📋 Key Information Summary
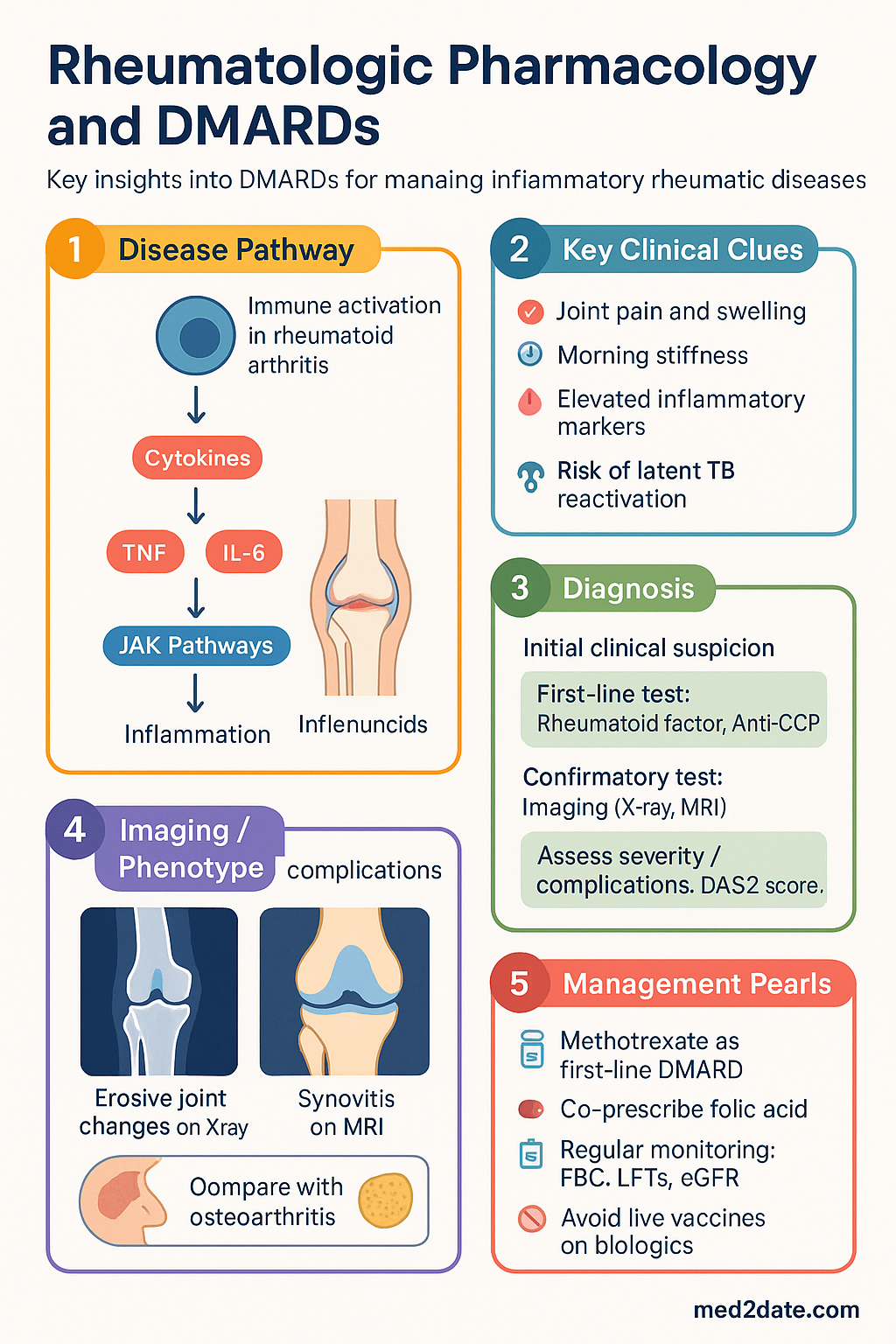
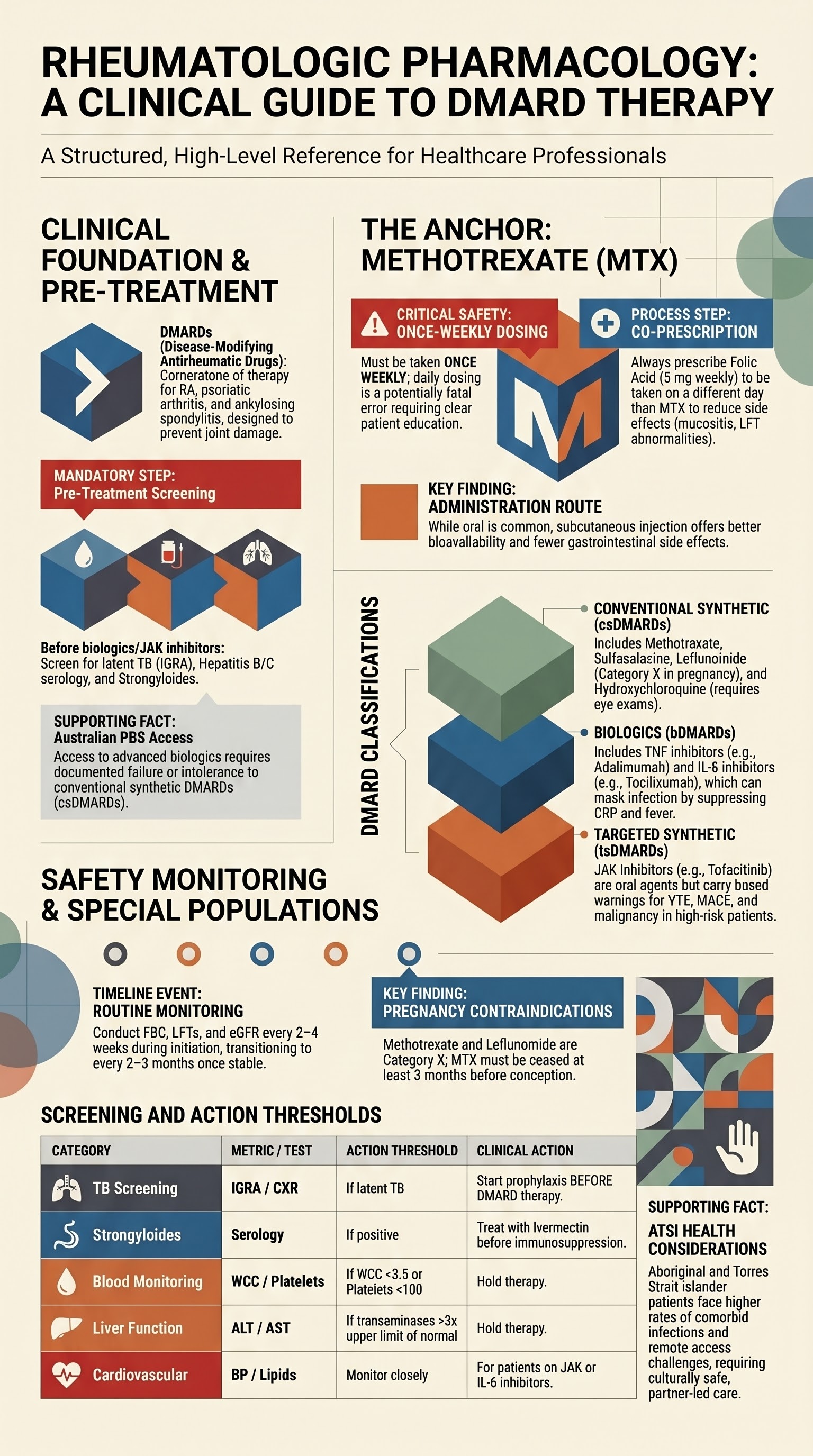
- DMARDs (Disease-Modifying Antirheumatic Drugs) are the cornerstone of therapy for inflammatory rheumatic diseases like rheumatoid arthritis (RA), aiming to prevent joint damage and disability.
- Methotrexate remains the anchor drug for RA; standard dose is 15–25 mg once weekly orally or subcutaneously, always co-prescribed with folic acid 5 mg weekly (not on the same day).
- Pre-treatment screening is mandatory before starting any biologic or targeted synthetic DMARD. Essential tests include latent TB screening (IGRA ± CXR), hepatitis B/C serology, and strongyloides serology in at-risk patients.
- Conventional synthetic DMARDs (csDMARDs) include methotrexate, sulfasalazine, leflunomide, and hydroxychloroquine. Choice depends on disease, comorbidities, and pregnancy plans.
- TNF inhibitors (e.g., adalimumab, etanercept) are first-line biologic DMARDs (bDMARDs) after csDMARD failure. They increase infection risk, particularly reactivation of latent TB.
- IL-6 inhibitors (tocilizumab, sarilumab) are effective for RA but can mask infection by suppressing CRP and fever; monitor lipids and for GI perforation.
- JAK inhibitors (tofacitinib, baricitinib, upadacitinib) are oral targeted synthetic DMARDs (tsDMARDs). They carry a higher risk of VTE, herpes zoster, and MACE in high-risk patients over 50 with CV risk factors.
- Routine monitoring for all DMARDs includes FBC, LFTs, and eGFR. Frequency is higher during initiation (e.g., every 2–4 weeks) then every 2–3 months when stable.
- Live vaccines (e.g., MMR, varicella, yellow fever) are contraindicated in patients on biologic/JAK inhibitor therapy.
- For Aboriginal and Torres Strait Islander patients, consider higher rates of comorbid infections (TB, strongyloides), remote access challenges for monitoring, and culturally safe care.
Introduction & Australian Epidemiology
Inflammatory rheumatic diseases like rheumatoid arthritis (RA), psoriatic arthritis, and ankylosing spondylitis are chronic autoimmune conditions leading to progressive joint damage, disability, and reduced quality of life. Disease-Modifying Antirheumatic Drugs (DMARDs) are fundamental to management, targeting underlying inflammatory pathways to achieve remission or low disease activity.
In Australia, RA affects approximately 2% of the population, with a higher prevalence and earlier onset observed in Aboriginal and Torres Strait Islander communities. The economic and personal burden is significant, making effective, early, and targeted DMARD therapy a priority within the Australian healthcare system.
Pre-treatment Screening (TB, HBV, Strongyloides)
Mandatory screening is required before initiating any biologic (bDMARD) or targeted synthetic (tsDMARD) therapy to prevent severe, opportunistic infections.
| Infection | Screening Test | Action if Positive | Australian Notes |
|---|---|---|---|
| Tuberculosis (TB) | Interferon-Gamma Release Assay (IGRA) (e.g., QuantiFERON-TB Gold). TST not preferred on biologics. | Chest X-ray to exclude active TB. If latent TB diagnosed, commence TB prophylaxis (e.g., isoniazid for 6–9 months) BEFORE starting DMARD. | Higher prevalence in ATSI communities and migrants from high-burden countries. Refer to state/territory TB services. |
| Hepatitis B (HBV) | HBsAg, anti-HBs, anti-HBc. | If HBsAg positive: refer hepatology, consider antiviral prophylaxis (e.g., entecavir). If anti-HBc positive only: monitor HBV DNA. | Important in patients from high-prevalence regions (e.g., Asia-Pacific). |
| Hepatitis C | Anti-HCV antibody, HCV RNA if positive. | Treat HCV with DAA therapy if active. DMARDs can be used post-cure. | PBS-listed DAA therapy available. |
| Strongyloides | Strongyloides serology. | Treat with ivermectin (200 mcg/kg daily for 2 days) before immunosuppression. | Critical for patients who have lived in endemic areas (tropical QLD, NT, Pacific Islands, Southeast Asia). Risk of fatal hyperinfection syndrome. |
Methotrexate (Dosing, Monitoring, Folate)
Methotrexate (MTX) is the first-line anchor DMARD for rheumatoid arthritis and is used in many other inflammatory conditions. It is a folate antagonist with immunomodulatory effects.
Managing Common Issues
- Nausea/GI intolerance: Consider switching to subcutaneous injection, dose splitting (e.g., 2.5 mg every 12 hours x 3 doses weekly), or antiemetics.
- Elevated LFTs: Hold if transaminases >3x ULN. Re-check after 2–4 weeks. Consider dose reduction or cessation if persistent.
- Cytopenias: Hold for significant leucopenia or thrombocytopenia. Check for concurrent trimethoprim use (avoid).
- Pneumonitis: Rare. Suspect if new dry cough or dyspnoea. Stop MTX and investigate urgently.
Conventional Synthetic DMARDs (csDMARDs)
These are oral agents used as monotherapy or in combination (e.g., triple therapy: MTX + sulfasalazine + hydroxychloroquine).
TNF Inhibitors
Tumour Necrosis Factor (TNF) inhibitors were the first class of biologic DMARDs. They are first-line biologics for RA, psoriatic arthritis, and ankylosing spondylitis after csDMARD failure.
IL-6, IL-17, IL-23 Inhibitors
IL-6 Receptor Inhibitors (RA, GCA, JIA)
IL-17 Inhibitors (PsA, AS)
IL-23 Inhibitors (PsA)
JAK Inhibitors
Janus Kinase (JAK) inhibitors are oral targeted synthetic DMARDs that block intracellular signalling of multiple cytokines. They are used in RA, PsA, and AS.
Routine Monitoring on DMARDs
Consistent monitoring is essential for safety. Frequency is higher during initiation and dose changes.
| Test | Frequency (Stable) | Applies To | Action Thresholds |
|---|---|---|---|
| FBC (Full Blood Count) | Every 3 months | MTX, LEF, SSZ, JAKi | Hold for WCC <3.5 or Platelets <100. Review if Hb drops. |
| LFTs (ALT/AST) | Every 3 months | MTX, LEF, SSZ | Hold if >3x ULN. Recheck in 2–4 weeks. |
| eGFR/Creatinine | Every 3–6 months | All (dose adjustments needed) | Dose adjust per SPC. |
| Lipids | Baseline, 3 months, then annually | IL-6 inhibitors, JAK inhibitors | Manage per CV risk. |
| Blood Pressure | Every visit | JAK inhibitors | Manage hypertension. |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Rheumatic diseases, including rheumatic fever and rheumatic heart disease, have a higher prevalence and greater severity in Aboriginal and Torres Strait Islander communities, particularly in remote areas. Management with DMARDs requires a culturally safe, patient-centred approach.
📚 References
- 1. Ledingham J, Deighton C; British Society for Rheumatology Standards, Audit and Guidelines Working Group. Update on the British Society for Rheumatology guidelines for prescribing TNFα inhibitors in adults with rheumatoid arthritis (update of previous guidelines of April 2001). Rheumatology (Oxford). 2005;44(8):1018-1027.
- 2. Singh JA, Saag KG, Bridges SL Jr, et al. 2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis Rheumatol. 2016;68(1):1-26.
- 3. Fraenkel L, Bathon JM, England BR, et al. 2021 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis Care Res (Hoboken). 2021;73(7):924-939.
- 4. Smolen JS, Landewé RBM, Bijlsma JWJ, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheum Dis. 2023;82(1):3-18.
- 5. Australian Institute of Health and Welfare (AIHW). Rheumatoid arthritis. Cat. no. PHE 248. Canberra: AIHW; 2021.
- 6. Pharmaceutical Benefits Scheme (PBS). Australian Government Department of Health. PBS Schedule. Available at: https://www.pbs.gov.au.
- 7. Ytterberg SR, Bhatt DL, Mikuls TR, et al. Cardiovascular and Cancer Risk with Tofacitinib in Rheumatoid Arthritis. N Engl J Med. 2022;386(4):316-326.
- 8. Buch MH, Landewé R, Rubbert-Roth A, et al. Safety of JAK inhibitors in patients with rheumatoid arthritis and other inflammatory diseases. RMD Open. 2023;9(2):e003073.
- 9. The Royal Australian College of General Practitioners (RACGP). National guide to a preventive health assessment for Aboriginal and Torres Strait Islander people. 3rd edn. East Melbourne, Vic: RACGP; 2018.
- 10. RHDAustralia (Australian Government Department of Health). The Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd edition. 2020.
- 11. Australasian Society of Clinical Immunology and Allergy (ASCIA). Guidelines for vaccination of patients on immunosuppressive therapy. 2023.
- 12. Beglinger C, Dudler J, Lottaz D, et al. Strongyloides stercoralis hyperinfection in a patient with rheumatoid arthritis. Ann Rheum Dis. 2005;64(8):1223-1224.