📋 Key Information Summary
- A leukemoid reaction is a marked, reactive leucocytosis (typically >50 × 10⁹/L) that mimics leukaemia clinically and morphologically.
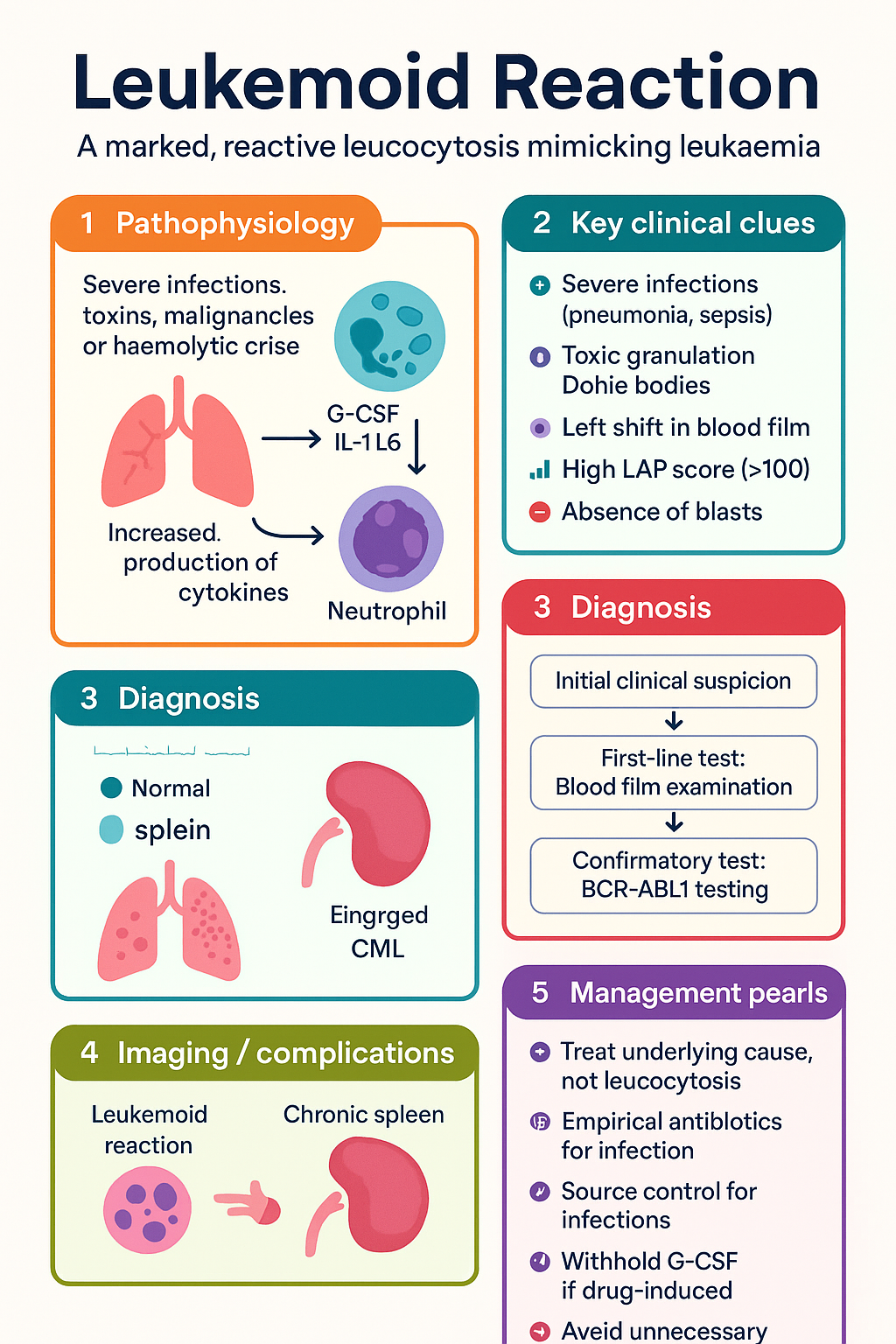
- Common causes in Australia include severe infections (e.g., pneumonia, sepsis), toxins (e.g., colony-stimulating factors), malignancies, and haemolytic or haemorrhagic crises.
- Critical first step: perform a thorough blood film examination to look for a reactive leucocyte picture (toxic granulation, Döhle bodies, left shift) and exclude blasts.
- The Leucocyte Alkaline Phosphatase (LAP) score is a key test; a high score (>100) strongly supports a reactive process.
- BCR-ABL1 (Philadelphia chromosome) testing by PCR or cytogenetics is mandatory to definitively exclude Chronic Myeloid Leukaemia (CML).
- Management is directed entirely at diagnosing and treating the underlying cause; do not treat the high white cell count in isolation.
- Consider plasmapheresis or leukapheresis only in life-threatening hyperviscosity, which is exceedingly rare.
- Special populations: Consider pregnancy-related causes (e.g., eclampsia) and age-specific infections in paediatrics.
- Aboriginal and Torres Strait Islander patients may have a higher burden of underlying infections, rheumatic heart disease, and chronic lung disease, which are common triggers.
- Always consider drug-induced causes, including recombinant G-CSF (e.g., lenograstim) and corticosteroids.
Introduction & Australian Epidemiology
A leukemoid reaction is defined as a markedly elevated white blood cell (WBC) count, typically exceeding 50 × 10⁹/L, driven by a non-neoplastic, reactive process. It is termed "leukemoid" because the degree of leucocytosis and the presence of immature myeloid precursors on the blood film can mimic a primary haematological malignancy, particularly chronic myeloid leukaemia (CML) or a myeloproliferative neoplasm. Accurate distinction is critical to avoid inappropriate cytotoxic therapy.
In the Australian context, the most frequent causes are severe bacterial infections—such as pneumonia, empyema, meningococcal disease, and septic arthritis—often complicated by bacteraemia. Other significant causes include severe tissue injury (burns, trauma), major haemorrhage, haemolytic anaemia, solid tumours with necrosis, and iatrogenic causes like administration of granulocyte colony-stimulating factor (G-CSF). Certain ethnic populations, including Aboriginal and Torres Strait Islander peoples, may present with leukemoid reactions in the setting of rheumatic heart disease or chronic suppurative lung disease.
The cornerstone of diagnosis is a high index of clinical suspicion combined with specific laboratory investigations. Management is never directed at the leucocytosis itself but at identifying and vigorously treating the underlying pathological stimulus.
Definition & Causes
Definition
A leukemoid reaction is a sustained, reactive leucocytosis >50 × 10⁹/L (often >100 × 10⁹/L) in the absence of a primary clonal haematological disorder. The WBC differential usually shows a neutrophilic predominance with a significant "left shift" (increased bands, metamyelocytes, myelocytes), though lymphocytic or eosinophilic variants exist.
Common Causes
| Category | Specific Examples |
|---|---|
| Infections | Severe bacterial pneumonia, empyema, TB, meningococcal meningitis, septic arthritis, infective endocarditis, Clostridioides difficile colitis |
| Toxins/Drugs | Recombinant G-CSF (e.g., lenograstim), corticosteroids, lithium (rarely) |
| Haematological | Severe haemolytic anaemia, major haemorrhage, post-splenectomy state |
| Malignancy | Metastatic solid tumours (especially with necrosis/inflammation), paraneoplastic G-CSF secretion |
| Inflammatory | Rheumatoid arthritis (Felty's syndrome), vasculitis, inflammatory bowel disease flare |
| Other | Severe burns, eclampsia/HELLP syndrome, acute haemolysis (e.g., ABO mismatch) |
Blood Film Features
A careful review of the peripheral blood smear by a haematologist or experienced scientist is mandatory and provides crucial clues to a reactive aetiology.
Typical Findings in a Reactive Leukemoid Reaction
- Left Shift: Prominent numbers of band forms, metamyelocytes, and myelocytes, but with a normal maturation sequence.
- Toxic Changes: Neutrophil toxic granulation (prominent dark cytoplasmic granules), Döhle bodies (small, blue-grey cytoplasmic inclusions), and cytoplasmic vacuolation. These are hallmarks of severe infection/inflammation.
- Absence of Blast Cells: Blasts are typically absent or <5%. Their presence is a red flag for leukaemia.
- Reactive Lymphocytes: If the leucocytosis is lymphocytic, look for atypical lymphocytes (viral syndrome, e.g., EBV).
- Normal Basophil and Eosinophil Counts: Marked basophilia (>2%) or eosinophilia favours a myeloproliferative neoplasm.
- Normal Red Cell and Platelet Morphology: While anaemia may be present from the underlying disease, dysplastic changes in red cells or platelets suggest a primary marrow disorder.
Distinguishing from CML (LAP Score, BCR-ABL)
Differentiating a severe leukemoid reaction from CML is the most critical diagnostic challenge. The following tests are essential.
Management of Underlying Cause
There is no specific treatment for the leukemoid reaction itself. Management is entirely focused on the prompt identification and aggressive treatment of the underlying condition. The elevated WBC count should normalise with successful treatment of the precipitant.
Key Management Principles
- Empirical Antibiotics: If infection is suspected, commence broad-spectrum antibiotics immediately after cultures, following local Australian antimicrobial guidelines (e.g., ceftriaxone + vancomycin for suspected sepsis with unknown source).
- Source Control: Essential for infections like empyema (drainage), abscess (drainage), or septic arthritis (joint washout).
- Stop Iatrogenic Causes: Withhold G-CSF or other offending drugs.
- Treat Malignancy: Initiate appropriate oncological treatment for solid tumours.
- Supportive Care: Aggressive fluid resuscitation, organ support in ICU as required for septic shock.
Special Populations
ATSI Health Considerations
📚 References
- 1. Bain BJ. Diagnosis from the blood smear. N Engl J Med. 2005;353(5):498-507.
- 2. Aster JC. Leukemoid reaction. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on 2024).
- 3. National Health and Medical Research Council (NHMRC). Australian guidelines for the prevention and control of infection in healthcare. Commonwealth of Australia, 2019.
- 4. Australian Commission on Safety and Quality in Health Care (ACSQHC). Bloodstream Infection (Sepsis) Clinical Care Standard. Sydney: ACSQHC; 2022.
- 5. Medical Benefits Schedule (MBS) Online. Item 73316 - Polymerase chain reaction. Australian Government Department of Health. Available at: http://www.mbsonline.gov.au
- 6. The Royal Australian College of General Practitioners (RACGP). Red Book: Guidelines for preventive activities in general practice. 10th edn. East Melbourne, Vic: RACGP, 2024.
- 7. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework 2023 summary report. Canberra: AIHW.
- 8. Savage DG, et al. Leukemoid reaction in solid tumors. Am J Med. 1999;106(5):633-635.
- 9. Hsieh MM, et al. Leukemoid reaction: a diagnostic clue for underlying malignancy. Mayo Clin Proc. 2006;81(4):545.
- 10. RHDAustralia (The Australian Government Department of Health). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd edn. Darwin: Menzies School of Health Research.