📋 Key Information Summary
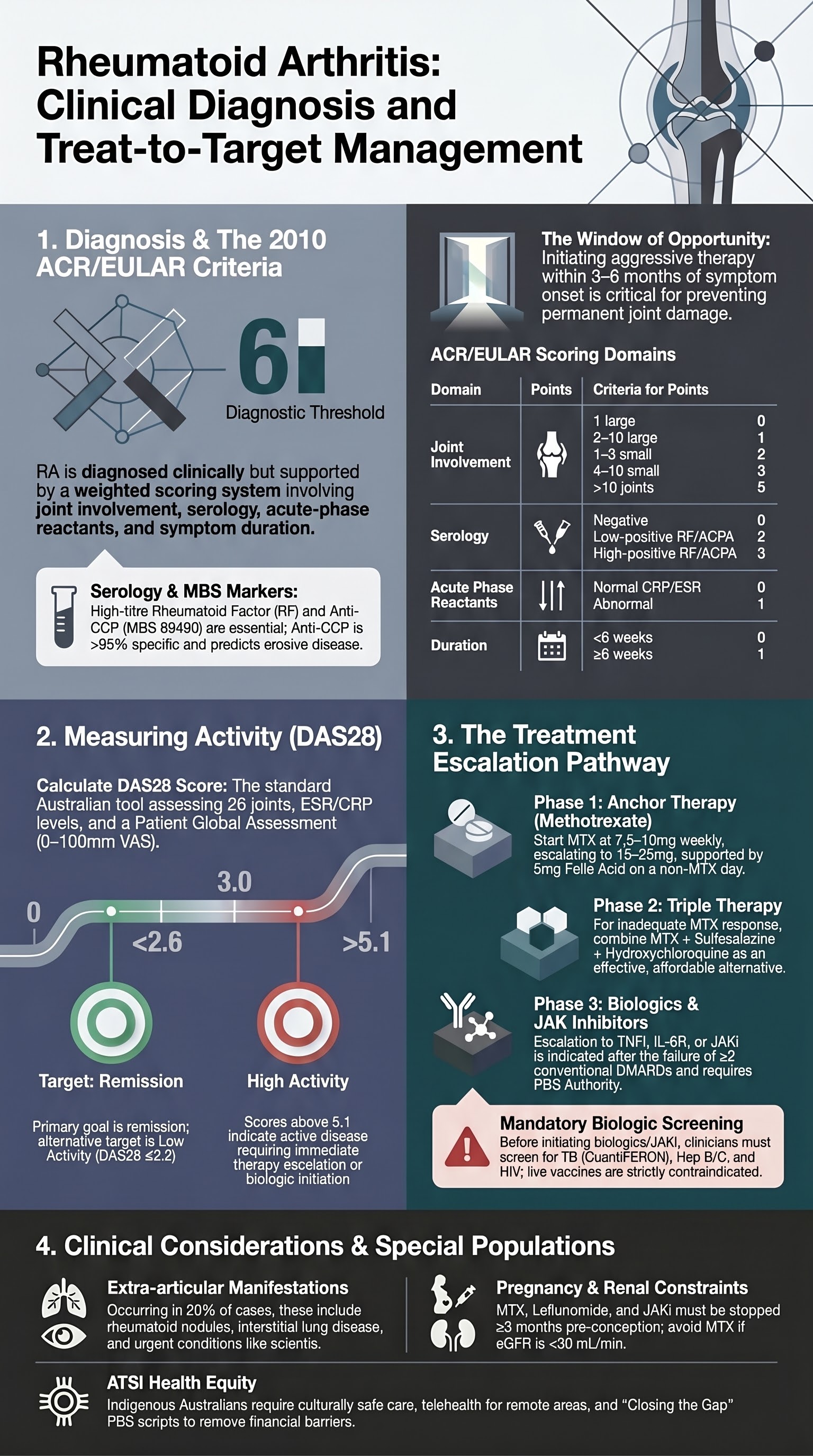
- Diagnosis: Based on 2010 ACR/EULAR criteria (score ≥6/10): joint involvement, serology (RF/anti-CCP), acute-phase reactants (CRP/ESR), symptom duration.
- First-line DMARD: Methotrexate (MTX) 7.5–25 mg weekly (oral or subcutaneous) with folic acid 5 mg weekly (not on MTX day).
- Combination csDMARDs: MTX + sulfasalazine + hydroxychloroquine (triple therapy) for inadequate response to MTX monotherapy.
- Biologic/tsDMARD escalation: After failure of ≥2 csDMARDs. Options include TNFi (adalimumab, etanercept), IL-6R (tocilizumab), JAKi (tofacitinib, baricitinib).
- Treat-to-target: Aim for remission (DAS28 <2.6) or low disease activity (DAS28 ≤3.2) every 3–6 months.
- DAS28 calculation: Based on 28 tender/swollen joint counts, ESR or CRP, patient global assessment (0–100 mm VAS).
- Monitoring: FBC, LFTs, creatinine every 2–4 weeks initially for MTX, then every 2–3 months. Annual eye exam for hydroxychloroquine.
- Safety: Screen for TB (QuantiFERON) and hepatitis B/C before biologics/JAKi. Live vaccines contraindicated.
- Extra-articular: Rheumatoid nodules, interstitial lung disease, vasculitis, episcleritis. Require specialist co-management.
- ATSI consideration: Higher prevalence, younger onset, more aggressive disease. Ensure culturally safe care and access to DMARDs.
Introduction & Australian Epidemiology
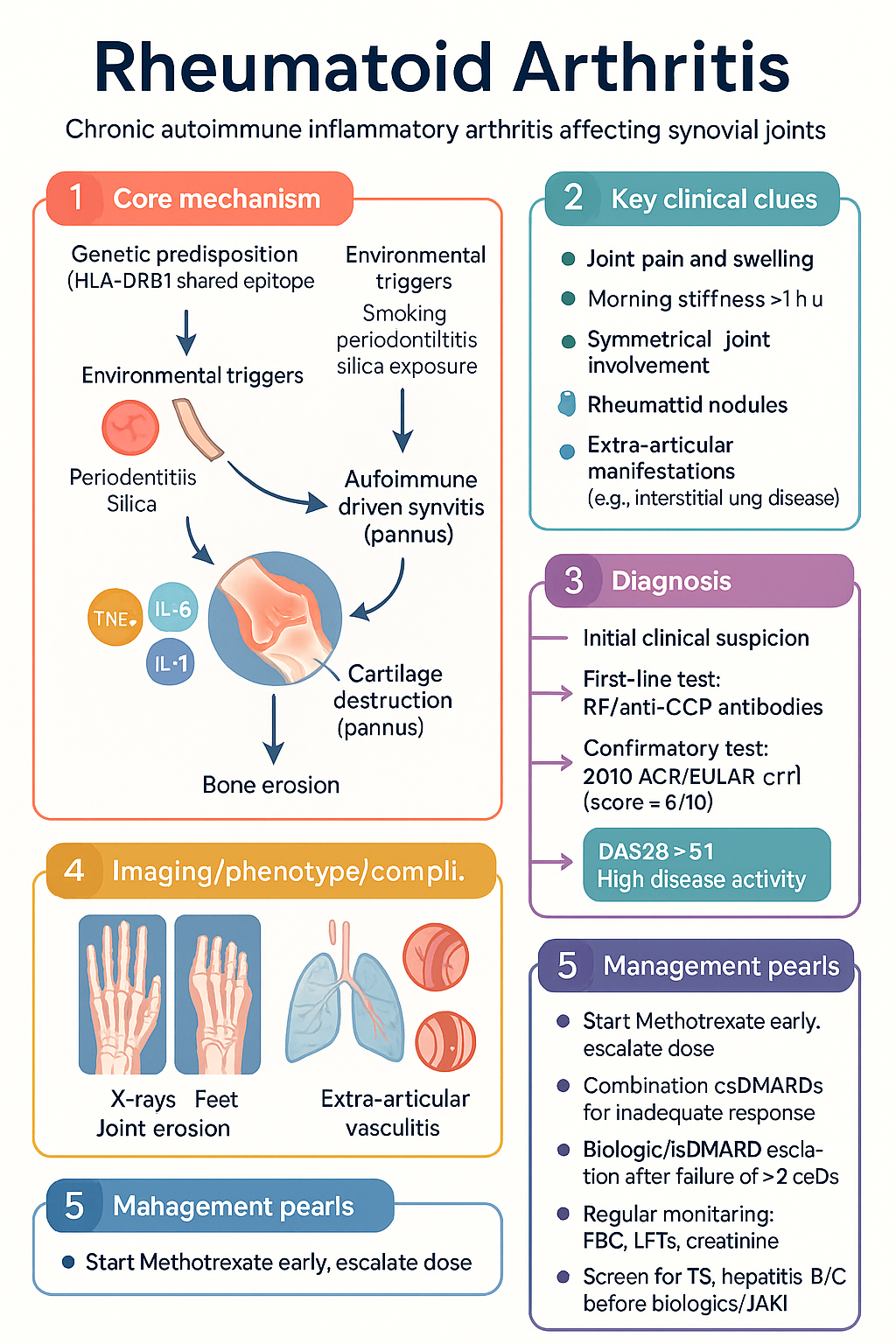
Rheumatoid arthritis (RA) is a chronic, systemic autoimmune inflammatory arthritis primarily affecting synovial joints. In Australia, prevalence is ~0.5–1% of adults, with higher rates in Aboriginal and Torres Strait Islander communities. Onset is typically between 35–60 years, with a female:male ratio of 3:1. Early diagnosis and aggressive treat-to-target therapy within 3–6 months of symptom onset ('window of opportunity') significantly improves long-term structural and functional outcomes.
Pathophysiology
Autoimmune-driven synovitis (pannus) leads to cartilage destruction and bone erosion. Key cytokines include TNF-α, IL-6, and IL-1. Genetic predisposition (HLA-DRB1 shared epitope) interacts with environmental triggers (smoking, periodontitis, silica exposure).
Diagnosis & 2010 ACR/EULAR Criteria
No single pathognomonic test. Diagnosis is clinical, supported by serology and imaging. The 2010 ACR/EULAR classification criteria (score ≥6/10 definite RA) are used for early identification.
| Domain | Score | Criteria |
|---|---|---|
| Joint Involvement | 0–5 | 1 large (0), 2–10 large (1), 1–3 small (2), 4–10 small (3), >10 (at least 1 small) (5) |
| Serology | 0–3 | Negative RF & negative ACPA (0), low-positive RF or ACPA (2), high-positive RF or ACPA (3) |
| Acute Phase Reactants | 0–1 | Normal CRP and normal ESR (0), abnormal CRP or abnormal ESR (1) |
| Duration of Symptoms | 0–1 | <6 weeks (0), ≥6 weeks (1) |
Key investigations (MBS items):
Disease Activity Scoring (DAS28)
DAS28 is the standard Australian tool for treat-to-target. Calculated using 28 tender/swollen joint counts, ESR (or CRP), and patient global health VAS (0–100).
Methotrexate & Conventional DMARDs
Methotrexate (MTX) is the anchor drug. Start early, escalate dose every 4 weeks to target (usually 15–25 mg/week).
Triple therapy: MTX + sulfasalazine + hydroxychloroquine is an effective and affordable alternative to biologics for moderate disease activity.
Biologics & Targeted Synthetic DMARDs
Indicated after failure of ≥2 csDMARDs (including MTX) or with poor prognostic factors. Require PBS Authority approval.
| Class | Examples | Key Considerations |
|---|---|---|
| TNF inhibitors (TNFi) | Adalimumab (Humira®), Etanercept (Enbrel®) | First-line biologic. SC injection. Risk of infection, demyelination. |
| IL-6 receptor inhibitors | Tocilizumab (Actemra®) | Can mask CRP rise. Monitor lipids and neutrophils. IV or SC. |
| JAK inhibitors (JAKi) | Tofacitinib (Xeljanz®), Baricitinib (Olumiant®) | Oral. Increased VTE, MACE, malignancy risk in >50y with CV risk factors (FDA warning). |
PBS Authority Required: For patients with severe active RA (DAS28 >5.1) despite adequate trial of csDMARDs.
Extra-articular Disease
Occurs in ~20% of patients, often with high-titre RF/anti-CCP. Indicates severe systemic disease.
Treat-to-Target Strategy
Special Populations
ATSI Health Considerations
📚 References
- 1. Aletaha D, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569-81.
- 2. Smolen JS, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheum Dis. 2023;82(1):3-18.
- 3. Royal Australian College of General Practitioners (RACGP). Rheumatoid arthritis: early diagnosis and disease management. East Melbourne: RACGP; 2020.
- 4. Australian Rheumatology Association (ARA). Biologics and targeted synthetic DMARDs: information for prescribers. 2023. Available from: https://www.rheumatology.org.au
- 5. Australian Government Department of Health. Pharmaceutical Benefits Scheme (PBS). Available from: www.pbs.gov.au
- 6. National Health and Medical Research Council (NHMRC). Australian guidelines for the prevention and control of infection in healthcare. Canberra: NHMRC; 2019.
- 7. Aboriginal and Torres Strait Islander Health Team. Cultural safety in healthcare. Australian Institute of Health and Welfare (AIHW). 2022.
- 8. Fraenkel L, et al. American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Care Res. 2021;73(7):924-39.
- 9. Ytterberg SR, et al. Cardiovascular and cancer risk with tofacitinib in rheumatoid arthritis. N Engl J Med. 2022;386(4):316-26.
- 10. Buch MH, et al. Treating rheumatoid arthritis to target: 2014 update of the recommendations of an international task force. Ann Rheum Dis. 2016;75(1):3-15.