📋 Key Information Summary
- The shoulder comprises four articulations — glenohumeral (GH), acromioclavicular (AC), sternoclavicular (SC), and scapulothoracic — all of which must be systematically assessed.
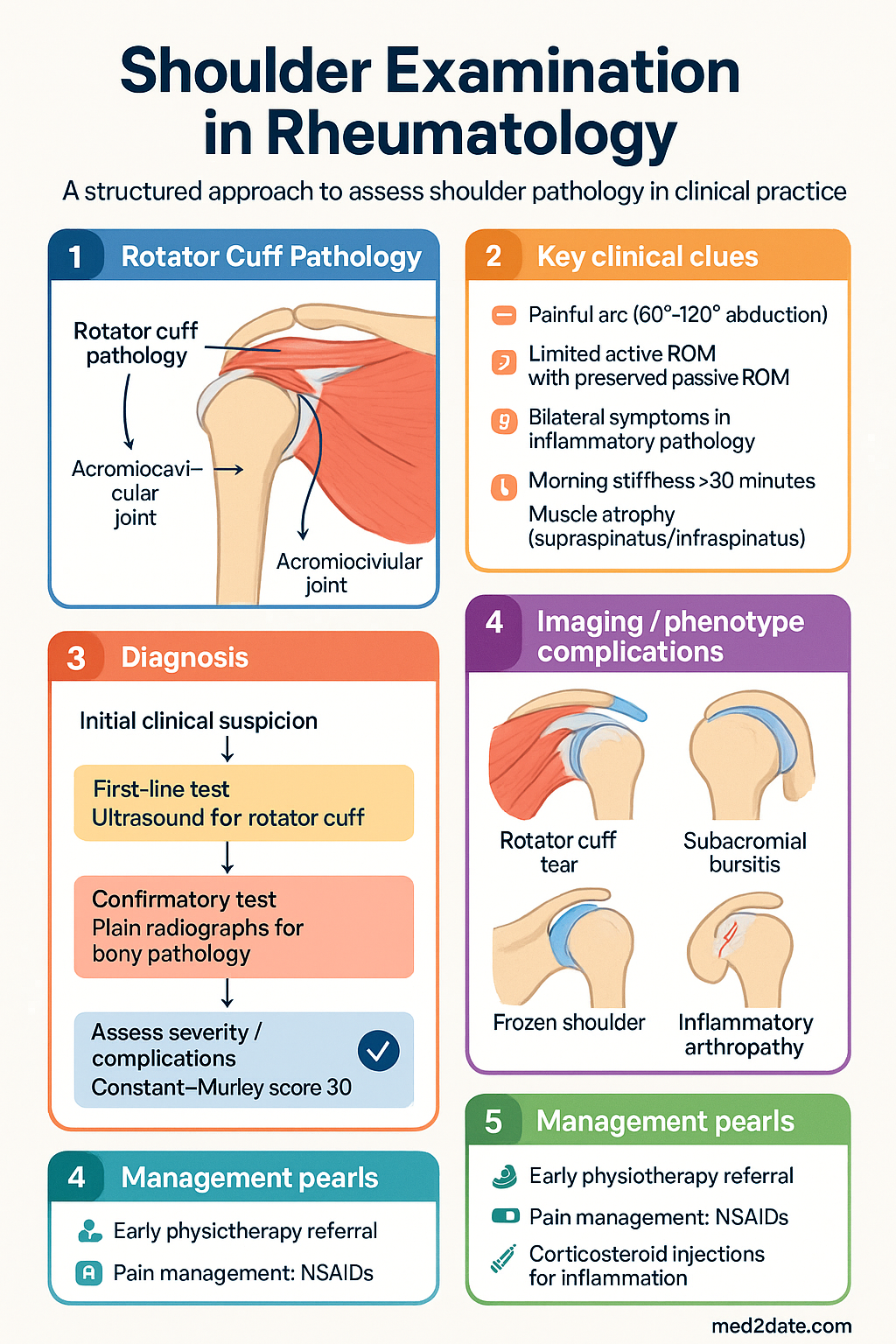
- Rotator cuff (SITS: supraspinatus, infraspinatus, teres minor, subscapularis) is the most common source of shoulder pathology in rheumatology practice.
- Use the Look–Feel–Move approach: inspect for asymmetry, swelling, and atrophy; palpate bony and soft-tissue landmarks; assess active then passive ROM.
- Normal glenohumeral ROM: flexion 180°, abduction 180°, external rotation 60–90°, internal rotation 60–90° (to T6–T12 spinous processes).
- Always compare active and passive ROM — preserved passive ROM with limited active ROM suggests a tendon/muscle pathology rather than joint contracture.
- The painful arc (pain between 60° and 120° of abduction) is a hallmark of subacromial pathology including rotator cuff tendinopathy and bursitis.
- Frozen shoulder (adhesive capsulitis) presents with global restriction of BOTH active and passive ROM in all planes — this distinguishes it from rotator cuff disease.
- Inflammatory shoulder pathology typically causes bilateral symptoms, morning stiffness >30 minutes, and systemic features — consider RA, PMR, and seronegative spondyloarthropathy.
- Key special tests: Neer and Hawkins-Kennedy (impingement), empty can/Jobe (supraspinatus), external rotation lag sign (infraspinatus), internal rotation lag sign (subscapularis), Speed's test (long head of biceps), O'Brien (SLAP / AC joint).
- The Constant–Murley score provides a validated patient-reported and clinician-assessed shoulder function score (0–100 points).
- Ultrasound is the first-line imaging for rotator cuff pathology; plain radiographs (AP, axillary lateral) assess bony pathology, calcific tendinitis, and OA.
- Aboriginal and Torres Strait Islander peoples experience higher rates of shoulder musculoskeletal disease with reduced access to specialist rheumatology and imaging services.
Introduction & Australian Epidemiology
A structured shoulder examination is essential for differentiating inflammatory, mechanical, and periarticular causes of shoulder pain in clinical rheumatology and musculoskeletal medicine practice. The shoulder is the third most common site of musculoskeletal consultation in Australian general practice, accounting for approximately 11% of all musculoskeletal presentations.
Shoulder complaints are responsible for significant functional impairment, lost work productivity, and reduced quality of life. In Australia, rotator cuff disease affects an estimated 20–30% of the adult population, with prevalence increasing with age — reaching 50–60% in those over 60 years. Frozen shoulder (adhesive capsulitis) has an estimated prevalence of 2–5%, with higher rates in people with diabetes mellitus, thyroid disease, and prolonged immobilisation.
The anatomical complexity of the shoulder — involving four discrete articulations and multiple periarticular structures — demands a systematic, structured examination approach. In rheumatology practice, distinguishing inflammatory arthropathy from degenerative or periarticular pathology is critical, as the investigation and management pathways diverge significantly. This guideline provides a practical framework for the clinical examination of the shoulder, with emphasis on Australian practice patterns, imaging availability, and validated scoring systems.
Anatomy & Functional Assessment
Articulations
The shoulder complex comprises four distinct articulations, each of which contributes to the overall range of motion and must be individually assessed during clinical examination:
| Joint | Type | Key Features | Examination Significance |
|---|---|---|---|
| Glenohumeral (GH) | Ball-and-socket synovial | Glenoid labrum provides socket depth; greatest ROM of any joint | Primary joint for ROM testing; intra-articular pathology (RA, OA, frozen shoulder) |
| Acromioclavicular (AC) | Plane synovial | Stabilised by AC ligament and coracoclavicular ligaments | Cross-body adduction test localises AC joint pathology |
| Sternoclavicular (SC) | Saddle synovial | Only axial articulation with the trunk; articular disc | Swelling may indicate septic arthritis, RA, or SAPHO syndrome |
| Scapulothoracic | Functional (non-synovial) | Serratus anterior, trapezius, rhomboids, levator scapulae stabilise | Winged scapula (long thoracic nerve palsy); scapular dyskinesis |
Rotator Cuff — SITS Muscles
The rotator cuff muscles form a musculotendinous cuff around the GH joint, providing dynamic stabilisation and enabling glenohumeral movement. The mnemonic SITS describes the four muscles:
| Muscle | Nerve | Primary Action | Clinical Test |
|---|---|---|---|
| Supraspinatus | Suprascapular (C5–C6) | Initiates abduction (first 15°) | Empty can / Jobe test |
| Infraspinatus | Suprascapular (C5–C6) | External rotation | External rotation lag sign |
| Teres minor | Axillary (C5–C6) | External rotation, adduction | Hornblower's sign |
| Subscapularis | Upper & lower subscapular (C5–C7) | Internal rotation | Internal rotation lag sign; Belly-press test; Lift-off test |
The Look–Feel–Move Approach
A systematic shoulder examination follows the structured Look–Feel–Move (Inspection–Palpation–Movement) framework, supplemented by special tests specific to the suspected pathology.
- Expose both shoulders; stand behind the patient
- Assess symmetry — compare side-to-side
- Muscle wasting: supraspinatus/infraspinatus atrophy (suprascapular neuropathy, massive rotator cuff tear), deltoid atrophy (axillary nerve palsy)
- Scapular winging (long thoracic nerve — serratus anterior)
- Visible swelling — anterior (GH joint effusion), superior (AC joint), SC joint
- Skin changes: erythema (septic arthritis, gout), psoriatic plaques, surgical scars
- Posture: rounded shoulders, forward head carriage
- AC joint — palpate along the clavicle to the acromion; tenderness localises AC pathology
- Bicipital groove — palpate in the bicipital groove (between greater and lesser tuberosities) anteriorly; tenderness suggests biceps tendinopathy
- Greater tuberosity — lateral aspect; tenderness over supraspinatus insertion
- Subacromial space — palpate through the deltoid; tenderness suggests bursitis
- GH joint line — palpate anteriorly through the rotator interval
- Suprascapular notch — posterior triangle; tenderness may indicate suprascapular nerve entrapment
- Temperature: increased warmth over inflamed joint (RA, septic arthritis)
- Always assess ACTIVE ROM first, then passive ROM — the discrepancy is diagnostic
- Compare with the contralateral (unaffected) shoulder
- Document range using a goniometer where possible
- Assess rhythm: scapulohumeral rhythm is normally 2:1 (GH : scapulothoracic contribution)
Normal Glenohumeral Range of Motion
| Movement | Normal ROM | Muscles Involved | Common Restriction Causes |
|---|---|---|---|
| Flexion | 180° | Anterior deltoid, supraspinatus | Frozen shoulder, GH arthritis, rotator cuff disease |
| Abduction | 180° | Deltoid, supraspinatus (initiates first 15°) | Supraspinatus tear, impingement, frozen shoulder |
| External rotation | 60–90° | Infraspinatus, teres minor | Frozen shoulder (early loss), subscapularis tear |
| Internal rotation | 60–90° | Subscapularis, pectoralis major, latissimus dorsi | Infraspinatus/supraspinatus pathology, adhesive capsulitis |
| Internal rotation (spinous process level) | T6–T12 | Subscapularis, teres major | Frozen shoulder, GH arthritis |
| Extension | 40–60° | Posterior deltoid, latissimus dorsi | Frozen shoulder, posterior capsule tightness |
Active vs Passive ROM — Diagnostic Significance
- Active = Passive (both restricted) → Joint pathology (frozen shoulder, GH arthritis, capsular contracture)
- Active < Passive (pain/weakness limiting active) → Muscle/tendon pathology (rotator cuff tendinopathy or tear)
- Active = Passive (both full) with pain → Bursitis, early impingement, or referred pain
The Painful Arc
The painful arc test is performed by asking the patient to actively abduct the arm from 0° to 180°. Pain occurring specifically between 60° and 120° of abduction is characteristic of subacromial pathology (rotator cuff tendinopathy, subacromial bursitis, or calcific tendinitis). Pain at the extremes of ROM (beginning and end range) more commonly suggests capsular pathology.
Special Tests
Special tests are provocative manoeuvres designed to stress specific anatomical structures to reproduce symptoms and localise pathology. Each test should be interpreted in the context of the overall clinical picture, not in isolation. The table below summarises the most clinically useful shoulder special tests in rheumatology practice.
Subacromial Impingement Tests
| Test | Technique | Positive Finding | Structures Assessed | Test Performance |
|---|---|---|---|---|
| Neer's Impingement | Stabilise scapula with one hand; passively flex the arm maximally with the other | Pain at maximal flexion | Supraspinatus tendon against coracoacromial arch | Sensitivity 75–89%, Specificity 31–48% |
| Hawkins–Kennedy | Arm at 90° forward flexion; passively internally rotate the shoulder | Pain on internal rotation | Rotator cuff tendons / bursa under coracoacromial ligament | Sensitivity 72–92%, Specificity 25–66% |
Rotator Cuff Integrity Tests
| Test | Technique | Positive Finding | Structures Assessed | Test Performance |
|---|---|---|---|---|
| Empty Can / Jobe Test | Arm at 90° abduction, 30° forward flexion, thumb pointing down (pronated); resist downward pressure | Pain and/or weakness against resistance | Supraspinatus tendon | Sensitivity 41–91%, Specificity 50–90% |
| External Rotation Lag Sign | Passively position arm at 20° abduction with 90° external rotation; ask patient to hold; release | Arm drops/rotates internally (loss of ER position) | Infraspinatus / teres minor (massive tear) | Specificity ~90%+ for full-thickness infraspinatus tear |
| Internal Rotation Lag Sign | Passively position arm at maximum internal rotation (hand behind back); ask patient to hold; release | Hand drops / cannot maintain position | Subscapularis | Specificity ~90%+ for subscapularis tear |
| Belly-Press Test | Patient presses hand firmly against abdomen with elbow anterior to the trunk | Unable to maintain pressure; elbow drops posteriorly or compensatory wrist flexion | Subscapularis (upper portion) | Sensitivity 40–80%, Specificity 60–90% |
| Lift-Off Test (Gerber) | Hand placed behind the back (lumbar region); ask patient to lift hand off back | Unable to lift hand away from back | Subscapularis (lower portion) | Specificity ~85%+ but cannot be performed if ROM restricted |
| Hornblower's Sign | Arm at 90° abduction, elbow at 90° flexion; ask patient to externally rotate against resistance | Unable to maintain external rotation position | Teres minor | Specificity ~93% for teres minor pathology |
Biceps Tendon Tests
| Test | Technique | Positive Finding | Structures Assessed |
|---|---|---|---|
| Speed's Test | Arm at 90° forward flexion, elbow extended, supinated forearm; resist downward force | Pain in bicipital groove | Long head of biceps (bicipital tendinopathy) |
| Yergason's Test | Elbow flexed to 90°, forearm pronated; resist supination while stabilising bicipital groove | Pain and/or subluxation in bicipital groove | Biceps tendon / transverse humeral ligament |
Instability Tests
| Test | Technique | Positive Finding | Structures Assessed |
|---|---|---|---|
| Apprehension Test | Arm at 90° abduction; slowly externally rotate | Patient becomes apprehensive / resists further ER; sense of impending dislocation | Anterior GH instability |
| Relocation Test | Follows apprehension test: apply posterior force to humeral head while at maximal ER | Apprehension resolves; further ER possible | Confirms anterior instability (Bankart lesion) |
AC Joint and Labral Tests
| Test | Technique | Positive Finding | Structures Assessed |
|---|---|---|---|
| O'Brien's Test (Active Compression) | Arm at 90° flexion, 10–15° adduction; first with thumb down (pronated), then thumb up (supinated); resist downward force in both positions | Pain with thumb down > thumb up; pain localised superiorly = AC joint; pain/deep click = labral (SLAP) | AC joint pathology / SLAP lesion (superior labral tear) |
| Cross-Body Adduction | Passively adduct the arm across the body at 90° flexion | Pain localised to AC joint | AC joint OA, distal clavicle osteolysis |
Scapular Assessment
Scapular dyskinesis (abnormal scapular motion) contributes to shoulder pathology and should be assessed during active arm elevation:
- Observe scapulohumeral rhythm from behind during arm elevation — should be 2:1 ratio
- Lateral scapular slide test: measure distance from inferior angle to spinous process at 0°, 45° abduction, and 90° abduction; asymmetry >1.5 cm suggests scapular dyskinesis
- Winged scapula: ask patient to push against a wall; medial winging = long thoracic nerve palsy (serratus anterior); lateral winging = spinal accessory nerve palsy (trapezius)
Clinical Patterns — Diagnostic Algorithms
The constellation of examination findings — rather than any single test — determines the clinical diagnosis. The following clinical patterns represent the most common diagnostic scenarios encountered in rheumatology practice.
Pattern Recognition Table
| Clinical Pattern | Active ROM | Passive ROM | Pain Pattern | Strength | Key Distinguishing Features |
|---|---|---|---|---|---|
| Frozen Shoulder | ↓↓ Globally restricted | ↓↓ Globally restricted | Diffuse, aching; night pain | Cannot assess (limited by ROM) | Loss of external rotation is the hallmark; capsular pattern (ER > abduction > IR); 3 phases (painful → stiff → thawing) |
| Rotator Cuff Tendinopathy / Tear | ↓ Painful arc | Normal or near-normal | 60–120° abduction (painful arc) | ↓ Resisted weakness (muscle-specific) | Active < Passive = tendon pathology; positive Jobe / ER lag / IR lag |
| Subacromial Bursitis | ↓ Painful arc | Near normal | 60–120° abduction; pain on IR in abduction | Normal (no weakness) | Painful arc + no weakness = bursitis; resisted tests may be painful but not weak |
| Inflammatory Arthropathy (RA, PMR) | ↓ Bilateral | ↓ Bilateral | Bilateral, diffuse; morning stiffness >30 min | May be reduced | Bilateral + morning stiffness + systemic features (fatigue, weight loss); synovial thickening on palpation; consider PMR if age >50 with bilateral shoulder girdle pain |
| Calcific Tendinitis | ↓ Acute pain | ↓ (pain limits) | Acute, severe; night pain; may mimic septic arthritis | Cannot test (pain) | Sudden acute onset; radiographic calcification in supraspinatus; self-limiting (resorptive phase) |
| GH Osteoarthritis | ↓ Gradual | ↓ | Deep, aching; worse with activity | May be reduced | Age >60; crepitus; capsular pattern; X-ray shows joint space narrowing, osteophytes, sclerosis |
Frozen Shoulder — The Hallmark of Global Restriction
Three phases of frozen shoulder:
Rotator Cuff Pathology — The Painful Arc + Weakness Pattern
Rotator cuff disease represents a spectrum from tendinopathy to partial-thickness tears to full-thickness tears. The examination pattern is:
- Painful arc (60–120° abduction) — present in tendinopathy and tears
- Resisted weakness — specific to the involved tendon (Jobe for supraspinatus, ER for infraspinatus, IR for subscapularis)
- Passive ROM preserved — this is the critical differentiator from frozen shoulder
- Lag signs — indicate full-thickness tears (high specificity)
Bursitis vs Tendinopathy
Subacromial bursitis and rotator cuff tendinopathy frequently coexist but can be distinguished clinically:
- Bursitis alone: Painful arc, pain on Neer/Hawkins, but no weakness on resisted testing
- Tendinopathy: Painful arc plus weakness on resisted testing of the specific tendon
- Bursitis: Pain with passive internal rotation of the abducted arm (Hawkins–Kennedy positive)
- Both improve with subacromial injection of local anaesthetic ± corticosteroid (diagnostic injection)
Inflammatory Shoulder — Red Flags for Systemic Disease
- Bilateral shoulder pain and stiffness
- Morning stiffness >30 minutes
- Systemic features: fatigue, weight loss, low-grade fever, night sweats
- Joint swelling / synovial thickening on palpation
- Age >50 with bilateral shoulder girdle + hip girdle pain → consider polymyalgia rheumatica (PMR)
- Symmetrical small joint involvement → consider rheumatoid arthritis
- Order: FBC, ESR, CRP, RF, anti-CCP antibodies, ANA; consider ultrasound for subdeltoid bursitis / GH synovitis
Constant–Murley Shoulder Score
The Constant–Murley score is the most widely used validated outcome measure for shoulder function. It provides a composite score (0–100 points) incorporating subjective and objective components:
| Domain | Components | Max Score | Assessment Method |
|---|---|---|---|
| Pain | Severity of pain (subjective) | 15 points | Visual analogue scale (0 = severe pain, 15 = no pain) |
| Activities of Daily Living | Work, recreation, sleep position | 20 points | Patient-reported questionnaire |
| Range of Motion | Flexion, abduction, ER, IR | 40 points | Clinician-assessed with goniometer |
| Strength | Isometric abduction strength | 25 points | Measured with spring balance or dynamometer at 90° abduction |
Interpretation: 90–100 = excellent; 80–89 = good; 70–79 = fair; <70 = poor. Age- and sex-adjusted normal values are available. The Constant–Murley score is used for monitoring treatment outcomes in rotator cuff repair, arthroplasty, and frozen shoulder management. It is less useful in acute settings where pain limits full testing.
Investigations & Imaging
Clinical examination guides investigation selection. Imaging should be directed by the working diagnosis derived from examination findings, not used as a screening tool for all shoulder pain.
Laboratory Investigations
Imaging
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Lewis J. Rotator cuff related shoulder pain: assessment, management and uncertainties. Manual Therapy. 2016;23:57–68.
- 2. Hanchard NC, Lenza M, Handoll HH, Takwoingi Y. Physical tests for shoulder impingements and local lesions of bursa, tendon or labrum that may accompany impingement. Cochrane Database of Systematic Reviews. 2013;(4):CD007427.
- 3. Hegedus EJ, Goode A, Campbell S, et al. Physical examination tests of the shoulder: a systematic review with meta-analysis of individual tests. British Journal of Sports Medicine. 2008;42(2):80–92.
- 4. Zuckerman JD, Rokito A. Frozen shoulder: a consensus definition. Journal of Shoulder and Elbow Surgery. 2011;20(2):322–325.
- 5. Constant CR, Murley AH. A clinical method of functional assessment of the shoulder. Clinical Orthopaedics and Related Research. 1987;(214):160–164.
- 6. Laslett M, Steele M, Hing W, McNair P, Cadogan A. Shoulder pain patients in primary care — part 2: predictors of outcome in patients with shoulder pain. Manual Therapy. 2014;19(6):602–611.
- 7. Hopewell S, Keene DJ, Maia Schlüssel M, et al. Clinical and ultrasound features of rotator cuff disease: a systematic review. Annals of the Rheumatic Diseases. 2018;77(suppl 2):A48.
- 8. Australian Institute of Health and Welfare (AIHW). Musculoskeletal conditions in Aboriginal and Torres Strait Islander people. Canberra: AIHW; 2023.
- 9. Royal Australian College of General Practitioners (RACGP). Musculoskeletal guidelines for primary care. Melbourne: RACGP; 2022.
- 10. Buchbinder R, Green S, Youd JM. Corticosteroid injections for shoulder pain. Cochrane Database of Systematic Reviews. 2003;(1):CD004016.
- 11. Downie BK, Miller BS, Bhatt S, et al. Physical examination and imaging of shoulder impingement. Current Reviews in Musculoskeletal Medicine. 2008;1(2):136–143.
- 12. Tibone JE, Jobe FW, Kerlan RK, et al. Shoulder impingement syndrome in athletes treated by an anterior acromioplasty. Clinical Orthopaedics and Related Research. 1985;(198):134–140.
- 13. Australian Orthopaedic Association (AOA). National Joint Replacement Registry — Shoulder Arthroplasty Annual Report. Adelaide: AOA; 2023.