📋 Key Information Summary
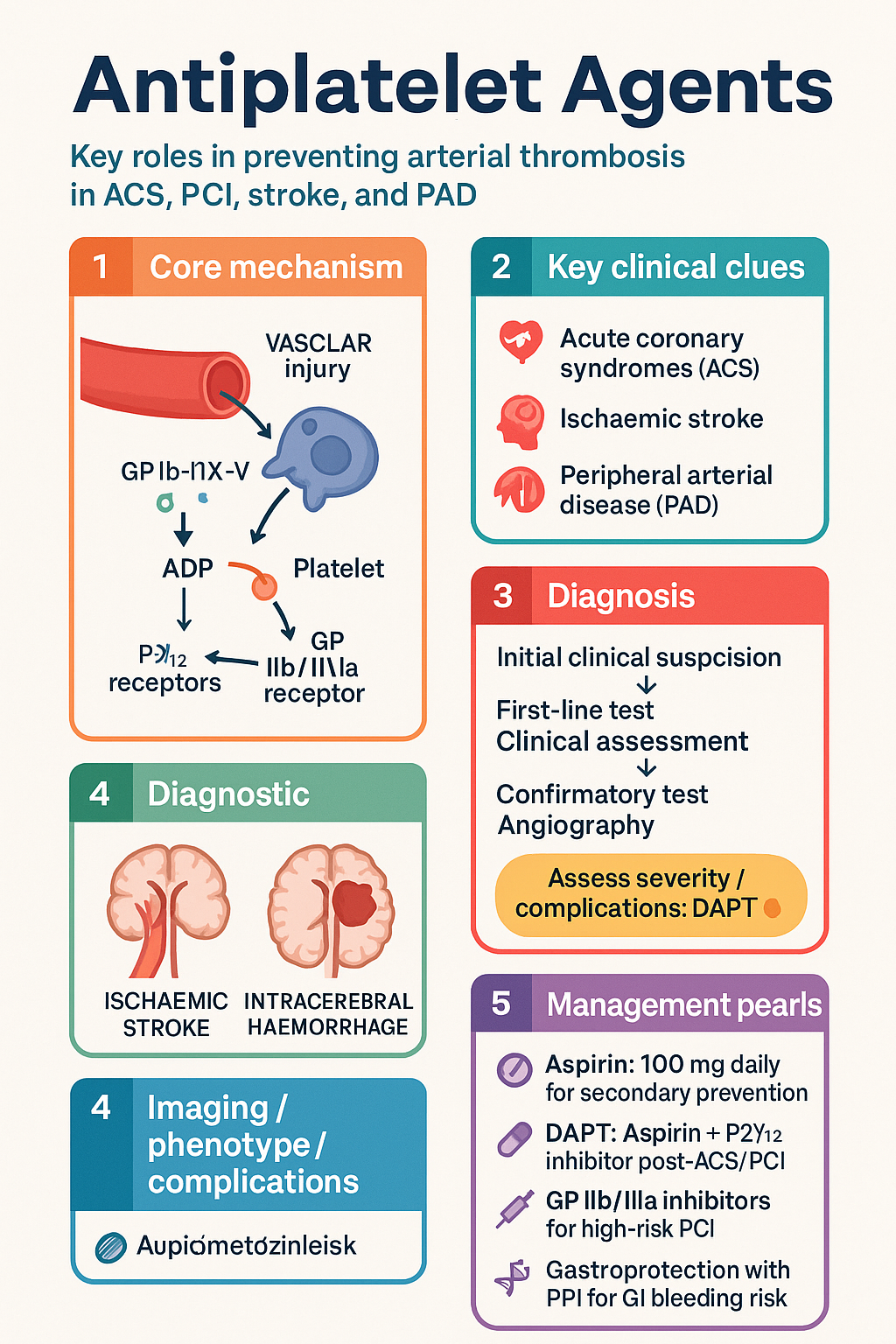
- Antiplatelet agents are cornerstone therapy for preventing arterial thrombosis in acute coronary syndromes (ACS), percutaneous coronary intervention (PCI), ischaemic stroke, and peripheral arterial disease (PAD).
- Aspirin irreversibly acetylates cyclooxygenase-1 (COX-1),reducing thromboxane A2 production. Standard dose is 100 mg (75–150 mg) daily for long-term secondary prevention.
- Dual antiplatelet therapy (DAPT) with aspirin plus a P2Y12 inhibitor is standard post-ACS and post-PCI to mitigate stent thrombosis and recurrent ischaemic events.
- P2Y12 inhibitors: Clopidogrel (prodrug, variable response), Ticagrelor (reversible, more potent, dyspnoea side-effect), and Prasugrel (contraindicated in prior stroke/TIA).
- DAPT duration is individualised: typically 12 months post-ACS, but can be shortened (1–3 months) or extended based on ischaemic vs. bleeding risk (DAPT score).
- GP IIb/IIIa inhibitors (abciximab, eptifibatide, tirofiban) are reserved for high-risk PCI or bail-out situations; administered IV in hospital settings.
- Bleeding is the major risk. Gastroprotection with a PPI is recommended for patients with high GI bleeding risk on DAPT.
- Perioperative management requires careful planning; generally stop ticagrelor 5 days, clopidogrel 5 days, and aspirin 7 days before elective surgery if indicated.
- Pharmacogenomic testing for CYP2C19 loss-of-function alleles can guide clopidogrel use in high-risk settings (e.g., post-PCI).
- Aspirin is not recommended for primary prevention of cardiovascular disease in the general population due to bleeding risk outweighing benefit.
- Aboriginal and Torres Strait Islander peoples have higher CVD burden; ensure equitable access, health-literate education, and consideration of remote pharmacy supply.
Introduction & Australian Epidemiology
Antiplatelet agents form a critical pillar in the management of atherothrombotic disease, targeting distinct pathways in platelet activation and aggregation to prevent arterial thrombosis. Their use is firmly established in the secondary prevention of cardiovascular,cerebrovascular,and peripheral arterial diseases.
In Australia, cardiovascular disease (CVD) remains a leading cause of mortality,accounting for approximately 25% of all deaths. Acute coronary syndromes (ACS) affect over 50,000 Australians annually. The burden is significantly higher among Aboriginal and Torres Strait Islander peoples,who experience CVD at younger ages and with greater severity. Antiplatelet therapy is integral to national guidelines from the Cardiac Society of Australia and New Zealand (CSANZ) and the National Heart Foundation (NHF).
Platelet Physiology & Activation
Platelets are anucleate cell fragments derived from megakaryocytes. Upon vascular injury,exposed collagen and von Willebrand factor (vWF) mediate platelet adhesion via glycoprotein (GP) Ib-IX-V and GP VI receptors. This triggers activation,leading to:
- Release of agonists such as ADP and thromboxane A2 (TxA2),which amplify activation via P2Y12 and TxA2 receptors.
- Shape change and granule secretion.
- Conformational activation of the GP IIb/IIIa receptor,which binds fibrinogen and mediates platelet cross-linking,forming the final common pathway of aggregation.
Antiplatelet drugs inhibit key steps in this cascade: TxA2 synthesis (aspirin),ADP signalling (P2Y12 inhibitors),and fibrinogen binding (GP IIb/IIIa inhibitors).
Aspirin (COX-1 Inhibition)
Aspirin irreversibly acetylates serine-530 of cyclooxygenase-1 (COX-1),preventing the conversion of arachidonic acid to TxA2 for the platelet's lifespan (7–10 days). This effect reduces platelet aggregation in response to various stimuli.
P2Y12 Inhibitors (Clopidogrel, Ticagrelor)
These agents block the P2Y12 ADP receptor on platelets,attenuating activation and amplification. Choice depends on clinical context (ACS vs. elective PCI),ischaemic/bleeding risk,and patient factors.
| Feature | Clopidogrel | Ticagrelor |
|---|---|---|
| Mechanism | Irreversible P2Y12 antagonist (prodrug) | Reversible, direct-acting P2Y12 antagonist |
| Onset | 2–6 hours (300–600 mg load) | 30 minutes (180 mg load) |
| ACS Dose | 300–600 mg load, then 75 mg daily | 180 mg load, then 90 mg BD |
| Key Limitation | Variable response due to CYP2C19 polymorphisms | Dyspnoea (≈14%),ventricular pauses |
| Perioperative stop | 5 days | 5 days |
GP IIb/IIIa Inhibitors & Indications
Glycoprotein IIb/IIIa inhibitors are intravenous agents that block the final common pathway of platelet aggregation. They are used in acute,hospital-based settings for high-risk interventions.
Key Indications
- High-risk ACS with planned early invasive strategy.
- Bail-out situation during PCI (e.g., thrombus,no-reflow).
- Elective high-risk PCI (e.g., complex anatomy,left main).
Monitoring
- Clinical: Signs of bleeding (gums, bruising,melaena,haematuria),dyspnoea (ticagrelor),adherence.
- Laboratory: Baseline FBC; monitor for thrombocytopaenia (especially after GP IIb/IIIa inhibitor exposure). Routine platelet function testing is not standard but may be used in specialised centres to assess on-treatment reactivity (e.g., VerifyNow assay).
- Pharmacogenomic: Consider CYP2C19 genotyping for poor metabolisers on clopidogrel in high-risk post-PCI settings to guide alternative P2Y12 inhibitor use.
Special Populations
📚 References
- 1. Chew DP, Scott IA, Cullen L, et al. National Heart Foundation of Australia & Cardiac Society of Australia and New Zealand: Australian Clinical Guidelines for the Management of Acute Coronary Syndromes 2016. Heart, Lung and Circulation. 2016;25(9):895-951.
- 2. Valgimigli M, Bueno H, Byrne RA, et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease. Eur Heart J. 2018;39(3):213-260.
- 3. American College of Cardiology/American Heart Association. ACC/AHA Guideline for the Management of Patients with Acute Coronary Syndromes (2021).
- 4. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Australia 2023. Cat. no. CVD 86. Canberra: AIHW.
- 5. NHMRC. Australian Guidelines for the Prevention and Control of Infection in Healthcare (2019). (Context for IE prophylaxis, where relevant).
- 6. Bhatt DL, Fox KAA, Hacke W, et al. Clopidogrel and Aspirin versus Aspirin Alone for the Prevention of Atherothrombotic Events. N Engl J Med. 2006;354:1706-1717.
- 7. Wallentin L, Becker RC, Budaj A, et al. Ticagrelor versus Clopidogrel in Patients with Acute Coronary Syndromes. N Engl J Med. 2009;361:1045-1057.
- 8. The EPIC Investigators. Use of a monoclonal antibody directed against the platelet glycoprotein IIb/IIIa receptor in high-risk coronary angioplasty. N Engl J Med. 1994;330:956-961.
- 9. RACGP. Smoking, nutrition, alcohol, physical activity (SNAP): A population health guide to behavioural risk factors in general practice. 2nd edition. (Context for primary prevention).
- 10. Aspirin in the primary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised controlled trials. Lancet. 2009;373:1849-1860.
- 11. NHMRC. National Statement on Ethical Conduct in Human Research (2023 updated). (Context for pharmacogenomic testing).
- 12. The Royal Australian College of General Practitioners. Guidelines for preventive activities in general practice. 10th edition. (Primary prevention context).