📋 Key Information Summary
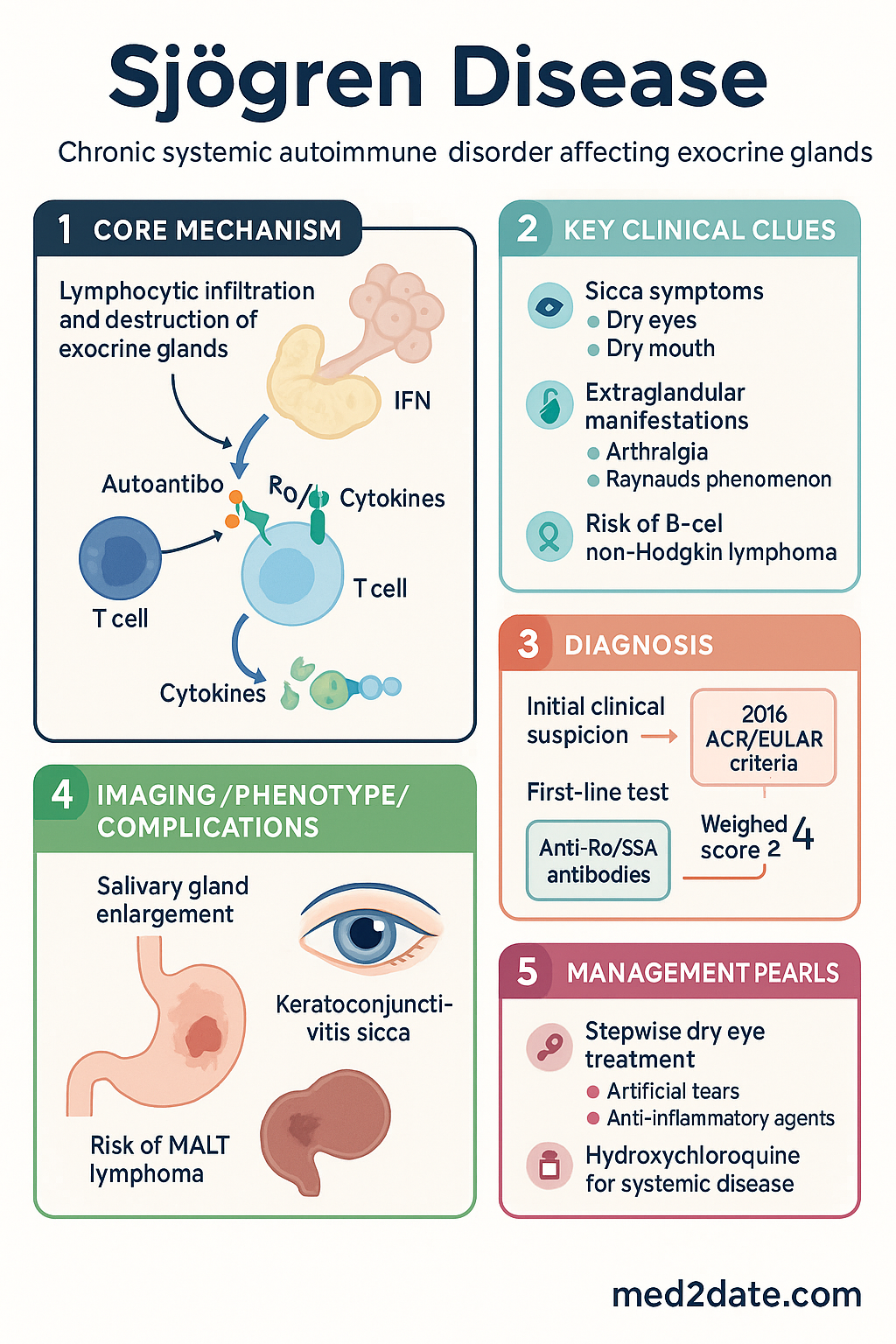
- Sjögren disease is a chronic systemic autoimmune disorder primarily affecting exocrine glands, leading to sicca symptoms (dry eyes, dry mouth).
- Diagnosis integrates sicca symptoms, objective evidence of keratoconjunctivitis sicca (KCS) and salivary gland hypofunction, and serological/ histopathological findings.
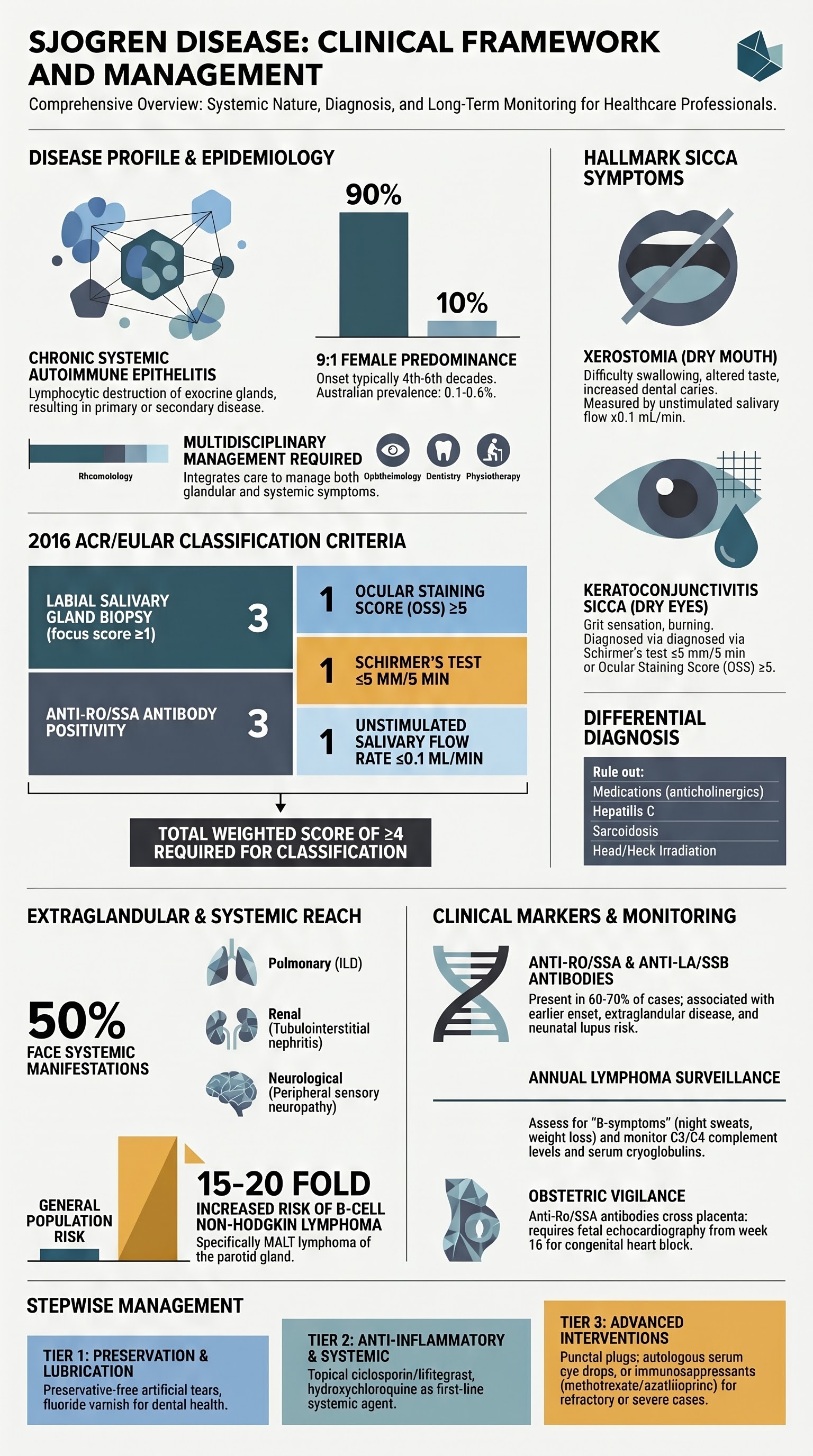
- The 2016 ACR/EULAR classification criteria are the standard, requiring a weighted score ≥4 after excluding other conditions.
- Anti-Ro/SSA antibodies are present in ~60-70% of patients and are strongly associated with earlier onset, extraglandular manifestations, and risk of lymphoma.
- Extraglandular disease can affect nearly any organ system, including musculoskeletal, pulmonary, renal, neurological, and vascular (Raynaud's phenomenon).
- Dry eye treatment is stepwise: artificial tears, then anti-inflammatory agents (ciclosporin, lifitegrast), with punctal plugs and serum tears for refractory cases.
- Patients have a 15-20 fold increased risk of developing B-cell non-Hodgkin lymphoma, particularly MALT lymphoma of the parotid gland.
- Lymphoma surveillance involves regular clinical assessment for "B-symptoms", persistent salivary gland enlargement, and monitoring of serum cryoglobulins and complement levels.
- Systemic treatment for extraglandular disease uses hydroxychloroquine as first-line, with methotrexate, azathioprine, or mycophenolate for more severe manifestations.
- Management requires a multidisciplinary team including rheumatology, ophthalmology, dentistry, and physiotherapy.
Introduction & Australian Epidemiology
Sjögren disease (SjD) is a chronic, systemic autoimmune epithelitis characterised by lymphocytic infiltration and progressive destruction of exocrine glands, particularly salivary and lacrimal glands. It presents as primary SjD or secondary SjD when associated with another autoimmune condition, most commonly rheumatoid arthritis or systemic lupus erythematosus.
In Australia, primary SjD has an estimated prevalence of 0.1-0.6%, affecting approximately 1 in 1000 adults. It demonstrates a strong female predominance (9:1 female-to-male ratio), with typical onset between the 4th and 6th decades of life. Aboriginal and Torres Strait Islander populations may experience different prevalence rates and disease severity, though robust epidemiological data are limited.
Sicca Symptoms (Xerostomia & Keratoconjunctivitis Sicca)
Sicca symptoms are the hallmark of SjD, resulting from lymphocytic infiltration and destruction of salivary and lacrimal glands.
Xerostomia (Dry Mouth)
- Symptoms: Persistent dry mouth, difficulty swallowing dry foods, altered taste, increased dental caries, and oral candidiasis.
- Objective measures: Unstimulated salivary flow rate ≤0.1 mL/min, abnormal parotid sialography showing diffuse sialectasia, or salivary gland scintigraphy showing delayed uptake/excretion.
Keratoconjunctivitis Sicca (Dry Eyes)
- Symptoms: Gritty sensation, foreign body sensation, burning, photophobia, and mucoid discharge.
- Objective measures: Schirmer's test ≤5 mm/5 min, positive ocular staining score (OSS) ≥5 (using fluorescein and lissamine green), or tear film break-up time <10 seconds.
Extraglandular Disease
Up to 50% of patients with primary SjD develop systemic, extraglandular manifestations. These can be organ-specific or constitutional.
| System | Manifestations |
|---|---|
| Constitutional | Profound fatigue, fevers, weight loss. |
| Musculoskeletal | Arthralgia, non-erosive arthritis, myalgia. |
| Cutaneous | Raynaud's phenomenon, palpable purpura (cryoglobulinaemic vasculitis), annular erythema. |
| Pulmonary | Interstitial lung disease (NSIP pattern most common), tracheobronchial sicca, lymphocytic interstitial pneumonitis. |
| Renal | Tubulointerstitial nephritis (type 1 RTA), glomerulonephritis (often with cryoglobulins). |
| Neurological | Peripheral sensory neuropathy, mononeuritis multiplex, autonomic neuropathy, CNS involvement (rare). |
| Haematological | Cytopenias, benign lymphocytic infiltration, risk of non-Hodgkin lymphoma. |
Dry Eye Treatment
Management of dry eye disease (DED) in SjD is stepwise and often requires combination therapy.
Step 1: Artificial Tears & Lubricants
First-line for mild disease. Preservative-free formulations are preferred for frequent use (>4x daily).
Step 2: Anti-Inflammatory Agents
For persistent symptoms or objective signs of inflammation.
Step 3: Procedural & Advanced Therapies
- Punctal Plugs: Occlusion of lacrimal drainage ducts (MBS item 42741).
- Autologous Serum Eye Drops (ASED): Prepared from patient's serum; requires specialist referral and compounding pharmacy access.
- Specialty Contact Lenses: Scleral lenses to protect the cornea and maintain a tear film reservoir.
Anti-Ro/SSA & Anti-La/SSB Antibodies
These are the hallmark autoantibodies of SjD and are central to diagnosis and prognostication.
| Antibody | Prevalence in pSjD | Clinical Significance |
|---|---|---|
| Anti-Ro/SSA | 60-70% | Strongly associated with earlier disease onset, more severe salivary gland involvement, extraglandular manifestations (interstitial lung disease, vasculitis), and increased lymphoma risk. Includes Ro52 and Ro60 subtypes. |
| Anti-La/SSB | 30-40% | Usually occurs in conjunction with anti-Ro. Associated with higher lymphoma risk and more pronounced glandular dysfunction. |
2016 ACR/EULAR Classification Criteria
The 2016 criteria provide a standardised, validated method for classifying primary SjD for clinical research. They can also aid diagnosis after excluding other conditions. A total weighted score ≥4 is required.
| Criterion | Weight/Score |
|---|---|
| Labial salivary gland biopsy with focal lymphocytic sialadenitis and focus score ≥1 | 3 |
| Anti-Ro/SSA antibody positivity | 3 |
| Ocular Staining Score (OSS) ≥5 (or van Bijsterveld score ≥4) | 1 |
| Schirmer's test ≤5 mm/5 min | 1 |
| Unstimulated salivary flow rate ≤0.1 mL/min | 1 |
Entry Criterion: Positive ANA ≥1:320, RF positive, or any systemic feature suggestive of SjD. Exclusion Criteria: History of head/neck radiation, active hepatitis C, AIDS, sarcoidosis, amyloidosis, GVHD, IgG4-related disease, or use of anticholinergic drugs.
Lymphoma Surveillance
Patients with SjD have a significant lifelong risk (standardised incidence ratio ~15-20) of developing B-cell non-Hodgkin lymphoma, most commonly MALT lymphoma in salivary glands.
Risk Factors for Lymphoma Development
- Persistent parotid or major salivary gland enlargement.
- Presence of palpable purpura or vasculitis.
- Low C4 complement levels or mixed cryoglobulinaemia.
- Anti-Ro/SSA and anti-La/SSB positivity.
- High disease activity, persistent B-cell activation, and lymphopenia.
Surveillance Strategy
Special Populations
Pregnancy
Paediatric
Renal Impairment
Aboriginal and Torres Strait Islander Health Considerations
Management of Sjögren disease in Aboriginal and Torres Strait Islander peoples requires culturally safe, holistic, and accessible care.
📚 References
- 1. Shiboski CH, Shiboski SC, Seror R, et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren's Syndrome. Arthritis Rheumatol. 2017;69(1):35-45.
- 2. Rasmussen A, Ice JA, Li H, et al. Comparison of the American-European Consensus Group Sjögren's syndrome classification criteria to newly proposed sets and the 2016 ACR/EULAR criteria. Arthritis Rheumatol. 2018;70(Suppl 10):Abstract.
- 3. Brito-Zerón P, Baldini C, Bootsma H, et al. Sjögren syndrome. Nat Rev Dis Primers. 2016;2:16047.
- 4. Gottenberg JE, Dernis E, Rist S, et al. A prospective, multicentre, randomised, double-blind, placebo-controlled trial assessing the efficacy and safety of abatacept in patients with primary Sjögren's syndrome: The ASAPIII trial. Ann Rheum Dis. 2022;81(5):694-702.
- 5. Theander E, Henriksson G, Ljungberg O, et al. Lymphoma and other malignancies in primary Sjögren's syndrome: a cohort study on cancer incidence and lymphoma predictors. Ann Rheum Dis. 2006;65(6):796-803.
- 6. Price EJ, Rauz S, Tappuni AR, et al. The British Society for Rheumatology guideline for the management of adults with primary Sjögren's Syndrome. Rheumatology (Oxford). 2017;56(10):e24-e48.
- 7. Ramos-Casals M, Brito-Zerón P, Bombardieri S, et al. EULAR recommendations for the management of Sjögren's syndrome with topical and systemic therapies. Ann Rheum Dis. 2020;79(1):3-18.
- 8. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework 2020 summary report. Canberra: AIHW; 2020.
- 9. Singh AG, Singh S, Matteson EL. Rate, risk factors and causes of mortality in patients with Sjögren's syndrome: a systematic review and meta-analysis of cohort studies. Rheumatology (Oxford). 2016;55(3):450-460.
- 10. Mavragani CP, Moutsopoulos HM. Sjögren syndrome. CMAJ. 2014;186(15):E579-E586.