📋 Key Information Summary
- Primary Indications: Arthrocentesis is indicated for acute monoarthritis to diagnose septic arthritis, crystal arthropathy, or haemarthrosis, and for therapeutic joint effusion drainage.
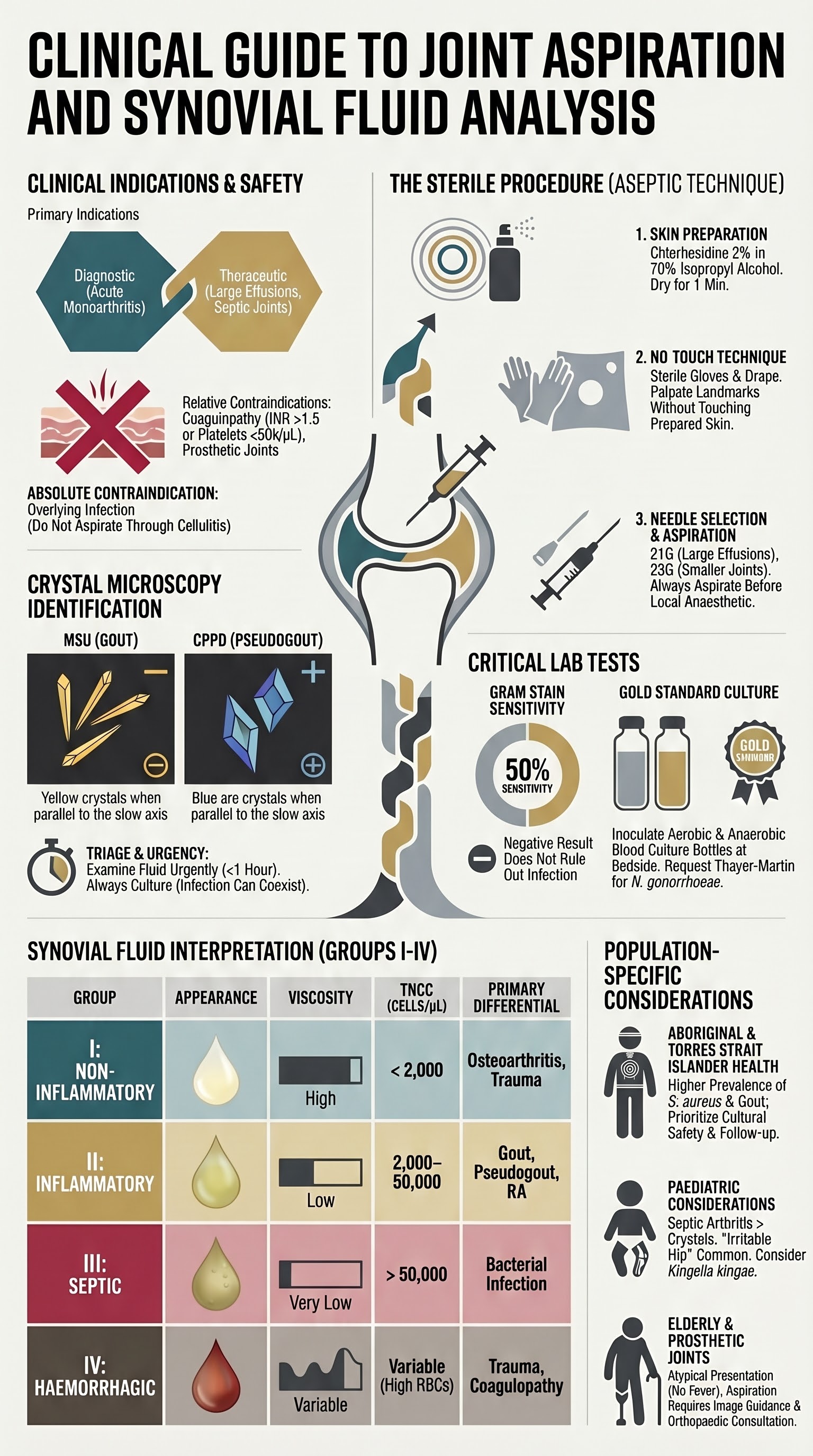
- Absolute Contraindications: Overlying cellulitis or bacteraemia; relative contraindications include coagulopathy (INR >1.5 or platelets <50,000/µL) and prosthetic joints without specialist consultation.
- Sterile Technique is Mandatory: Use a no-touch technique with chlorhexidine in alcohol preparation, sterile drape, and gloves to prevent iatrogenic septic arthritis.
- Synovial Fluid Analysis Triage: Immediately send fluid for: 1) Gram stain & culture (critical), 2) Crystal microscopy (polarised light), 3) Cell count with differential.
- Crystal Identification: Negatively birefringent, needle-shaped monosodium urate (MSU) crystals confirm gout. Weakly positively birefringent, rhomboid calcium pyrophosphate (CPPD) crystals confirm pseudogout.
- Fluid Appearance & Viscosity: Normal fluid is clear, pale yellow, and viscous. Turbid/cloudy suggests infection or inflammation; red/brown suggests trauma or haemorrhage.
- Cell Count Interpretation: Non-inflammatory (<2,000/µL), inflammatory (2,000–50,000/µL), septic (>50,000/µL, often >100,000/µL). Septic counts can occur in crystal arthropathy.
- Gram Stain & Culture: Gram stain has ~50% sensitivity for septic arthritis. Culture is gold standard. Fastidious organisms (e.g., Neisseria gonorrhoeae) require specific culture media.
- Pattern Interpretation (Group I-IV): Guides differential diagnosis: Group I (Non-inflammatory), Group II (Inflammatory), Group III (Septic), Group IV (Haemorrhagic).
- Special Considerations: Prosthetic joint aspiration often requires image guidance and is managed in consultation with orthopaedics/infectious diseases.
- ATSI Considerations: Higher prevalence of septic arthritis and gout; ensure timely access to procedure and follow-up in remote settings.
- Documentation & Safety: Document procedure details, fluid appearance, and tests sent. Use a time-out checklist. Send all fluid to lab if infection is suspected.
Introduction & Australian Epidemiology
Joint aspiration (arthrocentesis) and synovial fluid analysis is a critical diagnostic and therapeutic procedure in rheumatology and emergency medicine. It is the definitive investigation for differentiating septic arthritis from crystal arthropathy—two conditions that are medical emergencies with distinct treatments.
In Australia, acute monoarthritis is a common presentation. Gout prevalence is increasing, affecting ~5% of Australian men and ~1.5% of women. Septic arthritis, though less common (annual incidence ~5–10 per 100,000), carries significant morbidity (up to 30% mortality in elderly patients) and risk of permanent joint destruction if not promptly diagnosed and treated. Crystal arthropathy can coexist with infection, making synovial fluid analysis indispensable.
This guideline provides a comprehensive, evidence-based approach for Australian practitioners performing and interpreting arthrocentesis.
Indications & Contraindications
Indications
- Acute monoarthritis or oligoarthritis to differentiate septic arthritis, crystal arthropathy (gout, pseudogout), or inflammatory arthritis.
- Unexplained joint effusion.
- Evaluation of suspected haemarthrosis (e.g., trauma, coagulopathy).
- To obtain fluid for culture in suspected disseminated infection (e.g., meningococcal, N. gonorrhoeae).
- Drainage of a large, painful effusion for symptomatic relief.
- Aspiration prior to intra-articular corticosteroid injection.
- Decompression of a septic joint as an adjunct to systemic antibiotics.
Contraindications
Relative Contraindications (require risk-benefit analysis and often correction):
- Coagulopathy: INR >1.5 or platelet count <50,000/µL. Correct if possible; consider smaller needle (e.g., 22G).
- Prosthetic joint: High risk of seeding infection. Aspiration should only be performed by an experienced clinician, often with ultrasound guidance, and in consultation with the treating orthopaedic surgeon.
- Overlying skin lesion (psoriasis, dermatitis) that cannot be avoided by the needle track.
- Patient on anticoagulant/antiplatelet therapy: Weigh bleeding risk against diagnostic urgency. DOACs and warfarin increase risk; aspirin alone is not a major contraindication.
Sterile Technique
Strict aseptic technique is non-negotiable to prevent iatrogenic infection. Follow the RACGP-approved procedure checklist.
Crystal Microscopy (MSU, CPPD)
Crystal identification requires a compensated polarised light microscope. The fluid should be examined urgently, ideally within 1 hour, as crystals degrade.
| Crystal Type | Shape | Birefringence | Colour on Compensation | Diagnosis |
|---|---|---|---|---|
| Monosodium Urate (MSU) | Needle-shaped | Strong negative | Yellow when parallel to slow axis of red compensator | Gout |
| Calcium Pyrophosphate (CPPD) | Rhomboid / rod-shaped | Weak positive | Blue when parallel to slow axis | Pseudogout (CPPD disease) |
| Basic Calcium Phosphate (BCP) | Non-crystalline clumps | Non-birefringent | Not visible under polarised light | Calcific periarthritis, Milwaukee shoulder |
Cell Count & Differential
Perform cell count in an EDTA tube. The total nucleated cell count (TNCC) and differential are key for classification.
Important: TNCC in septic arthritis can sometimes be lower (e.g., 20,000–50,000/µL) in partially treated infections or with indolent organisms. Correlate with clinical context.
Gram Stain & Culture
This is the most critical test to rule out septic arthritis.
Group I-IV Pattern Interpretation
Integrating fluid appearance, viscosity, cell count, differential, and crystal findings leads to a pattern-based diagnosis.
| Group | Appearance | Viscosity | TNCC (/µL) | Predominant Cell | Crystals | Gram Stain/Culture | Primary Differential |
|---|---|---|---|---|---|---|---|
| I | Clear, pale yellow | High | <2,000 | Mononuclear | Negative | Negative | Osteoarthritis, Trauma |
| II | Cloudy, yellow-green | Low | 2,000–50,000 | Neutrophils (>50%) | Often positive (MSU/CPPD) | Negative | Gout, Pseudogout, RA |
| III | Turbid to purulent | Very low | >50,000 | Neutrophils (>75%) | May be present | Usually positive | Septic Arthritis |
| IV | Red/brown, xanthochromic | Variable | Variable | Mixed, with RBCs | Negative | Negative | Trauma, Coagulopathy, Tumour |
Key Synergy: A Group II fluid with MSU crystals confirms acute gout. A Group II fluid with CPPD crystals confirms acute pseudogout. A Group III fluid with crystals indicates concurrent septic arthritis and crystal arthropathy—treat both.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a higher burden of conditions requiring joint aspiration, including septic arthritis and gout. Cultural safety and addressing systemic barriers are paramount.
📚 References
- 1. Royal Australian College of General Practitioners (RACGP). A guide to understanding the investigation of joint pain in adults. East Melbourne: RACGP; 2020.
- 2. Australian Rheumatology Association (ARA). Gout: Management in general practice. Sydney: ARA; 2023.
- 3. Coakley G, Mathews C, Field M, et al. BSR & BHPR, BOA, RCGP and BSAC guidelines for management of the hot swollen joint in adults. Rheumatology. 2006;45(8):1039–1041.
- 4. Margaretten ME, Kohlwes J, Moore D, Bent S. Does this adult patient have septic arthritis? JAMA. 2007;297(13):1478–1488.
- 5. Swan A, Amer H, Dieppe P. The value of synovial fluid analysis in the diagnosis of joint disease. Ann Rheum Dis. 2002;61(6):493–498.
- 6. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 7. Jennings JM, Dennis DA, Kim RH, Miner TM, Yang CC, McNabb DC. AAOS Clinical Practice Guideline Summary: Management of Osteoarthritis of the Hip. J Am Acad Orthop Surg. 2022;30(4):e515–e520.
- 8. Tong SYC, Davis JS, Eichenberger E, Holland TL, Fowler VG. Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clin Microbiol Rev. 2015;28(3):603–661.
- 9. Aboriginal and Torres Strait Islander Health Team, Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework 2020 summary report. Canberra: AIHW; 2020.
- 10. RHDAustralia (a program of Menzies School of Health Research). 2022 Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine (ASHM) Guidelines for the management of acute rheumatic fever and rheumatic heart disease. Darwin: RHDAustralia; 2022.