📋 Key Information Summary
- Osteoarthritis (OA) is the most common joint disease in Australia, affecting over 2.1 million Australians and the leading cause of chronic musculoskeletal pain and disability.
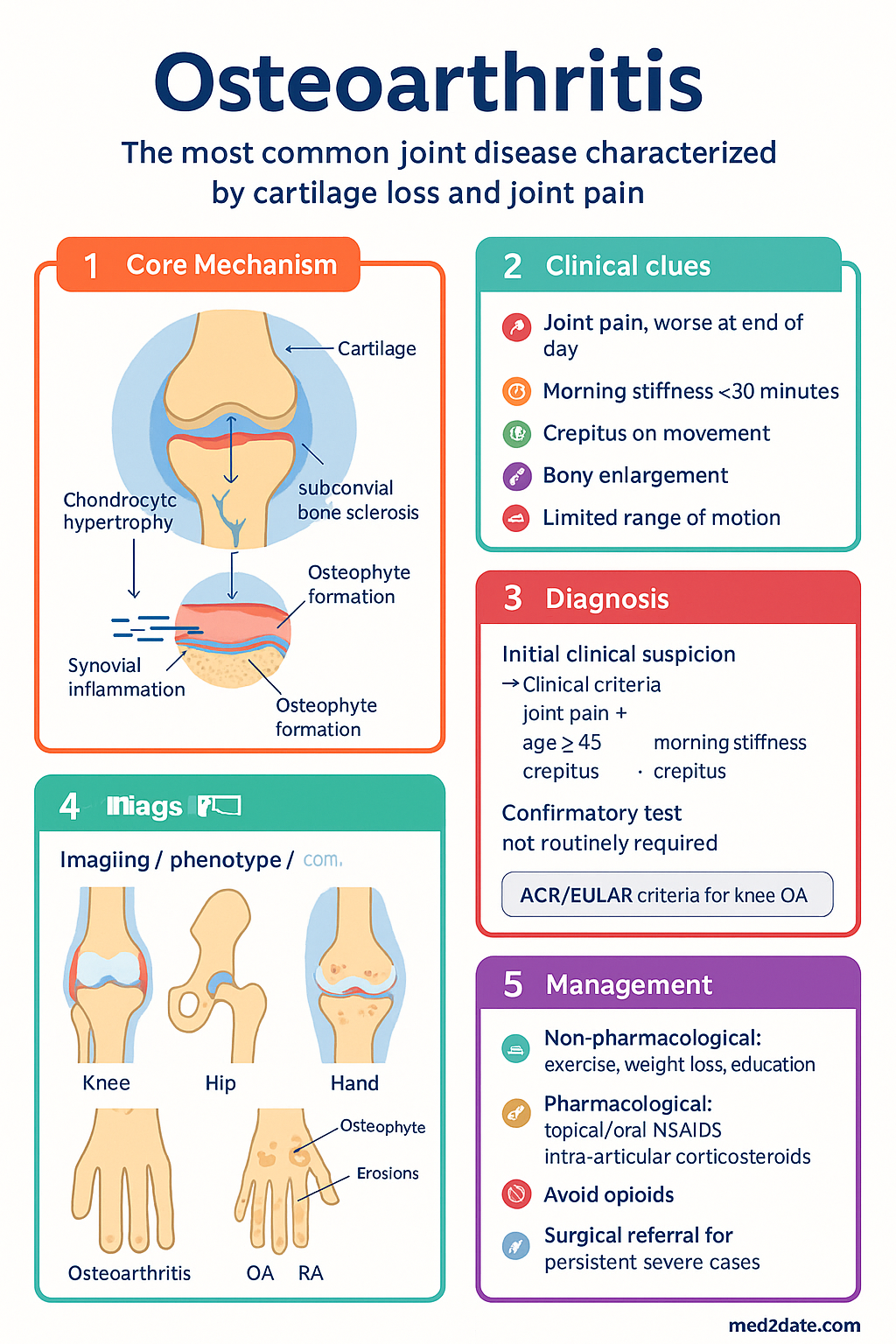
- Diagnosis is primarily clinical — joint pain plus ≥2 of: age ≥45 years, morning stiffness <30 minutes, crepitus, bony enlargement. X-ray is not required for diagnosis in typical presentations.
- First-line management is non-pharmacological: structured land-based exercise, weight loss (if BMI >25), education, and self-management — these are more effective long-term than analgesics alone.
- Pharmacological management follows a stepwise approach: oral paracetamol (limited efficacy), topical NSAIDs (knee/hand), oral NSAIDs with PPI cover, and intra-articular corticosteroid injection for flares.
- Opioids have NO role in chronic OA management — RACGP and ARA strongly recommend against initiation. Consider only in patients who are unsuitable for surgery or other therapies, and only short-term.
- Glucosamine, chondroitin, and collagen supplements are NOT recommended — no consistent evidence of benefit; discontinue if no improvement within 12 weeks.
- Knee OA: strong evidence for quadriceps strengthening, aerobic exercise, and weight loss. Hiking poles and braces may assist function. Intra-articular hyaluronic acid is NOT recommended by ARA.
- Hip OA: hip-specific strengthening, aquatic exercise, and weight loss are first-line. Fewer evidence-based supports than knee OA — surgical referral threshold is lower.
- Hand OA: topical NSAIDs preferred over oral; thumb-base (1st CMC) splints provide strong evidence of benefit. Intra-articular injections are less established for hand joints.
- Surgical referral (arthroplasty) is indicated when there is structural disease on imaging, persistent moderate-to-severe pain and functional limitation despite ≥3 months of optimised non-surgical and pharmacological therapy.
- Aboriginal and Torres Strait Islander peoples experience higher OA prevalence, earlier onset, and greater disability — culturally safe, community-based exercise programmes improve engagement and outcomes.
- All patients should receive a written OA management plan; allied health referrals (physiotherapy, exercise physiology, dietetics) are MBS-rebated under GP Management Plans (GPMP) and Team Care Arrangements (TCA).
Introduction & Australian Epidemiology
Osteoarthritis is a progressive, degenerative joint disease characterised by cartilage loss, subchondral bone remodelling, osteophyte formation, synovial inflammation, and periarticular muscle weakness. It is the most prevalent form of arthritis worldwide and the single largest cause of musculoskeletal disability in Australia.
The 2022 AIHW report estimates that over 2.1 million Australians (approximately 8.3% of the population) live with OA, with prevalence rising sharply after age 45 years. By age 75, over 50% of Australians demonstrate radiographic knee OA. OA is the most common reason for total knee and hip arthroplasty in Australia, with over 80,000 procedures performed annually.
Key Australian statistics:
- OA is the 12th leading cause of total disease burden (DALYs) in Australia and the leading cause among musculoskeletal conditions.
- Women are disproportionately affected, particularly after menopause, with a female-to-male ratio of approximately 1.5:1 for knee OA and 2:1 for hand OA.
- Obesity (BMI ≥30 kg/m²) is the strongest modifiable risk factor — each 5 kg/m² increase in BMI increases knee OA risk by 35%.
- Aboriginal and Torres Strait Islander peoples experience a 1.4-fold higher age-standardised prevalence and develop OA approximately 10 years earlier on average.
- OA costs the Australian health system an estimated $3.5 billion per year, including direct healthcare costs and lost productivity.
- Common joint sites in descending order of prevalence: knee (most common symptomatic site), hand (DIP, PIP, 1st CMC), hip, spine (facet joints).
Pathophysiology
OA was historically considered a "wear-and-tear" disease of cartilage but is now understood as a whole-organ disease involving dynamic, progressive loss of articular cartilage with concurrent changes in all periarticular tissues.
Key Pathological Processes
- Cartilage degradation: Chondrocyte hypertrophy and apoptosis lead to increased matrix metalloproteinase (MMP) activity, collagen breakdown, proteoglycan loss, and progressive cartilage thinning.
- Subchondral bone: Sclerosis, cyst formation, and increased vascularity — subchondral bone stiffening redistributes load, accelerating cartilage damage.
- Synovial inflammation: Low-grade chronic synovitis with macrophage and lymphocyte infiltration; releases inflammatory cytokines (IL-1β, TNF-α, IL-6) that further drive cartilage catabolism.
- Osteophytes: Bony outgrowths at joint margins driven by TGF-β and BMP signalling — represent attempted repair but contribute to pain, stiffness, and deformity.
- Periarticular structures: Tendon and ligament degeneration, periarticular muscle weakness (especially quadriceps in knee OA), and neurovascular ingrowth into subchondral bone and menisci contribute to pain sensitisation.
Pain Mechanisms
Joint pain in OA is multifactorial and not purely structural. Nociceptive, inflammatory, and neuropathic mechanisms all contribute. Central sensitisation (widespread pain, allodynia) develops in approximately 20–30% of patients with chronic knee OA, which may explain the disconnect between radiographic severity and symptoms.
Risk Factors
| Modifiable | Non-Modifiable |
|---|---|
| Obesity / overweight | Age (≥45 years) |
| Joint injury / previous surgery | Female sex |
| Occupational overuse | Genetic predisposition |
| Muscle weakness | Congenital joint abnormalities (e.g. DDH, SCFE) |
| Physical inactivity | Ethnicity (higher prevalence in ATSI, Māori) |
| Malalignment (varus/valgus) | Menopause (loss of oestrogen protection) |
Clinical Presentation & Diagnostic Criteria
OA should be diagnosed clinically in primary care without routine imaging. The American College of Rheumatology (ACR) / European Alliance of Associations for Rheumatology (EULAR) classification criteria support diagnosis based on history and examination.
Core Clinical Features
- Activity-related joint pain, typically worse at end of day or with prolonged use
- Short-lived morning stiffness (<30 minutes) that improves with gentle movement
- Crepitus on passive movement
- Bony enlargement (osteophytes)
- Limited range of motion
- Joint instability / giving way (particularly knee)
- Functional limitation — difficulty with stairs, rising from seated, gripping
When to Order Imaging
Red Flags Requiring Urgent Investigation
- Acute hot, swollen joint — exclude septic arthritis, gout, CPPD
- Night pain unrelieved by rest or analgesia
- Systemic symptoms (fever, weight loss, night sweats)
- Rapidly progressive joint destruction
- Suspected malignancy or pathological fracture
Knee Osteoarthritis
Knee OA is the most common site of symptomatic OA in Australia, affecting approximately 1 in 11 adults over 45 years. The medial tibiofemoral compartment is most frequently involved, followed by the patellofemoral joint.
Clinical Assessment
- Inspect for varus (medial OA) or valgus (lateral OA) malalignment
- Assess for effusion (bulge test, patellar ballottement)
- Quadriceps strength (sit-to-stand test)
- Patellofemoral crepitus and pain on resisted knee extension
- Assess gait — antalgic pattern, Trendelenburg sign
- Functional measures: 30-second sit-to-stand, timed up-and-go, WOMAC score
ACR/EULAR Clinical Classification Criteria (Knee OA)
Sensitivity 92%, Specificity 75%. Knee pain plus ≥3 of:
- Age ≥50 years
- Morning stiffness ≤30 minutes
- Crepitus
- Bony tenderness
- Bony enlargement
- No palpable warmth
Knee-Specific Management
- Exercise: Strong evidence for quadriceps strengthening (supervised progressive resistance), aerobic walking programmes (150 min/week), and tai chi. Physiotherapy referral is first-line.
- Weight loss: ≥5–10% body weight reduction reduces knee pain by 50% and slows structural progression. Combine diet + exercise for best outcomes.
- Bracing: Valgus unloader braces for medial compartment OA may reduce pain and improve function in select patients. Simple neoprene sleeves provide proprioceptive benefit.
- Taping: Patellar taping (McConnell technique) for patellofemoral component.
- Walking aids: Hiking poles reduce knee joint loading by 10–15%. Single-point cane in contralateral hand.
- Footwear: Shock-absorbing, flat-soled shoes. Avoid high heels. Lateral wedge insoles are NOT recommended (ARA 2024).
Hip Osteoarthritis
Hip OA is the second most common site of symptomatic OA. It tends to present later than knee OA (typically age >55) and has a faster trajectory to arthroplasty. Superolateral femoral head migration on X-ray indicates worse prognosis.
Clinical Assessment
- Pain in groin, anterior thigh, or buttock (not lateral hip — consider trochanteric bursitis)
- "C-sign" — patient cups hand over lateral hip indicating deep joint pain
- Loss of internal rotation (earliest and most sensitive sign)
- Positive FADIR (flexion-adduction-internal rotation) test
- Antalgic gait with shortened stance phase and Trendelenburg lurch
- Leg length discrepancy from superior migration
Hip-Specific Management
- Exercise: Hip-specific strengthening (gluteal, abductor), aquatic exercise, and walking programmes. Supervised physiotherapy is recommended.
- Weight loss: Similar importance to knee OA — even modest reductions improve symptoms.
- Walking aids: Contralateral cane reduces hip joint reaction force by up to 30%.
- Pharmacological: Same stepwise approach as for other sites. Intra-articular injection requires ultrasound or fluoroscopic guidance for accuracy.
- Surgical threshold: Lower than for knee OA — consider referral when pain and functional limitation are moderate despite conservative therapy. Total hip arthroplasty has excellent long-term outcomes (15–20 year survival >90%).
Hand OA & 1st CMC Joint
Hand OA is the most common form of OA in women over 50 and carries significant disability for fine motor tasks, grip, and daily function. The 1st carpometacarpal (CMC / trapeziometacarpal) joint is the second most commonly affected site after the distal interphalangeal (DIP) joints.
Clinical Features by Joint Site
| Joint Site | Features | Eponymous Sign |
|---|---|---|
| DIP joints | Bony nodules (Heberden's nodes), lateral deviation | Heberden's nodes |
| PIP joints | Bony nodules, swan-neck or boutonnière deformity | Bouchard's nodes |
| 1st CMC (thumb base) | Pain with pinch/grip, "squaring" of the thumb base, positive grind test | — |
| MCP joints | Less common — if involved, consider haemochromatosis | — |
1st CMC Joint — Specific Management
- Splinting: Rigid or semi-rigid thumb spica splint provides strong evidence of pain relief and functional improvement. Wear during aggravating activities (opening jars, wringing).
- Topical NSAIDs: First-line pharmacotherapy for hand OA — topical diclofenac 1% gel or 2.3% patch applied to affected joints.
- Hand therapy: Occupational therapist-led programmes including joint protection education, adaptive equipment, and grip-strengthening exercises.
- Intra-articular injections: Less established than for knee; consider corticosteroid injection for flares. Ultrasound-guided injection for 1st CMC improves accuracy.
- Surgical: Trapeziectomy (± ligament reconstruction and tendon interposition) is the most common surgical procedure for refractory 1st CMC OA with good outcomes.
Investigations
OA is a clinical diagnosis. Investigations serve to exclude alternative diagnoses or complications rather than to confirm OA.

Risk Stratification & Severity Scoring
Severity is best determined by clinical features and functional impact rather than imaging alone. The WOMAC (Western Ontario and McMaster Universities) index and KOOS (Knee Injury and Osteoarthritis Outcome Score) are validated patient-reported outcome measures (PROMs).
Functional Assessment Tools
- WOMAC: 24-item questionnaire covering pain, stiffness, and function. Score 0–96. Useful for tracking change.
- KOOS: 42-item knee-specific score. Covers pain, symptoms, function, sport, quality of life.
- HOOS: Hip equivalent of KOOS.
- 30-second sit-to-stand: Quick functional measure — fewer than 12 stands indicates increased fall risk.
- 6-minute walk test: Assesses functional walking capacity. <350 m suggests significant limitation.
Pharmacological Pain Management
Pharmacotherapy is adjunctive to non-pharmacological strategies. All oral analgesics for OA have modest effect sizes. The goal is pain control to enable engagement with exercise and self-management.
Stepwise Approach
Drug Cards
Medications NOT Recommended
- Opioids: RACGP, ARA, and international guidelines recommend AGAINST use in chronic OA. Harms (falls, fractures, dependence, respiratory depression) outweigh any modest benefit. Exception: short-term perioperative use or as a trial in patients unsuitable for surgery.
- Glucosamine / chondroitin: No consistent evidence of structural modification or clinically meaningful pain relief. Discontinue if no benefit within 12 weeks. Not PBS-listed.
- Intra-articular hyaluronic acid (viscosupplementation): ARA does not recommend — meta-analyses show minimal clinical benefit. Not PBS-listed. OOP cost $300–800 per injection.
- Duloxetine: Limited Australian data for OA. May have a role if central sensitisation / neuropathic component suspected. Off-label use — discuss with rheumatologist.
- Collagen supplements, CBD oil, PRP: Insufficient evidence. PRP is not MBS-rebated and is not recommended by ARA for routine OA management.
Exercise & Non-Pharmacological Therapy
Non-pharmacological management is the cornerstone of OA care. The 2019 EULAR recommendations and ARA 2024 guidelines prioritise education, exercise, and weight loss as first-line therapy for ALL patients with OA.
Core Components
- Land-based exercise — strongest evidence (NNT 4–6 for pain relief)
- Quadriceps / hip abductor progressive resistance training
- Aerobic exercise: walking, cycling, swimming (≥150 min/week)
- Aquatic exercise — particularly useful for obesity, frailty, or severe pain
- Tai chi and yoga — moderate evidence for knee OA
- Neuromuscular training / balance for fall prevention
- Supervised programmes (physiotherapy, exercise physiology) superior to unsupervised
- Target ≥5% body weight loss if BMI ≥25 kg/m²
- 10% loss provides additional benefit for knee OA
- Combine dietary modification + exercise for sustained results
- Referral to accredited practising dietitian (APD) via GPMP/TCA
- Bariatric surgery may be considered for BMI ≥40 with refractory knee OA
- Mediterranean-style diet associated with reduced inflammation
Education & Self-Management
- OA is NOT an inevitable consequence of ageing — patients should understand disease is manageable
- Written OA management plan — provide at every consultation
- Self-management programmes (e.g. Arthritis Australia, Pain Management Programme)
- Cognitive behavioural strategies for chronic pain
- Activity pacing to manage pain fluctuations
Allied Health Referrals — MBS Access
| Provider | Role | MBS Access |
|---|---|---|
| Physiotherapist | Exercise prescription, gait training, braces, taping | GPMP/TCA — 5 subsidised visits/year |
| Exercise physiologist | Structured exercise programmes, long-term maintenance | GPMP/TCA — 5 subsidised visits/year |
| Accredited practising dietitian | Weight management, dietary counselling | GPMP/TCA — 5 subsidised visits/year |
| Occupational therapist | Joint protection, splints (hand/CMC), adaptive equipment | GPMP/TCA — 5 subsidised visits/year |
| Psychologist | CBT for chronic pain, mood management, self-efficacy | Mental Health Treatment Plan — 6 subsidised visits/year (initial) + 4 (review) |
Surgical Referral
Total joint arthroplasty (TJA) is the definitive treatment for end-stage OA when conservative management has failed. In Australia, over 80,000 total knee arthroplasties (TKA) and 50,000 total hip arthroplasties (THA) are performed annually.
Indications for Referral to Orthopaedic Surgery
- Persistent moderate-to-severe pain and functional limitation despite ≥3 months of optimised non-surgical therapy (exercise, weight loss, pharmacotherapy)
- Structural disease on X-ray (KL grade 3–4)
- Reduced quality of life — inability to perform ADLs, walking <500 m, night pain disturbing sleep
- Patient preference after informed discussion of risks and benefits
Before Referral — Checklist
- Has the patient completed ≥3 months of supervised exercise therapy?
- Has weight loss been addressed? BMI >40 is a relative contraindication to arthroplasty.
- Have pharmacological options been optimised (topical NSAIDs, oral NSAIDs, injections)?
- Has the patient been counselled on realistic expectations (rehabilitation duration, return to function)?
- Are comorbidities optimised for anaesthesia (diabetes, cardiac, respiratory)?
- Is smoking cessation addressed? Smoking increases infection and revision rates.
Surgical Options
| Procedure | Indication | Expected Outcome |
|---|---|---|
| Total Knee Arthroplasty (TKA) | End-stage tricompartmental knee OA | 95% patient satisfaction. 15–20 yr implant survival >90% |
| Total Hip Arthroplasty (THA) | End-stage hip OA | 95% patient satisfaction. 15–20 yr implant survival >90%. Faster recovery than TKA |
| Unicompartmental Knee Arthroplasty | Isolated medial or lateral compartment OA with intact ACL | Faster recovery, better ROM. Higher revision rate than TKA at 10 yr |
| Trapeziectomy ± LRTI | Refractory 1st CMC OA | Good pain relief. Grip strength may be reduced. Functional improvement at 6–12 months |
| Arthroscopic debridement | NOT recommended for OA (ARA 2024) | No benefit over placebo surgery. AVOID. |
Perioperative Considerations
- Prehabilitation (exercise before surgery) improves post-operative recovery
- NSAIDs should be ceased 1 week before surgery
- DOACs/anticoagulants — coordinate with surgical team for timing
- VTE prophylaxis with LMWH or DOAC post-operatively (per local protocol)
- Early mobilisation and intensive rehabilitation are essential
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a 1.4-fold higher age-standardised prevalence of OA compared with non-Indigenous Australians, with onset approximately 10 years earlier. OA is one of the leading contributors to the health gap in musculoskeletal burden and disability.
📚 References
- 1. Australian Institute of Health and Welfare (AIHW). Osteoarthritis. Cat. no. PHE 254. Canberra: AIHW; 2023.
- 2. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2020;72(2):149–162.
- 3. Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1578–1589.
- 4. Musculoskeletal Australia. The State of Musculoskeletal Health in Australia 2023. Melbourne: Musculoskeletal Australia; 2023.
- 5. Bennell KL, Hinman RS. A review of the clinical evidence for exercise in osteoarthritis of the hip and knee. J Sci Med Sport. 2011;14(1):4–9.
- 6. Messier SP, Mihalko SL, Legault C, et al. Effects of intensive diet and exercise on knee joint loads, inflammation, and clinical outcomes among overweight and obese adults with knee osteoarthritis: the IDEA randomized clinical trial. JAMA. 2013;310(12):1263–1273.
- 7. Fransen M, McConnell S, Harmer AR, et al. Exercise for osteoarthritis of the knee. Cochrane Database Syst Rev. 2015;(1):CD004376.
- 8. Arthritis Australia. Position Statement: Opioids for Osteoarthritis. Sydney: Arthritis Australia; 2022.
- 9. da Costa BR, Nüesch E, Kasteler R, et al. Oral or transdermal opioids for osteoarthritis of the knee or hip. Cochrane Database Syst Rev. 2014;(9):CD003115.
- 10. Kirkley A, Birmingham TB, Litchfield RB, et al. A randomized trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2008;359(11):1097–1107.
- 11. Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice. 10th ed. East Melbourne: RACGP; 2024.
- 12. Dziedzic KS, Healey EL, Porcheret M, et al. Implementing the NICE osteoarthritis guidelines: a mixed methods evaluation. BMC Musculoskelet Disord. 2017;18:380.
- 13. Eyles JP, Hunter DJ, Briggs AM, et al. Improving care for Aboriginal and Torres Strait Islander peoples with musculoskeletal conditions. MJA. 2022;216(2):67–69.