📋 Key Information Summary
- Vitamin B12 (cobalamin) deficiency causes megaloblastic anaemia and subacute combined degeneration (SCD) of the posterior and lateral columns of the spinal cord — neurological damage may be irreversible if treatment is delayed.
- Pernicious anaemia (autoimmune gastritis with loss of intrinsic factor) is the most common cause in Australia, accounting for 20–50% of cases.
- Other major causes include malabsorptive conditions (coeliac disease, Crohn's ileitis, gastrectomy, bariatric surgery), inadequate dietary intake (vegan/vegetarian diets), and drug-induced impairment (metformin, PPIs, nitrous oxide).
- Serum B12 <150 pmol/L is consistent with deficiency; 150–250 pmol/L is indeterminate and requires functional markers (methylmalonic acid [MMA] and homocysteine) to confirm.
- MMA and homocysteine are elevated in true B12 deficiency and are the most reliable functional tests when serum B12 is in the indeterminate range.
- Anti-intrinsic factor antibodies are highly specific for pernicious anaemia (95%) and should be tested when pernicious anaemia is suspected.
- First-line treatment is intramuscular hydroxocobalamin — loading dose of 1 mg IM on alternate days for 2 weeks, then maintenance of 1 mg IM every 2–3 months for life if pernicious anaemia.
- Oral high-dose cyanocobalamin (1000 µg daily) is an acceptable alternative for patients without severe neurological features or malabsorption, and is PBS-listed.
- Always assess for neurological involvement — paraesthesias, gait ataxia, proprioceptive loss, cognitive impairment — as urgent treatment prevents permanent cord damage.
- Concurrent folate deficiency is common; always check serum folate and correct both simultaneously to avoid precipitating subacute combined degeneration.
- Aboriginal and Torres Strait Islander peoples may have higher rates of B12 deficiency related to nutritional factors, H. pylori infection, and reduced access to specialist gastroenterology services in remote areas.
- Monitor reticulocyte count at 1 week; reticulocyte peak confirms response. Neurological improvement may take 3–6 months or longer.
Introduction & Australian Epidemiology
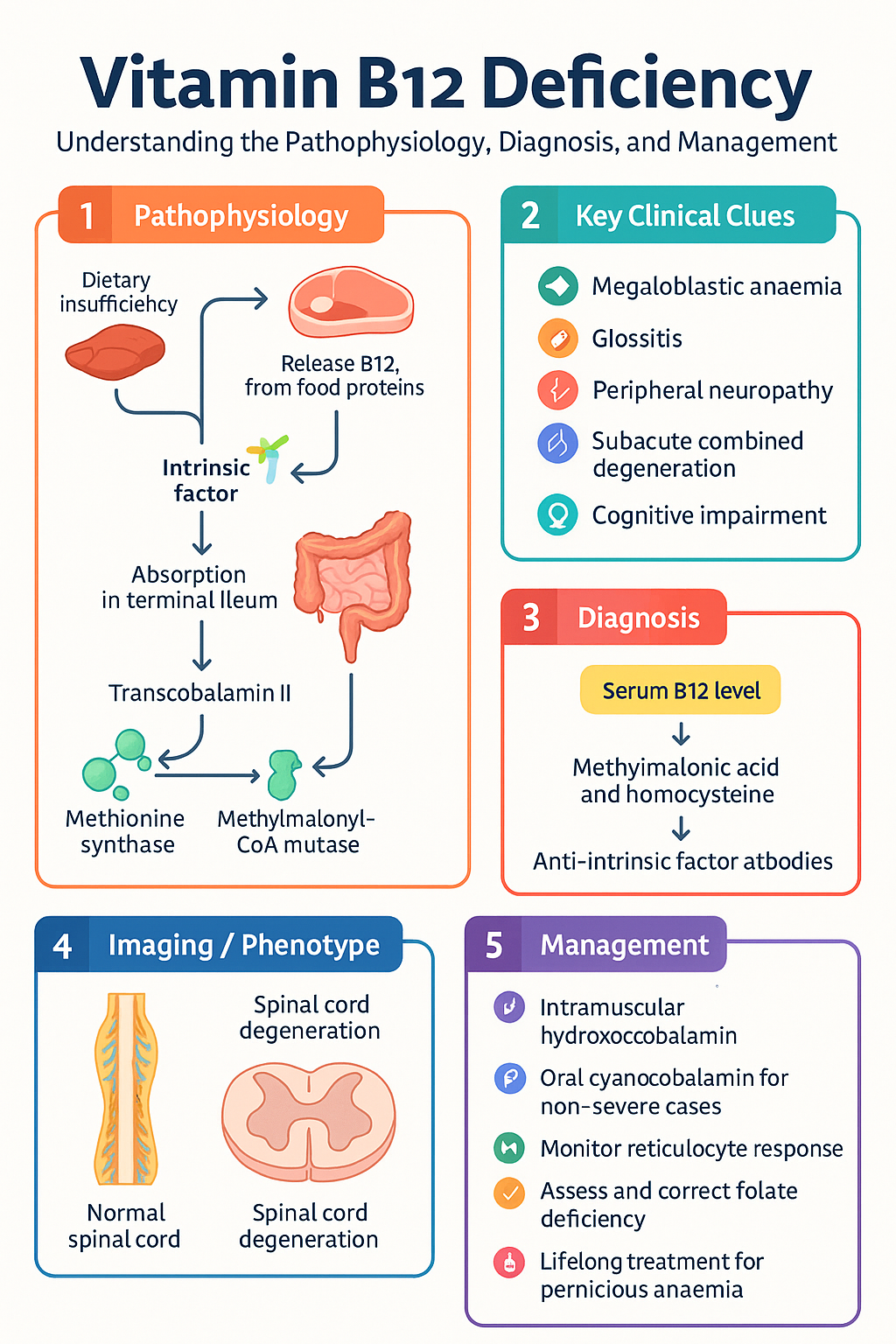
Vitamin B12 (cobalamin) is an essential water-soluble vitamin required for DNA synthesis, erythropoiesis, and maintenance of myelin integrity in the central and peripheral nervous systems. Deficiency results in megaloblastic anaemia and, when prolonged, subacute combined degeneration of the spinal cord — a potentially irreversible demyelinating condition affecting the posterior and lateral columns.
B12 deficiency is common in Australian primary care. Prevalence estimates suggest 5–6% of the general population aged ≥50 years have low serum B12, with significantly higher rates among older adults in residential aged care (up to 20%), vegans and vegetarians (up to 50–80%), and individuals with gastrointestinal disease or prior surgery. The Australian Institute of Health and Welfare (AIHW) data indicate that B12 deficiency-related presentations account for a significant proportion of nutritional anaemia diagnoses nationally.
In Australia, the most frequent aetiology is pernicious anaemia — an autoimmune condition characterised by destruction of gastric parietal cells and loss of intrinsic factor production — followed by malabsorptive disorders including coeliac disease, inflammatory bowel disease affecting the terminal ileum, and iatrogenic causes such as post-gastrectomy and post-bariatric surgery states. Dietary insufficiency is increasingly relevant given rising rates of plant-based diets, particularly in younger Australians.
The clinical spectrum ranges from asymptomatic biochemical deficiency with subtle haematological changes to severe megaloblastic anaemia with pancytopenia and profound neurological disability. Early recognition and treatment are critical, as neurological damage — particularly subacute combined degeneration — may become irreversible within months if untreated.
This guideline provides a comprehensive framework for the diagnosis and management of B12 deficiency in Australian clinical practice, aligned with current evidence and Australian therapeutic standards.
Pathophysiology
Vitamin B12 is obtained exclusively from animal-derived dietary sources (meat, dairy, eggs, fish) and requires a complex absorption pathway:
- Dietary B12 is released from food proteins by gastric acid and pepsin.
- Free B12 binds to R-proteins (haptocorrin) in the stomach.
- In the duodenum, pancreatic proteases degrade R-proteins, releasing B12 which then binds to intrinsic factor (IF) — a glycoprotein secreted by gastric parietal cells.
- The B12–IF complex is absorbed in the terminal ileum via the cubilin–amnionless receptor complex.
- Absorbed B12 binds to transcobalamin II (TC II) in the portal circulation and is delivered to tissues.
Metabolic roles: B12 serves as a cofactor for two critical enzymatic reactions:
| Enzyme Reaction | Consequence of B12 Deficiency |
|---|---|
| Methionine synthase (converts homocysteine → methionine using methylcobalamin) | ↑ Homocysteine; impaired methylation reactions; folate trapping (methylfolate cannot be demethylated → functional folate deficiency) |
| Methylmalonyl-CoA mutase (converts methylmalonyl-CoA → succinyl-CoA using adenosylcobalamin) | ↑ Methylmalonic acid (MMA); impaired fatty acid and amino acid metabolism; neurotoxicity from abnormal odd-chain fatty acid incorporation into myelin |
Haematological effects: Impaired DNA synthesis leads to megaloblastic erythropoiesis — large erythroblasts with immature nuclei relative to cytoplasm. This extends to all rapidly dividing cells, explaining the pancytopenia and glossitis seen in severe deficiency.
Neurological effects: Demyelination of the posterior columns (dorsal columns) causes loss of proprioception and vibration sense; lateral corticospinal tract involvement causes upper motor neuron signs (spasticity, hyperreflexia, extensor plantar responses). Peripheral neuropathy with axonal degeneration also occurs. The mechanism is thought to relate to impaired methylation of myelin basic protein and accumulation of abnormal fatty acids in myelin sheaths.
Causes of B12 Deficiency
Pernicious Anaemia
Pernicious anaemia (PA) is the most common cause of B12 deficiency in Australia, accounting for 20–50% of cases. It is an autoimmune condition characterised by:
- Autoimmune destruction of gastric parietal cells → atrophic gastritis, achlorhydria, and loss of intrinsic factor production.
- Presence of anti-parietal cell antibodies (sensitivity ~80%, specificity low) and/or anti-intrinsic factor antibodies (sensitivity ~50%, specificity ~95%).
- Increased incidence in patients with other autoimmune conditions: autoimmune thyroid disease (Hashimoto's, Graves'), type 1 diabetes mellitus, vitiligo, and Addison's disease.
- Typically presents in patients aged ≥60 years, but may occur at any age.
- Slight female predominance (F:M = 1.5:1).
Malabsorptive Causes
| Cause | Mechanism | Notes |
|---|---|---|
| Coeliac disease | Villous atrophy of small bowel mucosa; reduced absorptive surface | Screen with anti-tTG IgA; B12 deficiency present in 5–15% at diagnosis |
| Crohn's disease (ileal) | Terminal ileal inflammation or resection impairs B12–IF complex absorption | Risk increases with >60 cm ileal resection |
| Total/partial gastrectomy | Loss of parietal cells → no intrinsic factor; reduced acid → impaired B12 release from food | Deficiency almost universal after total gastrectomy; supplement prophylactically |
| Bariatric surgery (Roux-en-Y, one-anastomosis gastric bypass) | Bypass of duodenum/jejunum; reduced IF; reduced acid; reduced R-protein binding | Sleeve gastrectomy lower risk but still possible; lifelong monitoring required |
| Chronic pancreatitis | Impaired pancreatic protease secretion → failure to release B12 from R-proteins | Usually only causes clinically significant deficiency in advanced disease |
| Bacterial overgrowth (SIBO) | Bacteria consume B12 before absorption; may also damage mucosa | Associated with anatomical abnormalities, motility disorders, achlorhydria |
| Diphyllobothrium latum (fish tapeworm) | Parasite competes for dietary B12 in the intestinal lumen | Rare in Australia; seen in patients consuming raw freshwater fish from endemic regions |
Dietary Insufficiency
- Strict vegans (no animal products): 5–10 year hepatic B12 stores become depleted; deficiency develops in 2–5 years without supplementation.
- Lacto-ovo vegetarians: lower risk but still at increased risk, especially elderly vegetarians with reduced absorptive capacity.
- Restrictive eating disorders (anorexia nervosa, ARFID): may present with B12 and other micronutrient deficiencies.
Drug-Induced Causes
| Drug | Mechanism | Clinical Relevance |
|---|---|---|
| Metformin | Interferes with calcium-dependent IF–B12 complex uptake in terminal ileum | 5–10% of long-term users develop low B12; screen after ≥4 years of use |
| Proton pump inhibitors (PPIs) | Reduced gastric acid → impaired release of protein-bound B12 from food | Clinically relevant with prolonged use (>3–4 years); omeprazole, esomeprazole, pantoprazole |
| H2-receptor antagonists | Reduced acid secretion (less effect than PPIs) | Less clinically significant than PPIs |
| Colchicine | Impairs IF–B12 complex uptake; mucosal damage | Relevant in long-term gout prophylaxis |
| Nitrous oxide | Oxidises cobalt atom in B12 → irreversible inactivation of methionine synthase | Can precipitate acute SCD in patients with borderline B12 stores; recreational use is an emerging cause |
Other Causes
- Pregnancy and lactation: Increased demand; may unmask marginal deficiency.
- Transcobalamin II deficiency: Rare autosomal recessive condition presenting in infancy.
- Functional B12 deficiency: B12 bound to haptocorrin (inactive) is elevated while TC II-bound (active) B12 is low; serum B12 may be normal — check holotranscobalamin (active B12) if available.
Clinical Features
The clinical presentation of B12 deficiency spans a wide spectrum, from asymptomatic biochemical abnormality to severe haematological and neurological disease. Haematological and neurological manifestations may occur independently — a patient can develop subacute combined degeneration without significant anaemia, and vice versa.
Haematological Manifestations
| Feature | Details |
|---|---|
| Megaloblastic anaemia | Macrocytic (MCV typically >100 fL), with oval macrocytes and hypersegmented neutrophils (≥5 lobes) on blood film; may see leukopenia, thrombocytopenia, or pancytopenia in severe cases |
| Haemolysis | Ineffective erythropoiesis with intramedullary destruction; mildly elevated LDH, indirect bilirubin, low haptoglobin |
| Pancytopenia | Severe deficiency may mimic myelodysplastic syndrome or aplastic anaemia; correctable with B12 replacement |
| Glossitis | Beefy-red, smooth, sore tongue (Hunter's glossitis) — reflects mucosal megaloblastic change |
| Angular stomatitis | Cracking at the corners of the mouth |
Neurological Manifestations
| Feature | Details |
|---|---|
| Peripheral neuropathy | Symmetrical distal paraesthesias (tingling, numbness, "pins and needles") in hands and feet; may progress proximally; reduced ankle reflexes |
| Subacute combined degeneration (SCD) | Posterior column dysfunction: loss of proprioception and vibration sense, sensory ataxia, positive Romberg's sign. Lateral column dysfunction: spasticity, hyperreflexia, extensor plantar responses, weakness |
| Gait disturbance | Ataxic, wide-based gait; may be mistaken for normal-pressure hydrocephalus or other causes of gait disorder in the elderly |
| Cognitive impairment | Memory loss, confusion, irritability, depression; may present as dementia — always check B12 in new cognitive decline |
| Optic neuropathy | Rare; bilateral progressive visual loss; tobacco-alcohol amblyopia pattern |
| Psychiatric features | Megaloblastic madness — psychosis, paranoia, hallucinations; may be the presenting feature in the absence of anaemia |
Other Manifestations
- Fatigue, weakness, dyspnoea on exertion (from anaemia).
- Anorexia, weight loss, mild diarrhoea.
- Recurrent oral ulcers.
- Hyperpigmentation of skin creases (more common in darker-skinned individuals).
- Infertility and recurrent miscarriage (rare; associated with severe deficiency).
Investigations
Laboratory Investigations
Investigations to Identify the Underlying Cause
- Coeliac serology: Anti-tissue transglutaminase IgA (anti-tTG IgA) with total IgA — MBS Item 66595. Screen all patients with unexplained B12 deficiency.
- Gastroscopy with biopsies: Indicated if PA suspected (look for atrophic gastritis, intestinal metaplasia), or if coeliac serology positive. Consider in patients with upper GI symptoms or iron deficiency coexisting with B12 deficiency.
- Schilling test: Historical gold standard — now obsolete in Australia. Replaced by anti-IF antibody testing and clinical assessment.
- Colonoscopy: If Crohn's disease suspected or if ileal disease on imaging.
- CT/MRI abdomen: If ileal Crohn's disease, SIBO, or small bowel pathology suspected.
Neurological Investigations
- MRI spine: In patients with suspected subacute combined degeneration — look for T2 hyperintensity in posterior and lateral columns (inverted V sign on axial images).
- Nerve conduction studies / EMG: May confirm sensorimotor axonal or demyelinating peripheral neuropathy.
- Neuropsychological testing: In patients presenting with cognitive impairment or psychiatric features.
Diagnostic Algorithm
Management
Principles of Treatment
- Treat the underlying cause where possible (e.g., gluten-free diet for coeliac disease, treat H. pylori, discontinue/limit causative drugs).
- Replace B12 — intramuscular hydroxocobalamin is first-line.
- Always check and correct concurrent folate deficiency.
- Do NOT give folate alone without B12 — this may mask the haematological picture while allowing irreversible neurological progression.
- Monitor for hypokalaemia during treatment (rapid erythropoiesis consumes potassium).
Intramuscular Hydroxocobalamin — First-Line Therapy
Oral Cyanocobalamin — Alternative for Selected Patients
Management of Specific Scenarios
| Scenario | Management |
|---|---|
| Severe anaemia (Hb <70 g/L) with cardiac compromise | Transfuse packed red blood cells cautiously (risk of fluid overload); commence B12 replacement simultaneously; monitor potassium closely |
| Subacute combined degeneration | Urgent IM hydroxocobalamin 1 mg daily for 1 week, then alternate days for 2 weeks, then maintenance; physiotherapy and rehabilitation referral |
| Nitrous oxide exposure with neurological symptoms | Stop nitrous oxide immediately; IM hydroxocobalamin 1 mg daily for at least 2 weeks; high-dose oral B12 supplementation may also be needed |
| Post-bariatric surgery prophylaxis | Lifelong oral B12 1000 µg daily OR IM hydroxocobalamin 1 mg every 3 months; annual B12 monitoring |
| Vegan/vegetarian patients | Oral B12 1000 µg daily (dietary supplementation); if already deficient, IM loading then oral maintenance |
| Concurrent folate deficiency | Folic acid 5 mg PO daily for 4 months (or 1 mg daily in pregnancy); always give with B12 replacement |
Folic Acid Replacement
Monitoring & Follow-Up
When to Refer
- Neurologist: Suspected subacute combined degeneration, significant peripheral neuropathy, or diagnostic uncertainty.
- Gastroenterologist: Suspected coeliac disease, Crohn's disease, suspected pernicious anaemia for gastroscopy/biopsy, or unexplained malabsorption.
- Haematologist: Pancytopenia, diagnostic uncertainty (e.g., concern for myelodysplastic syndrome), or refractory B12 deficiency.
- Dietitian: All vegan/vegetarian patients with deficiency; post-bariatric surgery patients.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Quick Reference — Treatment Summary
📚 References
- 1. Green R, Allen LH, Bjørke-Monsen AL, et al. Vitamin B12 deficiency. Nature Reviews Disease Primers. 2017;3:17040.
- 2. Stabler SP. Vitamin B12 deficiency. New England Journal of Medicine. 2013;368(2):149–160.
- 3. Devalia V, Hamilton MS, Molloy AM. Guidelines for the diagnosis and treatment of cobalamin and folate disorders. British Journal of Haematology. 2014;166(4):496–513.
- 4. The Royal Australian College of General Practitioners. RACGP National guide to a preventive health assessment for Aboriginal and Torres Strait Islander people. 3rd ed. East Melbourne: RACGP; 2018.
- 5. Australian Institute of Health and Welfare. Aboriginal and Torres Strait Islander health performance framework 2020 summary report. Canberra: AIHW; 2020.
- 6. Hunt A, Harrington D, Robinson S. Vitamin B12 deficiency. BMJ. 2014;349:g5226.
- 7. Andrès E, Serraj K, Zhu J, Vermorken AJM. The pathophysiology of huge vitamin B12 deficiency. Annals of Hematology. 2013;92(10):1297–1304.
- 8. Langan RC, Goodbred AJ. Vitamin B12 deficiency: recognition and management. American Family Physician. 2017;96(6):384–389.
- 9. Wielders JPM, van Wijk JM, Engelen M, et al. Efficacy of oral supplementation with high-dose cyanocobalamin versus intramuscular hydroxocobalamin. European Journal of Clinical Investigation. 2015;45(10):1037–1044.
- 10. National Health and Medical Research Council. Nutrient reference values for Australia and New Zealand including recommended dietary intakes. Canberra: NHMRC; 2006 (updated 2017).
- 11. O'Leary F, Samman S. Vitamin B12 in health and disease. Nutrients. 2010;2(3):299–316.
- 12. Kibirige D, Mwebaze R. Vitamin B12 deficiency among patients with diabetes mellitus: is routine screening and supplementation justified? Journal of Diabetes & Metabolic Disorders. 2013;12:17.
- 13. Australian Commission on Safety and Quality in Health Care. National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2017.
- 14. Toh BH. Pathophysiology and laboratory diagnosis of pernicious anemia. Immunology Research. 2017;65(1):32–36.
- 15. Moore E, Mander A, Ames D, et al. Cognitive impairment and vitamin B12: a review. International Psychogeriatrics. 2012;24(4):541–556.