📋 Key Information Summary
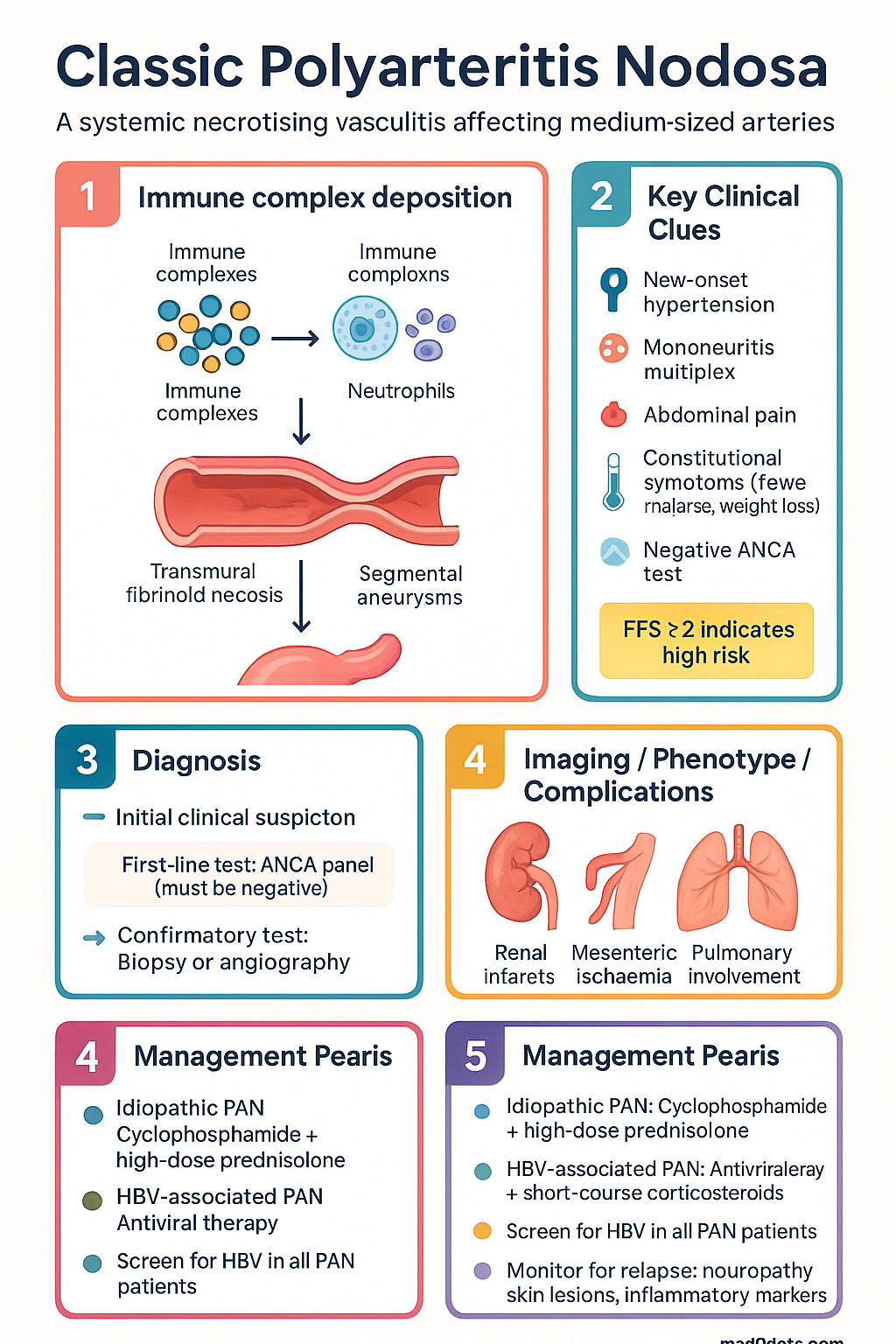
- Classic PAN is a systemic necrotising vasculitis of medium-sized muscular arteries — ANCA-negative and does NOT cause glomerulonephritis or pulmonary capillaritis.
- Approximately 30% of cases are associated with hepatitis B virus (HBV) infection via immune complex deposition; idiopathic cases account for the remainder.
- Hallmark pathology: transmural fibrinoid necrosis with neutrophilic infiltrate at arterial bifurcations, progressing to segmental aneurysms visible on conventional angiography.
- Classic organ involvement includes renal (infarcts, renovascular hypertension — no glomerulonephritis), peripheral nerves (mononeuritis multiplex), mesenteric vasculature (ischaemic colitis), and testes.
- Diagnosis rests on clinical features plus either histological confirmation (biopsy of symptomatic site) or characteristic angiographic aneurysms — ACR 1990 classification criteria require ≥3 of 10 features.
- Five-factor score (FFS 2009) stratifies prognosis and guides treatment intensity: age >65, cardiac involvement, GI involvement, renal insufficiency (Cr >140 µmol/L), ear/nose/throat involvement.
- Idiopathic PAN: treat with combination cyclophosphamide + high-dose prednisolone for remission induction; azathioprine or methotrexate for maintenance.
- HBV-associated PAN: antiviral therapy (entecavir or tenofovir) is the cornerstone; short-course corticosteroids plus plasma exchange — do NOT give prolonged cyclophosphamide.
- Prednisolone taper typically extends over 12–18 months; abrupt discontinuation risks relapse.
- Pulmonary involvement is ABSENT in classic PAN — if present, consider ANCA-associated vasculitis (e.g., GPA, MPA, EGPA) instead.
- Aboriginal and Torres Strait Islander peoples have higher HBV prevalence; screen all PAN patients for HBV and tailor therapy accordingly.
- Relapse occurs in 10–20% of idiopathic PAN; monitor for recurrent neuropathy, skin lesions, or rising inflammatory markers after remission.
Introduction & Australian Epidemiology
Classic polyarteritis nodosa (PAN) is a systemic necrotising vasculitis predominantly affecting medium-sized muscular arteries, causing transmural inflammation, segmental necrosis, and subsequent ischaemic injury to visceral organs and peripheral nerves. Crucially, PAN spares the pulmonary circulation and does not produce glomerulonephritis — features that distinguish it from ANCA-associated vasculitides.
In Australia, PAN is rare, with an estimated incidence of 2–9 per million population per year. The disease shows a male predominance (M:F ratio ~2:1) and a peak incidence in the fifth to sixth decade of life. Approximately 30% of cases are associated with hepatitis B virus (HBV) infection, an important consideration given the higher prevalence of chronic HBV in Aboriginal and Torres Strait Islander communities and among migrants from endemic regions (Southeast Asia, Sub-Saharan Africa, Pacific Islands).
The distinction between HBV-associated and idiopathic PAN is therapeutically critical: HBV-associated PAN responds best to antiviral therapy with short-course corticosteroids and plasma exchange, whereas idiopathic PAN requires immunosuppressive induction with cyclophosphamide. Accurate classification therefore directly impacts treatment outcomes.
Pathophysiology & Classification
Pathogenesis
Classic PAN is characterised by ANCA-negative necrotising arteritis of medium-sized muscular arteries at branch points. The pathological hallmark is transmural fibrinoid necrosis with neutrophil infiltration of the vessel wall, progressing to mononuclear cell infiltrates, intimal proliferation, and eventual fibrosis. Segmental aneurysms (up to 1 cm) form at arterial bifurcations and are visible on conventional catheter-based angiography.
Two distinct aetiological pathways are recognised:
- HBV-associated PAN (~30% of cases): Immune complexes containing HBV surface antigen (HBsAg) and antibody deposit in arterial walls, activating complement and driving transmural inflammation. Circulating immune complexes correlate with disease activity. This form typically presents within six months of acute HBV infection and is more common in younger patients.
- Idiopathic PAN (~70% of cases): No identifiable infectious trigger. The immunopathogenesis is incompletely understood but involves T-cell–mediated vascular injury and macrophage activation. Some cases are associated with hairy-cell leukaemia, relapsing polychondritis, or familial Mediterranean fever (FMF).
Classification Criteria — ACR 1990
The American College of Rheumatology (ACR) 1990 classification criteria require ≥3 of the following 10 features for classifying a patient as having PAN:
| Criterion | Definition | Sensitivity / Specificity |
|---|---|---|
| 1. Weight loss ≥4 kg | Unintentional, since illness began, not attributable to dieting | 73% / 73% |
| 2. Livedo reticularis | Mottled, net-like violaceous skin discolouration | 16% / 96% |
| 3. Testicular pain or tenderness | On history or examination, not attributable to infection or trauma | 16% / 96% |
| 4. Myalgia, weakness, or leg tenderness | Diffuse myalgias or leg tenderness, or mild muscle weakness of intrinsic muscles | 65% / 75% |
| 5. Mononeuropathy or polyneuropathy | Development of mononeuritis multiplex or peripheral polyneuropathy | 58% / 74% |
| 6. Diastolic BP >90 mmHg | New-onset or worsening hypertension | 53% / 73% |
| 7. Elevated BUN or creatinine | BUN >40 mg/dL (14.3 mmol/L) or creatinine >1.5 mg/dL (133 µmol/L) — due to renal infarction, NOT glomerulonephritis | 37% / 88% |
| 8. HBV seropositivity | Positive anti-HBsAg antibody or HBsAg | 19% / 89% |
| 9. Arteriographic abnormality | Aneurysms or occlusions of visceral arteries (not due to atherosclerosis, fibromuscular dysplasia, or other causes) | 45% / 91% |
| 10. Biopsy of small or medium artery containing PMN | Histological evidence of granulocytes or granulocytes and mononuclear cells in the artery wall | 22% / 91% |
The 1990 ACR criteria have a reported sensitivity of 82.2% and specificity of 86.6% for distinguishing PAN from other vasculitides. These are classification criteria (designed for research), not diagnostic criteria — clinical judgement remains essential.
Clinical Features
PAN is a multisystem disease with protean manifestations driven by ischaemia and infarction of medium-sized arteries. Constitutional symptoms (fever, malaise, weight loss) are present in >50% of patients at diagnosis. Organ-specific features depend on the vascular bed involved:
| System | Manifestations | Frequency |
|---|---|---|
| Peripheral nerves | Mononeuritis multiplex (foot/wrist drop); painful sensory neuropathy; asymmetric polyneuropathy | 50–70% |
| Renal | Renovascular hypertension (renal artery branch involvement); renal infarction (flank pain, haematuria); progressive renal impairment — NO glomerulonephritis | 40–60% |
| Gastrointestinal | Mesenteric ischaemia (postprandial abdominal pain, weight loss, GI haemorrhage, bowel perforation); hepatic artery involvement | 30–40% |
| Skin | Livedo reticularis; subcutaneous nodules (classic "nodosa"); purpura; digital gangrene; ulcers | 30–40% |
| Musculoskeletal | Myalgia; arthralgia (non-erosive, non-deforming); leg tenderness | 50–65% |
| Testicular | Testicular pain/tenderness (highly specific but low sensitivity) | 16% |
| Cardiac | Coronary arteritis (angina, MI); pericarditis; cardiomyopathy — contributes to mortality | 10–30% |
| Central nervous system | Cerebral infarction; seizures; encephalopathy (less common than peripheral neuropathy) | 5–10% |
Features That EXCLUDE Classic PAN
- Pulmonary involvement (haemoptysis, nodules, cavitation) → consider GPA, MPA, or EGPA
- Glomerulonephritis (dysmorphic red cells, RBC casts, rapidly declining GFR) → consider ANCA-associated vasculitis or IgA vasculitis
- Positive ANCA (c-ANCA/PR3 or p-ANCA/MPO) → not classic PAN
- Small-vessel involvement on biopsy (capillaritis, venulitis) → not classic PAN
Investigations
Laboratory Tests
Imaging
Histopathology
Risk Stratification & Severity Scoring
The Five-Factor Score (FFS), revised in 2009 by the French Vasculitis Study Group (FVSG), is used to predict mortality and guide treatment intensity in systemic vasculitides including PAN:
Five-Factor Score (FFS 2009) — Adverse Prognostic Factors
| Factor | Definition |
|---|---|
| Age >65 years | At time of diagnosis |
| Cardiac symptoms | Cardiomyopathy, heart failure, or pericarditis attributable to vasculitis |
| GI involvement | Mesenteric ischaemia, perforation, haemorrhage, pancreatitis, or biliary involvement |
| Renal insufficiency | Serum creatinine >140 µmol/L (≥1.58 mg/dL) |
| ENT involvement | Absent in classic PAN (only scored in AAV) — effectively only 4 factors apply to PAN |
Treatment
Treatment of PAN depends critically on whether the disease is idiopathic or HBV-associated. The two forms require fundamentally different therapeutic strategies.
Idiopathic PAN — Remission Induction
Idiopathic PAN — Remission Maintenance
HBV-Associated PAN — Specific Treatment
Short-course corticosteroids in HBV-PAN: Prednisolone 1 mg/kg/day for 2 weeks, then rapid taper over 2–4 weeks (total duration ≤6 weeks). Only enough to control acute vasculitis while antivirals take effect.
Plasma exchange in HBV-PAN: 3–7 sessions (60 mL/kg per session) in the first 2 weeks to remove circulating immune complexes. Indicated for severe disease (FFS ≥1) or visceral crisis. Available at major tertiary centres.
Supportive Therapies
| Intervention | Indication | Details |
|---|---|---|
| Antihypertensive therapy | Renovascular hypertension | ACE inhibitor or ARB first-line; target BP <130/80 mmHg |
| Pneumocystis jirovecii prophylaxis | All patients on cyclophosphamide or ≥20 mg prednisolone >4 weeks | Trimethoprim 160 mg / sulfamethoxazole 800 mg PO daily (or 3 times/week) — PBS General Benefit |
| Osteoporosis prophylaxis | Prednisolone ≥7.5 mg for ≥3 months | Calcium 1000 mg + vitamin D 1000 IU daily; consider bisphosphonate if age >65 or prior fracture |
| Gastric protection | Prednisolone + NSAID or GI risk factors | Pantoprazole 20–40 mg daily — PBS General Benefit |
| Analgesia | Neuropathic pain, myalgia | Gabapentin, pregabalin, or duloxetine for neuropathic pain; paracetamol for myalgia |
Monitoring
Disease Activity Monitoring
Relapse Surveillance
- Watch for recurrent mononeuritis multiplex, new skin nodules/ulcers, rising ESR/CRP, worsening hypertension, or abdominal symptoms.
- Relapse is more common during steroid taper — reduce taper rate if relapse occurs.
- HBV-PAN relapse usually indicates antiviral failure or non-adherence — check HBV DNA and antiviral resistance.
Cyclophosphamide Toxicity Monitoring
| Toxicity | Monitoring | Action |
|---|---|---|
| Neutropenia | FBC every 2 weeks during oral therapy; day 10–14 after IV pulse | Hold if ANC <1.5 × 10⁹/L; G-CSF if clinically indicated |
| Haemorrhagic cystitis | Urinalysis each visit; maintain hydration ≥2 L/day | Mesna co-administration with IV pulses; switch to azathioprine if recurrent |
| Gonadal toxicity | Counselling at baseline | Consider GnRH agonist (goserelin) or sperm/egg cryopreservation before treatment |
| Bladder malignancy | Lifelong risk; annual urinalysis for haematuria | Urological referral if persistent haematuria after cumulative dose >30 g |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Quick Reference — Treatment Summary
📚 References
- 1. Jennette JC, Falk RJ, Bacon PA, et al. 2012 revised International Chapel Hill Consensus Conference nomenclature of vasculitides. Arthritis Rheum. 2013;65(1):1–11.
- 2. Lightfoot RW Jr, Michel BA, Bloch DA, et al. The American College of Rheumatology 1990 criteria for the classification of polyarteritis nodosa. Arthritis Rheum. 1990;33(8):1088–1093.
- 3. Guillevin L, Pagnoux C, Seror R, et al. The Five-Factor Score revisited: assessment of prognoses of systemic necrotizing vasculitides based on the French Vasculitis Study Group (FVSG) cohort. Medicine (Baltimore). 2011;90(1):19–27.
- 4. Pagnoux C, Seror R, Henegar C, et al. Clinical features and outcomes in 348 patients with polyarteritis nodosa: a systematic retrospective study of patients diagnosed between 1963 and 2005 and entered into the French Vasculitis Study Group Database. Arthritis Rheum. 2010;62(2):616–626.
- 5. Guillevin L, Mahr A, Callard P, et al. Hepatitis B virus-associated polyarteritis nodosa: clinical characteristics, outcome, and impact of treatment in 115 patients. Medicine (Baltimore). 2005;84(5):313–322.
- 6. Mukhtyar C, Guillevin L, Cid MC, et al. EULAR recommendations for the management of primary small and medium vessel vasculitis. Ann Rheum Dis. 2009;68(3):310–317.
- 7. De Virgilio A, Greco A, Magliulo G, et al. Polyarteritis nodosa: a contemporary overview. Autoimmun Rev. 2016;15(6):564–570.
- 8. Australian Government Department of Health. National Hepatitis B Strategy 2018–2022. Canberra: Commonwealth of Australia; 2018.
- 9. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework 2020 summary report. Canberra: AIHW; 2020.
- 10. Kidney Health Australia. Caring for Australasians with Renal Impairment (CARI) Guidelines — Renal Vasculitis. Melbourne: KHA; 2020.
- 11. RACGP. Guidelines for preventive activities in general practice (Red Book). 10th edn. East Melbourne: RACGP; 2018.
- 12. Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook. Australian Government Department of Health, Canberra. Updated 2023. Available at: immunisationhandbook.health.gov.au.
- 13. Robson JC, Dawson J, Cronholm PF, et al. Patient-reported outcomes in vasculitis. Curr Opin Rheumatol. 2018;30(1):48–54.