📋 Key Information Summary
- Drug-induced lupus erythematosus (DILE) is a lupus-like syndrome triggered by chronic exposure to specific medications, typically resolving after drug withdrawal.
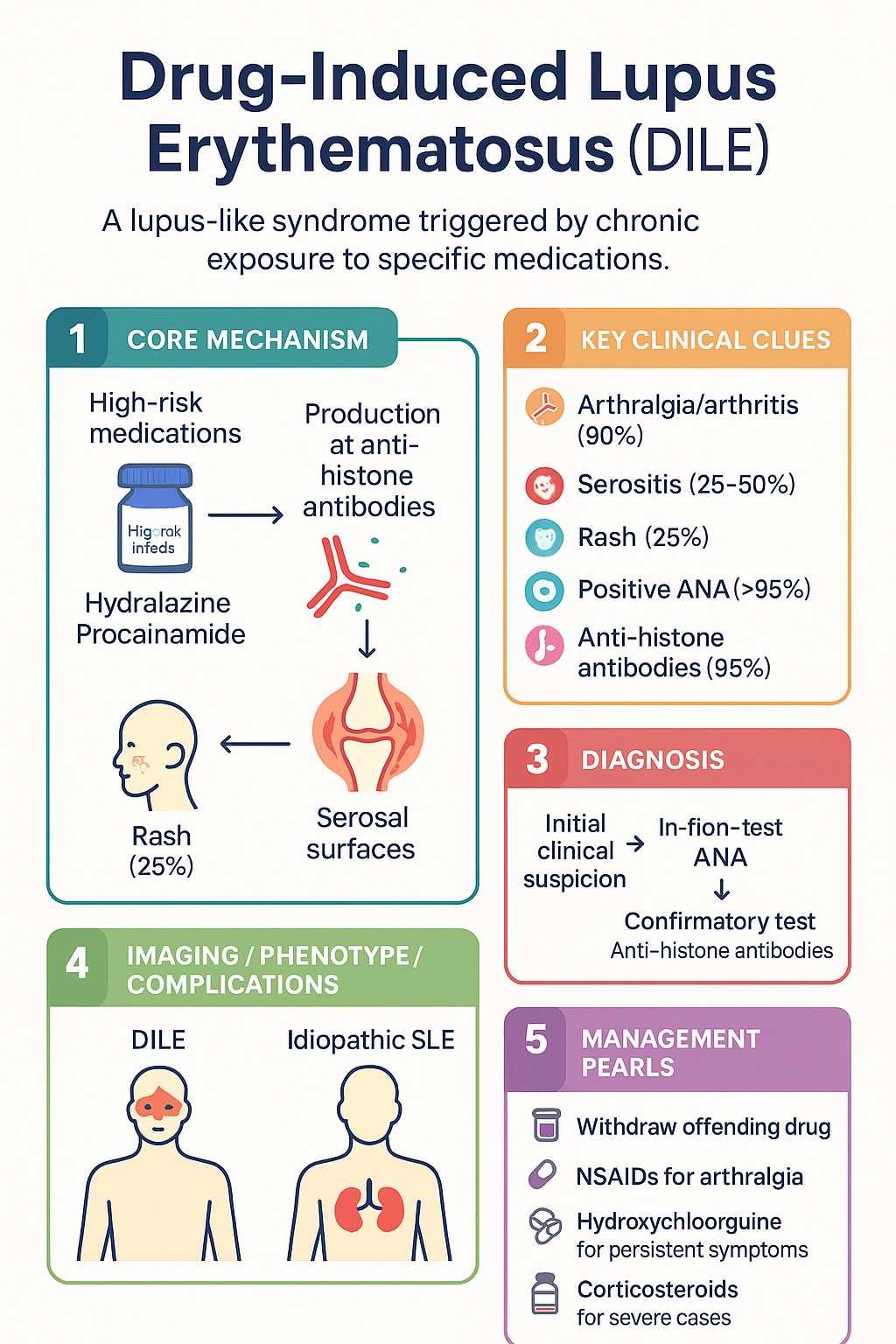
- Classic high-risk causative agents include hydralazine and procainamide; isoniazid and minocycline are also strongly associated.
- Newer causes include biologic agents (anti-TNF therapies) and immune checkpoint inhibitors.
- Clinical presentation is generally milder than idiopathic SLE, with arthralgia/arthritis (90%) and serositis predominating.
- Severe renal or central nervous system involvement is rare, distinguishing DILE from SLE.
- >95% of patients have a positive antinuclear antibody (ANA); anti-histone antibodies are the hallmark serologic finding (>95%).
- Complement levels (C3, C4) are typically normal, and anti-dsDNA antibodies are usually negative.
- Diagnosis is clinical and serologic, requiring temporal association with a causative drug and exclusion of idiopathic SLE.
- The cornerstone of management is identification and withdrawal of the offending drug, leading to resolution over weeks to months.
- Symptomatic treatment includes NSAIDs for arthralgia and hydroxychloroquine for persistent symptoms.
- Short courses of corticosteroids are reserved for significant serositis or cytopenias.
- DILE induced by biologic agents (e.g., anti-TNF) may have a more protracted course and can be serologically atypical (positive anti-dsDNA).
- A detailed medication history is critical in any patient presenting with new lupus-like symptoms.
Introduction & Australian Epidemiology
Drug-induced lupus erythematosus (DILE) is an autoimmune syndrome caused by chronic exposure to certain medications. It shares clinical and serologic features with idiopathic systemic lupus erythematosus (SLE) but is generally milder, has a clear temporal relationship with drug exposure, and typically resolves after the causative agent is discontinued.
The precise incidence in Australia is not well-documented but is estimated to be 15,000 to 30,000 cases per year in the United States. Given similar prescribing patterns for high-risk drugs like hydralazine and procainamide, a proportional incidence is expected in Australia. The risk is highest with hydralazine (5–10% of users) and procainamide (15–20% of users) when used chronically. The condition may be under-recognised due to its variable presentation and the common use of causative medications for prevalent conditions like hypertension, arrhythmia, and tuberculosis.
Understanding DILE is crucial for Australian general practitioners, rheumatologists, and clinical immunologists to avoid misdiagnosis of idiopathic SLE and to ensure appropriate management through drug withdrawal.
Common Causative Drugs
Over 100 drugs have been implicated in DILE. The risk is dose- and duration-dependent, particularly for hydralazine and procainamide. They are categorised by risk level and mechanism.
High-Risk Drugs (Strongly Associated)
Moderate-Risk Drugs
Quinidine (antiarrhythmic), carbamazepine (anticonvulsant), methyldopa (antihypertensive), and sulfasalazine (DMARD) are recognised causes. DILE associated with these agents also typically features anti-histone antibodies.
Biologic-Induced Lupus-like Syndrome
Checkpoint Inhibitor-Induced Lupus
Immune checkpoint inhibitors (e.g., pembrolizumab, nivolumab, ipilimumab) used in oncology can trigger a wide spectrum of immune-related adverse events, including rare but severe lupus-like syndromes. These are managed in conjunction with oncology teams.
Clinical Features & Diagnosis
DILE is a diagnosis of exclusion based on clinical presentation, serology, and a clear temporal relationship with a causative drug.
Clinical Presentation
Symptoms typically appear after months to years of continuous drug exposure. The presentation is generally milder than idiopathic SLE.
| Feature | Frequency in DILE | Comparison to Idiopathic SLE |
|---|---|---|
| Arthralgia/Arthritis | ~90% | Very common in both; DILE arthritis is often non-erosive. |
| Serositis (pleuritis, pericarditis) | 25–50% | Less common than arthritis but frequent. |
| Rash (malar, discoid, photosensitive) | 25% | Less frequent and severe; true discoid rash rare. |
| Constitutional (fever, fatigue, weight loss) | Common | Similar to SLE flares. |
| Renal Involvement | Rare (<5%) | Major distinction; significant nephritis suggests SLE. |
| CNS Involvement | Very Rare | Major distinction; psychosis or seizures suggest SLE. |
| Mucosal Ulcers, Alopecia | Uncommon | Less prominent. |
Diagnostic Criteria (Proposed)
No formal classification criteria exist, but diagnosis requires:
- Exposure to a known causative drug for at least 1 month (often >3–6 months) prior to symptom onset.
- At least one clinical feature of SLE (arthralgia/arthritis, serositis, rash, fever).
- Positive antinuclear antibody (ANA) ≥1:160.
- Resolution of symptoms within weeks to months (usually <1 year) after drug discontinuation.
- Absence of prior history of idiopathic SLE.
Key Serologic Investigations
Management
The primary goal is to identify and withdraw the causative drug. Symptomatic treatment is then tailored to the severity of the clinical features.
Stepwise Approach
Special Considerations: Biologic-Induced DILE
Management is more complex. The decision to stop the biologic agent must be made in consultation with the treating specialist (e.g., rheumatologist, gastroenterologist, dermatologist) balancing the risk of lupus flare against the benefit of the biologic for the underlying condition. Symptoms may persist longer. Hydroxychloroquine and corticosteroids are often needed. Switching within the anti-TNF class is generally not recommended due to high cross-reactivity.
Follow-up
Monitor symptoms and serology (ANA, anti-histone, complement) every 3–6 months until resolution. ANA may remain positive for months to years despite clinical improvement.
Aboriginal and Torres Strait Islander Health Considerations
The burden of autoimmune and rheumatic disease is higher in Aboriginal and Torres Strait Islander peoples. DILE must be considered in the differential diagnosis of musculoskeletal symptoms, particularly in communities where high-risk medications like isoniazid for tuberculosis or hydralazine for hypertension are used.
📚 References
- 1. Borchers AT, Keen CL, Gershwin ME. Drug-induced lupus. Ann N Y Acad Sci. 2007;1108:166-82. doi:10.1196/annals.1422.019.
- 2. Rubin RL. Drug-induced lupus. In: Wallace DJ, Hahn BH, eds. Dubois' Lupus Erythematosus and Related Syndromes. 9th ed. Elsevier; 2019:442-55.
- 3. Marzano AV, Vezzoli P, Crosti C. Drug-induced lupus: an update on its dermatologic aspects. Lupus. 2009;18(11):935-40. doi:10.1177/0961203309345725.
- 4. Katz U, Zandman-Goddard G. Drug-induced lupus: an update. Autoimmun Rev. 2010;10(1):46-50. doi:10.1016/j.autrev.2010.07.005.
- 5. Flores-Borja F, Jury EC, Mauri C, Ehrenstein MR. Defective B cell function in patients with drug-induced lupus. Arthritis Rheum. 2009;60(10):3031-42. doi:10.1002/art.24788.
- 6. Sparks JA, Costenbader KH. Drug-induced lupus associated with synthetic and biologic disease-modifying antirheumatic drugs. Lupus. 2015;24(4-5):423-30. doi:10.1177/0961203314567555.
- 7. Moulis G, Sommet A, Lapeyre-Mestre M, et al. Association of drug-induced lupus and minocycline: a population-based case-control study. Semin Arthritis Rheum. 2014;44(2):190-6. doi:10.1016/j.semarthrit.2014.05.005.
- 8. Ramos-Casals M, Brito-Zerón P, Soto MJ, Cuadrado MJ, Khamashta MA. Autoimmune diseases induced by TNF-targeted therapies. Best Pract Res Clin Rheumatol. 2008;22(5):847-61. doi:10.1016/j.berh.2008.09.004.
- 9. Australian Institute of Health and Welfare (AIHW). Rheumatoid arthritis and other musculoskeletal conditions. AIHW; 2023. [Accessed 2024].
- 10. RHDAustralia (a program of the Aboriginal Medical Services Alliance Northern Territory). Rheumatic Heart Disease Australia Annual Report 2023. Darwin: RHDAustralia; 2023.
- 11. Bossingham D. Systemic lupus erythematosus in the far north of Queensland. Lupus. 2003;12(4):327-31. doi:10.1191/0961203303lu375oa.
- 12. The Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice. 9th ed. RACGP; 2016.