistance to apoptosis: BCL-XL upregulation and p53 inactivation protect against programmed cell death.
- Genomic instability: Impaired DNA repair via altered DNA-PKcs function and reactive oxygen species generation promotes acquisition of secondary mutations.
The ABL1 Kinase Domain — TKI Binding
The ATP-binding pocket of the ABL1 kinase domain is the pharmacological target of all approved TKIs. The kinase domain exists in two conformations:
- Active (DFG-in) conformation: The activation loop adopts an open position, exposing the ATP-binding site. Imatinib binds preferentially to the inactive conformation.
- Inactive (DFG-out) conformation: The activation loop folds over the catalytic site. Imatinib, nilotinib, and ponatinib bind to this conformation.
Dasatinib binds to both active and inactive conformations, which partly explains its potency against some imatinib-resistant mutants (except T315I). The T315I "gatekeeper" mutation directly disrupts a critical hydrogen bond between imatinib and the kinase domain, conferring resistance to all first- and second-generation TKIs; only ponatinib and asciminib retain activity against this mutation.
Detection Methods (FISH, PCR)
Accurate detection and quantification of the Philadelphia chromosome and BCR-ABL1 fusion is essential at diagnosis (for treatment selection) and throughout therapy (for molecular monitoring). Three complementary laboratory methods are employed, each with distinct capabilities and limitations.
Conventional Cytogenetics (G-Banded Karyotyping)
Metaphase cytogenetic analysis of bone marrow aspirate remains the standard method for initial detection of t(9;22)(q34;q11). Twenty or more metaphases should be analysed. The Ph chromosome appears as a shortened chromosome 22. Karyotyping also identifies additional cytogenetic abnormalities (clonal evolution) that define accelerated phase.
- Sensitivity: ~5% (1 in 20 metaphases) — cannot detect submicroscopic rearrangements.
- Turnaround: 10–21 days (requires viable dividing cells).
- Limitations: Requires bone marrow aspirate; cannot detect cryptic insertions; inadequate if metaphases are insufficient (<20 analysed).
- Availability: All major Australian haematology centres (Royal Adelaide, Westmead, Peter MacCallum, PathWest, Sullivan Nicolaides).
Fluorescence In Situ Hybridisation (FISH)
Interphase FISH uses fluorescently labelled DNA probes flanking the BCR and ABL1 breakpoint regions. In the absence of rearrangement, separate red (ABL1) and green (BCR) signals are seen; the Ph translocation produces a fusion (yellow/orange) signal. Dual-fusion (D-FISH) and extra-signal (ES-FISH) probe strategies are available.
- Sensitivity: ~1–5% on interphase nuclei (analyses 200–500 cells).
- Turnaround: 2–5 days.
- Applications: Confirming BCR-ABL1 when cytogenetics fails or is inadequate; monitoring when PCR is unavailable; detecting variant translocations (complex three-way rearrangements).
- Limitations: Cannot distinguish transcript type (p210 vs p190); false negatives in CML with cryptic insertions; lower sensitivity than PCR for monitoring.
- MBS consideration: Investigated under MBS item 73307 (in situ hybridisation, per probe); bone marrow FISH typically billed with MBS item 73313.
Real-Time Quantitative PCR (RQ-PCR)
RQ-PCR (also called RT-qPCR) is the gold standard for molecular monitoring of CML and Ph+ ALL. It quantifies BCR-ABL1 mRNA transcript levels from peripheral blood (or bone marrow), expressed on the International Scale (IS) as BCR-ABL1IS percentage. This method is used for:
- Baseline quantification: Establishes the initial BCR-ABL1 level at diagnosis.
- Treatment monitoring: Molecular response milestones guide TKI therapy decisions per ELN 2020 criteria.
- Deep molecular response assessment: Detection of MR4 (BCR-ABL1IS ≤0.01%) and MR4.5 (≤0.0032%) — essential for TFR eligibility.
- Relapse detection: Rising BCR-ABL1 levels indicate loss of response before haematological relapse.
| Milestone | BCR-ABL1IS | Log Reduction | Clinical Significance |
|---|---|---|---|
| Complete cytogenetic response (CCyR) | ≤1% | ≥2 log | Associated with progression-free survival >95% |
| Major molecular response (MMR) | ≤0.1% | ≥3 log | Key treatment milestone at 12 months; optimal response |
| MR4 | ≤0.01% | ≥4 log | Deep molecular response; TFR eligibility threshold |
| MR4.5 | ≤0.0032% | ≥4.5 log | Sustained MR4.5 for ≥2 years preferred for TFR |
Molecular Monitoring Frequency — ELN 2020 Australian Application
BCR-ABL1 Kinase Domain Mutation Analysis
Direct sequencing (Sanger or next-generation sequencing) of the ABL1 kinase domain is indicated when:
- Warning or failure milestones are reached on ELN 2020 criteria.
- Rising BCR-ABL1 levels (≥2 log increase from best response) confirmed on repeat testing.
- Loss of previously achieved MMR.
- Disease progression (accelerated phase or blast crisis).
Over 100 kinase domain mutations have been described; clinically important mutations include T315I (gatekeeper — resistant to imatinib, dasatinib, nilotinib), E255K/V, Y253H, F317L, and V299L. Mutation-specific TKI selection is guided by sensitivity profiles:
| Mutation | Imatinib | Dasatinib | Nilotinib | Ponatinib |
|---|---|---|---|---|
| T315I | Resistant | Resistant | Resistant | Sensitive |
| Y253H | Resistant | Sensitive | Resistant | Sensitive |
| E255K/V | Resistant | Sensitive | Resistant | Sensitive |
| F317L | Sensitive | Resistant | Sensitive | Sensitive |
| V299L | Sensitive | Resistant | Sensitive | Sensitive |
| E255K/V | Resistant | Variable | Resistant | Sensitive |
Mutation analysis is available at major Australian molecular haematology laboratories (e.g., Royal Melbourne Hospital, SA Pathology, Pathology Queensland). Turnaround is typically 2–4 weeks. NGS-based panels can detect low-level mutant clones (<15%) not identified by Sanger sequencing.
Clinical Significance & TKI Targeting
Ph Chromosome in Chronic Myeloid Leukaemia
The Ph chromosome is present in >95% of CML cases at diagnosis and is a defining WHO criterion for the disease. CML follows a triphasic natural history — chronic phase (CP), accelerated phase (AP), and blast crisis (BC) — with TKI therapy dramatically altering the trajectory. The landmark IRIS trial (imatinib vs interferon + cytarabine) demonstrated 8-year CCyR rates of 83% and 8-year overall survival of 85% with imatinib in CP-CML.
Ph Chromosome in Acute Lymphoblastic Leukaemia
Ph+ ALL is characterised by the presence of t(9;22) and/or BCR-ABL1 fusion. It is the most common subtype of ALL in adults (20–30%) but is rare in children (2–5%). The fusion transcript in Ph+ ALL is frequently p190 (e1a2). Ph+ ALL is historically associated with a poor prognosis, but the addition of TKIs to chemotherapy has significantly improved outcomes.
TKI Therapy Algorithm in CML — Australian Practice
TKI Therapy in Ph+ ALL
The standard of care for Ph+ ALL in Australia is a combination of TKI with either intensive chemotherapy or corticosteroid-only protocols (especially in older adults):
- Younger adults (<65 years): Dasatinib 140 mg daily + intensive chemotherapy (e.g., HyperCVAD or the GRAALL-2014 protocol). Dasatinib is preferred over imatinib in ALL due to superior CNS penetration and potency.
- Older adults (≥65 years): Dasatinib + corticosteroid induction (± vincristine) — based on the EWALL-Ph-01 study showing high CR rates with reduced toxicity.
- Paediatric Ph+ ALL: Dasatinib 60 mg/m²/day integrated into high-risk ALL chemotherapy backbone (COG/ALLTogether protocols). Allogeneic HSCT in first CR is recommended for high-risk patients or those with persistent MRD.
- Blinatumomab + TKI: Emerging data (ECOG-ACRIN E1910) suggest blinatumomab (Blincyto®) + TKI may replace chemotherapy in Ph+ ALL — check local ALLG trial availability.
Treatment-Free Remission (TFR)
TFR — discontinuation of TKI with sustained undetectable molecular residual disease — is achievable in ~40–60% of CML patients who achieve durable deep molecular response. Australian eligibility criteria (aligned with ELN 2020 and NCCN):
- CML in chronic phase only.
- TKI therapy for ≥5 years total (≥3 years on first-line TKI; ≥2 years on second-line TKI).
- Confirmed MR4 (BCR-ABL1IS ≤0.01%) for ≥2 years prior to cessation.
- Access to validated IS-standardised RQ-PCR with sensitivity of MR4.5.
- Structured molecular monitoring programme: monthly PCR for 6 months, then 2–3 monthly for ≥5 years.
- No prior AP/BC; no kinase domain mutations.
Allogeneic Haematopoietic Stem Cell Transplant (HSCT)
While TKI therapy is first-line for CML, allogeneic HSCT retains a role in:
- CML in accelerated phase or blast crisis (after TKI + chemotherapy to second chronic phase).
- TKI-refractory CML with no remaining TKI options (especially T315I prior to ponatinib availability or ponatinib failure).
- Ph+ ALL in first complete remission — especially adults with high-risk features, persistent MRD, or not in MMR at end of consolidation.
- Paediatric Ph+ ALL — HSCT in CR1 recommended for those with persistent MRD or high-risk genetics.
Australian transplant centres performing HSCT for CML/Ph+ ALL include Royal Adelaide Hospital, Westmead Hospital, Peter MacCallum Cancer Centre, Royal Melbourne Hospital, and Royal Brisbane and Women's Hospital. Donor registries include the Australian Bone Marrow Donor Registry (ABMDR) and international cord blood banks.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34(4):966–984.
- 2. O'Brien SG, Guilhot F, Larson RA, et al. Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 2003;348(11):994–1004.
- 3. Hughes TP, Saglio G, Quintás-Cardama A, et al. BCR-ABL1 mutation development during first-line treatment with dasatinib or imatinib for chronic myeloid leukemia in chronic phase. Leukemia. 2015;29(9):1832–1838.
- 4. Soverini S, Branford S, Nicolini FE, et al. Implications of BCR-ABL1 kinase domain-mediated resistance in chronic myeloid leukemia. Leuk Res. 2014;38(1):10–20.
- 5. Daver N, Schlenk RF, Russell NH, Levis MJ. Targeting FLT3 mutations in AML: review of current knowledge and evidence. Leukemia. 2019;33(2):299–312. [Note: cross-referenced for methodology context]
- 6. Australian Institute of Health and Welfare (AIHW). Cancer in Aboriginal & Torres Strait Islander people of Australia. AIHW Cat. No. CAN 113. Canberra: AIHW; 2018.
- 7. Rousselot P, Johnson-Ansah M, Huguet F, et al. Personalized daily doses of dasatinib in chronic phase chronic myeloid leukemia: a feasibility study. Haematologica. 2015;100(1):e10–e12.
- 8. Chalandon Y, Thomas X, Hayette S, et al. Randomized study of reduced-intensity chemotherapy combined with imatinib in adults with Ph-positive acute lymphoblastic leukemia. Blood. 2015;125(24):3711–3719.
- 9. Mahon FX, Réa D, Guilhot J, et al. Discontinuation of imatinib in patients with chronic myeloid leukaemia who have maintained complete molecular remission for at least 2 years: the prospective, multicentre Stop Imatinib (STIM) trial. Lancet Oncol. 2010;11(11):1029–1035.
- 10. Cortes JE, Kim DW, Pinilla-Ibarz J, et al. A phase 2 trial of ponatinib in Philadelphia chromosome–positive leukemias. N Engl J Med. 2013;369(19):1783–1796.
- 11. Pharmaceutical Benefits Scheme (PBS). Imatinib, dasatinib, nilotinib, ponatinib — Schedule listings. Australian Government Department of Health. Available at: https://www.pbs.gov.au
- 12. Branford S, Fletcher L, Cross NC, et al. Desirable performance characteristics for BCR-ABL measurement on an international reporting scale to allow consistent assessment of responses in patients with chronic myeloid leukemia. Leukemia. 2007;21(10):2083–2090.
- 13. National Health and Medical Research Council (NHMRC). National statement on ethical conduct in human research. Canberra: NHMRC; 2023 (updated). [For ATSI research considerations]
- 14. Cancer Council Australia. Clinical practice guidelines for the management of chronic myeloid leukaemia. Available at: https://www.cancer.org.au