📋 Key Information Summary
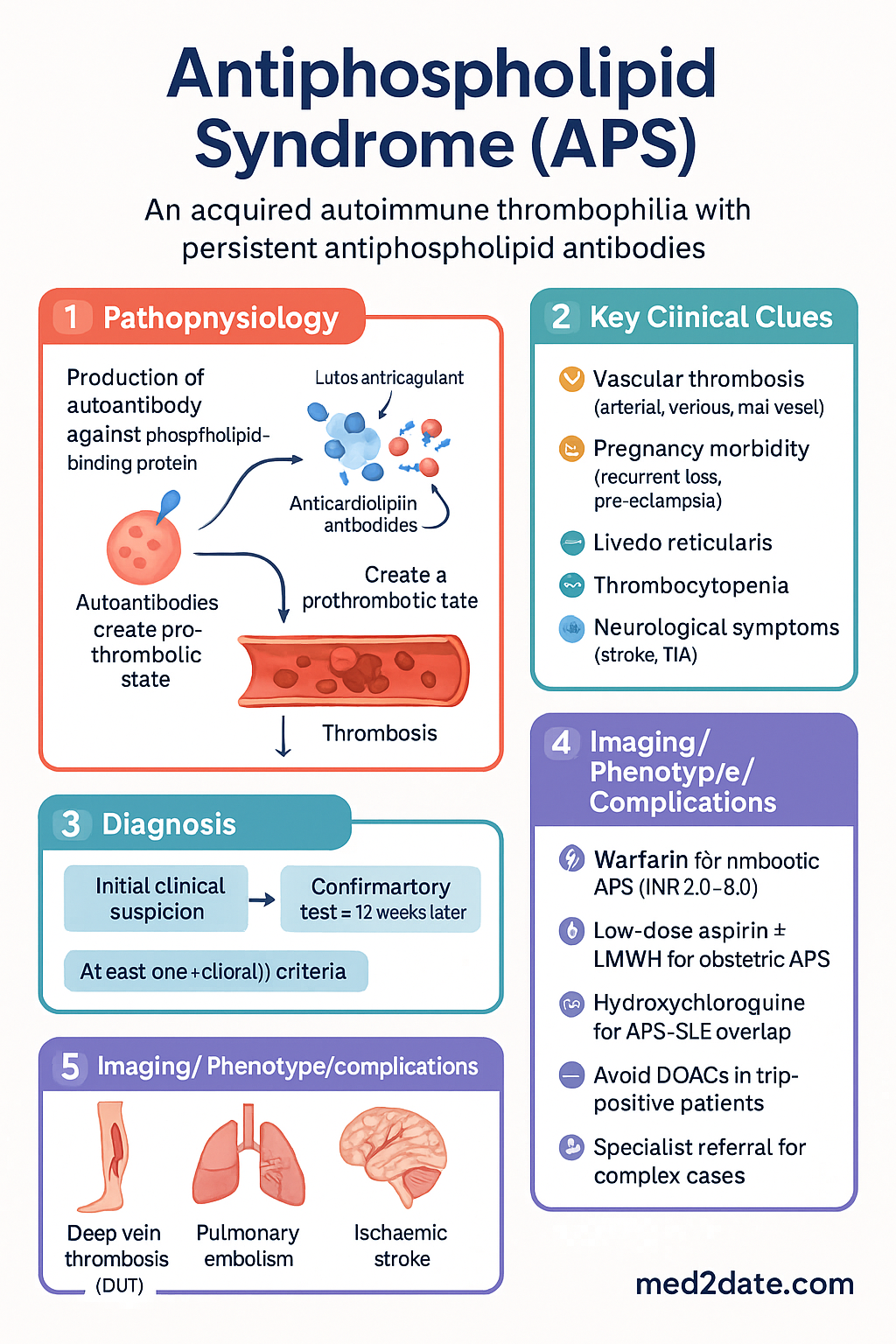
- Antiphospholipid syndrome (APS) is an acquired autoimmune thrombophilia with persistent antiphospholipid antibodies (aPL).
- The three main pathogenic antibodies are lupus anticoagulant (LA), anticardiolipin antibodies (aCL), and anti-β2-glycoprotein I antibodies (anti-B2GP1).
- Clinical hallmarks are vascular thrombosis (arterial, venous, small-vessel) and specific pregnancy morbidity.
- Diagnosis requires at least one clinical criterion and one laboratory criterion, with antibodies positive on two occasions ≥12 weeks apart (Sapporo/Sydney criteria).
- First-line long-term therapy for thrombotic APS is warfarin (target INR 2.0–3.0 for venous; may target 2.5–3.5 for arterial).
- Direct oral anticoagulants (DOACs) are generally inferior to warfarin in APS, especially in triple-positive patients, and are not recommended first-line.
- For obstetric APS, treatment is with low-dose aspirin (LDA) ± prophylactic LMWH, which significantly improves live birth rates.
- Hydroxychloroquine (HCQ) is a key immunomodulator, particularly in APS associated with SLE, and may reduce thrombotic risk.
- Catastrophic APS (CAPS) is a rare, life-threatening emergency requiring anticoagulation, high-dose corticosteroids, and often plasma exchange or IVIG.
- Aboriginal and Torres Strait Islander patients may have higher prevalence of autoimmune conditions and face barriers to specialist access and anticoagulation monitoring.
Introduction & Australian Epidemiology
Antiphospholipid syndrome (APS) is an acquired thrombophilia characterised by arterial or venous thrombosis and specific pregnancy complications, associated with persistent autoantibodies directed against phospholipid-binding proteins. It is a major cause of acquired thrombosis and recurrent pregnancy loss.
In Australia, APS affects an estimated 40–50 per 100,000 population. It is the most common acquired risk factor for venous thromboembolism (VTE) in younger patients (<50 years) and a significant cause of stroke in the absence of traditional vascular risk factors. The prevalence of antiphospholipid antibodies in the general population is about 1–5%, but only a subset develops clinical APS. It is more common in women, particularly obstetric APS, and has a strong association with systemic lupus erythematosus (SLE).
Pathogenesis & Antibodies
APS is driven by a heterogeneous group of autoantibodies targeting phospholipid-binding proteins. The pathogenesis involves a "two-hit" hypothesis: antibodies create a prothrombotic state, with a second trigger (e.g., surgery, infection, oestrogen) precipitating thrombosis.
Key Pathogenic Antibodies
- Lupus Anticoagulant (LA): An in vitro phenomenon prolonging phospholipid-dependent coagulation tests (e.g., dRVVT, APTT). Despite the name, it is strongly associated with in vivo thrombosis. It is considered the strongest risk marker for thrombosis and pregnancy complications.
- Anticardiolipin Antibodies (aCL): Detected by ELISA. IgG and IgM isotypes are considered. High titres (>40 GPL/MPL or >99th percentile) are clinically significant.
- Anti-β2-glycoprotein I Antibodies (anti-β2GPI): Detected by ELISA. Considered more specific for APS than aCL. IgG and IgM isotypes are relevant.
Clinical Features
Thrombosis
Thrombosis can be venous, arterial, or small-vessel, and may occur in any vascular bed.
- Venous: Deep vein thrombosis (DVT) and pulmonary embolism (PE) are most common. Unusual site thrombosis (e.g., cerebral venous sinus, hepatic, portal, renal veins) is a clue.
- Arterial: Ischaemic stroke and transient ischaemic attack (TIA) are the most frequent arterial events. Myocardial infarction, peripheral arterial occlusion, and retinal artery occlusion also occur.
- Small-vessel: Livedo reticularis/racemosa, renal thrombotic microangiopathy, adrenal haemorrhage.
Pregnancy Morbidity
APS is a treatable cause of recurrent pregnancy loss.
- ≥1 unexplained death of a morphologically normal foetus at or beyond 10 weeks' gestation.
- ≥1 premature birth before 34 weeks due to severe pre-eclampsia or placental insufficiency.
- ≥3 unexplained consecutive spontaneous abortions before 10 weeks.
Other Manifestations
- Cardiac: Libman-Sacks endocarditis, valvular thickening.
- Haematological: Thrombocytopenia, haemolytic anaemia.
- Neurological: Cognitive dysfunction, seizures, chorea.
- Catastrophic APS (CAPS): Rapid-onset multi-organ thrombosis with microangiopathy (3+ organs in <1 week). Mortality ~30–50%.
Sapporo Criteria & Investigations
Diagnosis is based on the 2006 Sydney revised Sapporo classification criteria. At least one clinical and one laboratory criterion must be met.
Clinical Criteria
- Vascular thrombosis: One or more episodes of arterial, venous, or small-vessel thrombosis in any tissue/organ, confirmed by objective validated criteria.
- Pregnancy morbidity: As detailed above.
Laboratory Criteria
Must be present on two or more occasions at least 12 weeks apart.
- Lupus anticoagulant (LA) present in plasma.
- Anticardiolipin antibody (aCL) of IgG and/or IgM isotype in serum or plasma, present in medium or high titre (>40 GPL/MPL or >99th percentile).
- Anti-β2-glycoprotein I antibody (anti-β2GPI) of IgG and/or IgM isotype in serum or plasma (in titre >99th percentile).
Key Investigations (Australian Context)
Management
Management is lifelong and tailored to clinical phenotype (thrombosis vs. obstetric), antibody profile, and underlying autoimmune disease (e.g., SLE).
Anticoagulation for Thrombotic APS
Antiplatelet & Immunomodulatory Therapy
Obstetric APS Management
Treatment is with prophylactic anticoagulation to improve placental perfusion.
- First-line: Low-dose aspirin (75–100 mg daily), commenced pre-conception or as soon as pregnancy is confirmed.
- Add Prophylactic LMWH (e.g., Enoxaparin 40 mg SC daily) once foetal heart activity is confirmed, continued to 6 weeks post-partum.
- Treatment-dose LMWH is used if there is a prior history of thrombosis.
Catastrophic APS (CAPS) Management
A medical emergency requiring intensive care unit admission.
- Immediate anticoagulation: IV unfractionated heparin (UFH) bolus then infusion.
- High-dose corticosteroids: IV methylprednisolone 500–1000 mg daily for 3 days.
- Plasma exchange (PLEX) or Intravenous Immunoglobulin (IVIG): Especially if thrombotic microangiopathy is present.
- Treat precipitating trigger (e.g., infection, surgery).
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
The burden of autoimmune disease and cardiovascular risk factors is higher in Aboriginal and Torres Strait Islander peoples, which may impact APS prevalence and outcomes. Consider APS in younger patients with unexplained thrombosis.
📚 References
- 1. Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost. 2006;4(2):295-306.
- 2. Cohen H, BJH, Efthymiou M, et al. British Society for Haematology Guidelines for the investigation and management of antiphospholipid syndrome. Br J Haematol. 2012;157(1):47-58.
- 3. Tektonidou MG, Andreoli L, Limper M, et al. EULAR recommendations for the management of antiphospholipid syndrome in adults. Ann Rheum Dis. 2019;78(10):1296-1304.
- 4. Pengo V, Denas G, Zoppellaro G, et al. Rivaroxaban vs warfarin in high-risk patients with antiphospholipid syndrome (TRAPS): a randomized trial. Blood. 2018;132(13):1365-1371.
- 5. Ordi-Ros J, Sáez-Comet L, Pérez-Conesa M, et al. Rivaroxaban versus vitamin K antagonist in antiphospholipid syndrome: a randomized noninferiority trial. Ann Intern Med. 2019;171(10):685-694.
- 6. Cervera R, Serrano R, Pons-Estel GJ, et al. Morbidity and mortality in the antiphospholipid syndrome during a 10-year period: a multicentre prospective study of 1000 patients. Ann Rheum Dis. 2015;74(6):1011-1018.
- 7. Royal Australian College of General Practitioners (RACGP). Management of Venous Thromboembolism in Primary Care. East Melbourne: RACGP; 2021.
- 8. Australian Commission on Safety and Quality in Health Care (ACSQHC). Blood Management Standard. Sydney: ACSQHC; 2022.
- 9. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework. Canberra: AIHW; 2023.
- 10. Cervera R, Rodríguez-Pintó I, Espinosa G. The diagnosis and clinical management of the catastrophic antiphospholipid syndrome: A comprehensive review. J Autoimmun. 2018;92:1-11.