📋 Key Information Summary
- Splenomegaly is defined as splenic enlargement beyond its normal weight of approximately 150g or length >12 cm on imaging.
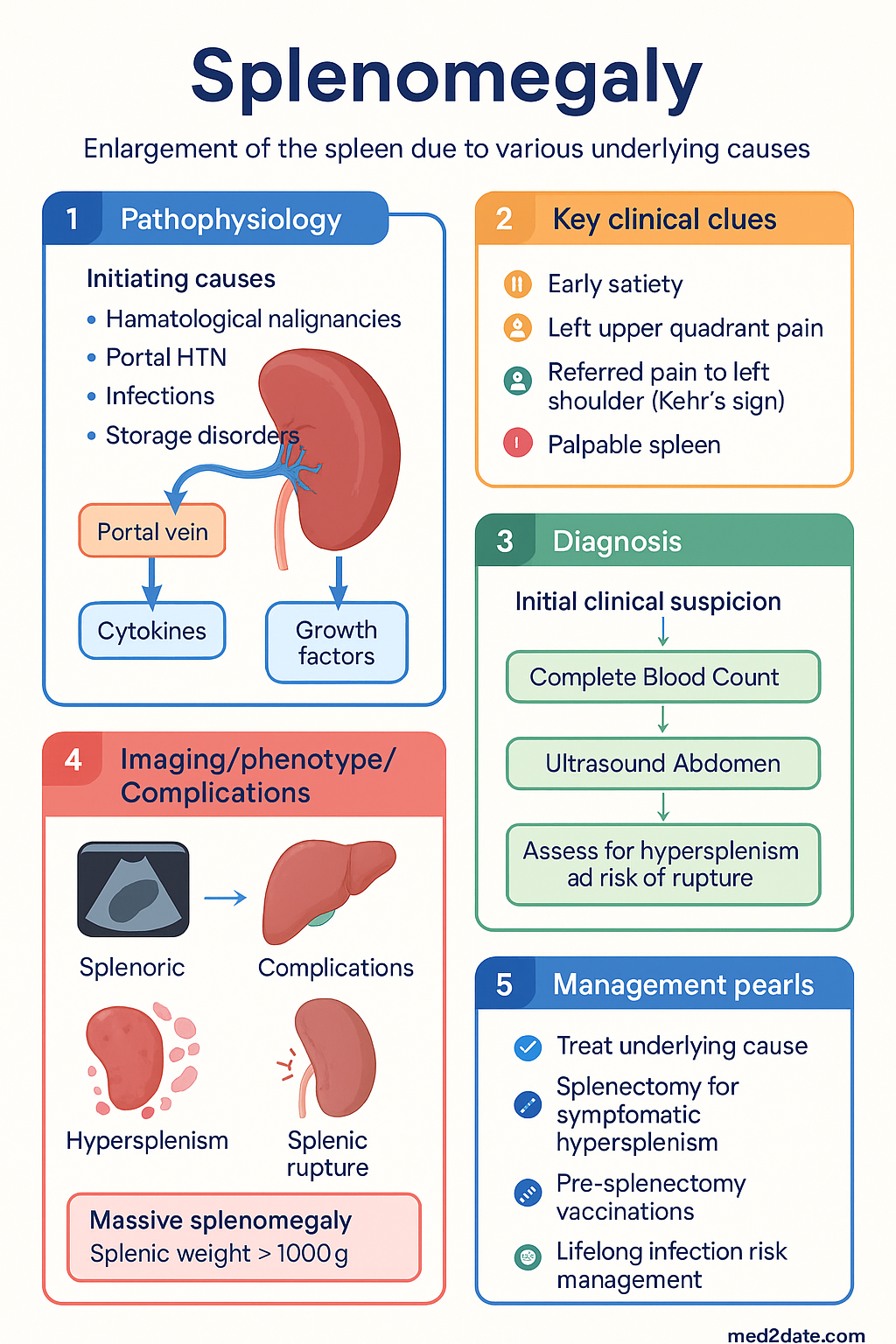
- Systematic classification is essential: haematological malignancies, portal hypertension, infections, and storage disorders are the four major aetiological categories.
- Clinical examination for splenomegaly has moderate sensitivity; ultrasound is the first-line imaging modality for confirmation and measurement.
- Initial investigation requires a complete blood count, peripheral blood film, and liver function tests to narrow the differential.
- Massive splenomegaly (splenic weight >1000g or extending to the iliac crest) is highly suggestive of myeloproliferative neoplasms or chronic lymphocytic leukaemia.
- Management is directed at the underlying cause; splenectomy is considered for symptomatic hypersplenism, diagnostic uncertainty, or specific haematological disorders.
- All patients with splenomegaly require assessment for hypersplenism (cytopenias) and risk of splenic rupture.
- Key investigations include FBC, blood film, LDH, liver function, and imaging (ultrasound ± CT).
- Consider bone marrow biopsy in cases of unexplained cytopenias or suspected haematological malignancy.
- Post-splenectomy patients require lifelong vaccinations (pneumococcal, meningococcal, Haemophilus influenzae type b) and may need prophylactic antibiotics.
- Aboriginal and Torres Strait Islander populations have a higher burden of infections and conditions leading to splenomegaly, requiring culturally safe, community-based care.
Introduction & Australian Epidemiology
Splenomegaly is a clinical sign, not a disease, indicating an underlying pathological process. It arises from numerous causes including haematological malignancies, portal hypertension, infections, and storage disorders, requiring systematic evaluation. In Australia, the epidemiology of splenomegaly reflects the diverse population, with common causes including chronic liver disease, haematological malignancies, and infections such as Ross River virus and Barmah Forest virus. The prevalence of specific conditions varies, with haematological malignancies being a significant consideration in older adults and infections more common across all age groups.
The spleen acts as a filter for blood, participating in immune surveillance and haematopoiesis. Its enlargement can lead to hypersplenism, causing cytopenias, and increases the risk of traumatic rupture. A structured approach to investigation is crucial to identify the underlying aetiology and guide management.
Causes & Classification
Causes of splenomegaly are broadly classified into five categories:
| Category | Examples |
|---|---|
| Congestive / Portal Hypertension | Cirrhosis (alcohol, viral hepatitis), Budd-Chiari syndrome, portal vein thrombosis, hepatic schistosomiasis |
| Infections | Acute: Infectious mononucleosis (EBV), cytomegalovirus, HIV, viral hepatitis, Ross River virus, Barmah Forest virus. Chronic: Tuberculosis, malaria, brucellosis, infective endocarditis, visceral leishmaniasis. |
| Haematological | Malignant: Myeloproliferative neoplasms (e.g., primary myelofibrosis, CML), lymphoproliferative disorders (e.g., CLL, lymphoma), hairy cell leukaemia. Benign: Haemolytic anaemias (e.g., hereditary spherocytosis, thalassaemia major), megaloblastic anaemia. |
| Inflammatory / Autoimmune | Rheumatoid arthritis (Felty syndrome), systemic lupus erythematosus, sarcoidosis |
| Infiltrative / Storage | Gaucher disease, Niemann-Pick disease, amyloidosis, metastatic cancer (rare) |
Clinical Features & Examination
The spleen is normally not palpable. Palpability suggests enlargement, but a palpable spleen is not always pathological (e.g., in thin individuals). Symptoms may be absent or include early satiety, left upper quadrant pain or fullness, and referred pain to the left shoulder (Kehr's sign).
Physical Examination Technique
- Position: Patient supine, with knees flexed to relax abdominal muscles. Examine from the right side.
- Palpation: Start in the right iliac fossa. Ask the patient to take a deep breath. Feel for the splenic edge moving towards the fingertips on inspiration. A palpable spleen is at least 1.5-2x enlarged.
- Percussion: Traube's space (left 6th-10th ribs, anterior axillary line) may be dull. Castle's method: percuss from the left costal margin towards the umbilicus; loss of tympany may indicate splenomegaly.
Clinical examination has limited sensitivity (60-70%) and specificity. Ultrasound is required for confirmation.
Investigations (FBC, Film, Imaging)
Investigation is tailored to the clinical context. A stepwise approach is recommended.
Initial Investigations
Further Investigations (Based on Clinical Suspicion)
Management & Splenectomy Indications
Management is entirely directed at the underlying cause. Symptomatic treatment is limited.
Medical Management
- Treat the underlying cause: Antibiotics for infections, disease-modifying therapy for autoimmune conditions, targeted therapy for haematological malignancies.
- Manage hypersplenism: If cytopenias are severe and symptomatic, treat the primary disease. Splenectomy is a last resort.
Splenectomy: Indications and Considerations
Splenectomy (laparoscopic preferred) is considered for:
- Diagnostic: Undiagnosed splenomegaly after exhaustive non-invasive workup and bone marrow biopsy.
- Therapeutic - Hypersplenism: Severe, symptomatic cytopenias (e.g., transfusion-dependent anaemia, life-threatening thrombocytopenia) unresponsive to medical therapy.
- Therapeutic - Specific Diseases:
- Hereditary spherocytosis (with significant anaemia or gallstones).
- Primary myelofibrosis (with symptomatic massive splenomegaly).
- Hairy cell leukaemia (if refractory to medical therapy).
- Immune thrombocytopenia (ITP) (refractory, chronic).
- Massive Splenomegaly: For symptom relief (pain, early satiety, mechanical compression).
- Splenic Rupture: Emergency splenectomy for traumatic rupture.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
The burden of conditions causing splenomegaly is higher among Aboriginal and Torres Strait Islander peoples, particularly in remote communities. A culturally safe, holistic, and community-embedded approach is essential.
📚 References
- 1. Pozo AL, Godfrey EM, Bowles KM. Splenomegaly: investigation, diagnosis and management. Blood Rev. 2009;23(3):105-111.
- 2. Di Sabatino A, Carsetti R, Corazza GR. Post-splenectomy and hyposplenic states. Lancet. 2011;378(9785):86-97.
- 3. Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice. 9th edn. East Melbourne: RACGP; 2016.
- 4. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework. Canberra: AIHW; 2023.
- 5. Australasian Society for Infectious Diseases (ASID). Guidelines for the prevention of infection in patients with an absent or dysfunctional spleen. Sydney: ASID; 2019.
- 6. Tefferi A. Primary myelofibrosis: 2023 update on diagnosis, risk-stratification, and management. Am J Hematol. 2023;98(5):827-847.
- 7. Bloodsafe. Pre-splenectomy vaccination guide. [Internet]. Available from: https://www.bloodsafe.com.au
- 8. Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook. Australian Government Department of Health; 2022.
- 9. Lane S, et al. The post-splenectomy state. Aust Prescr. 2021;44(1):4-10.
- 10. National Health and Medical Research Council (NHMRC). Australian guidelines to reduce health risks from drinking alcohol. Canberra: NHMRC; 2020. [For cirrhosis prevention context].