📋 Key Information Summary
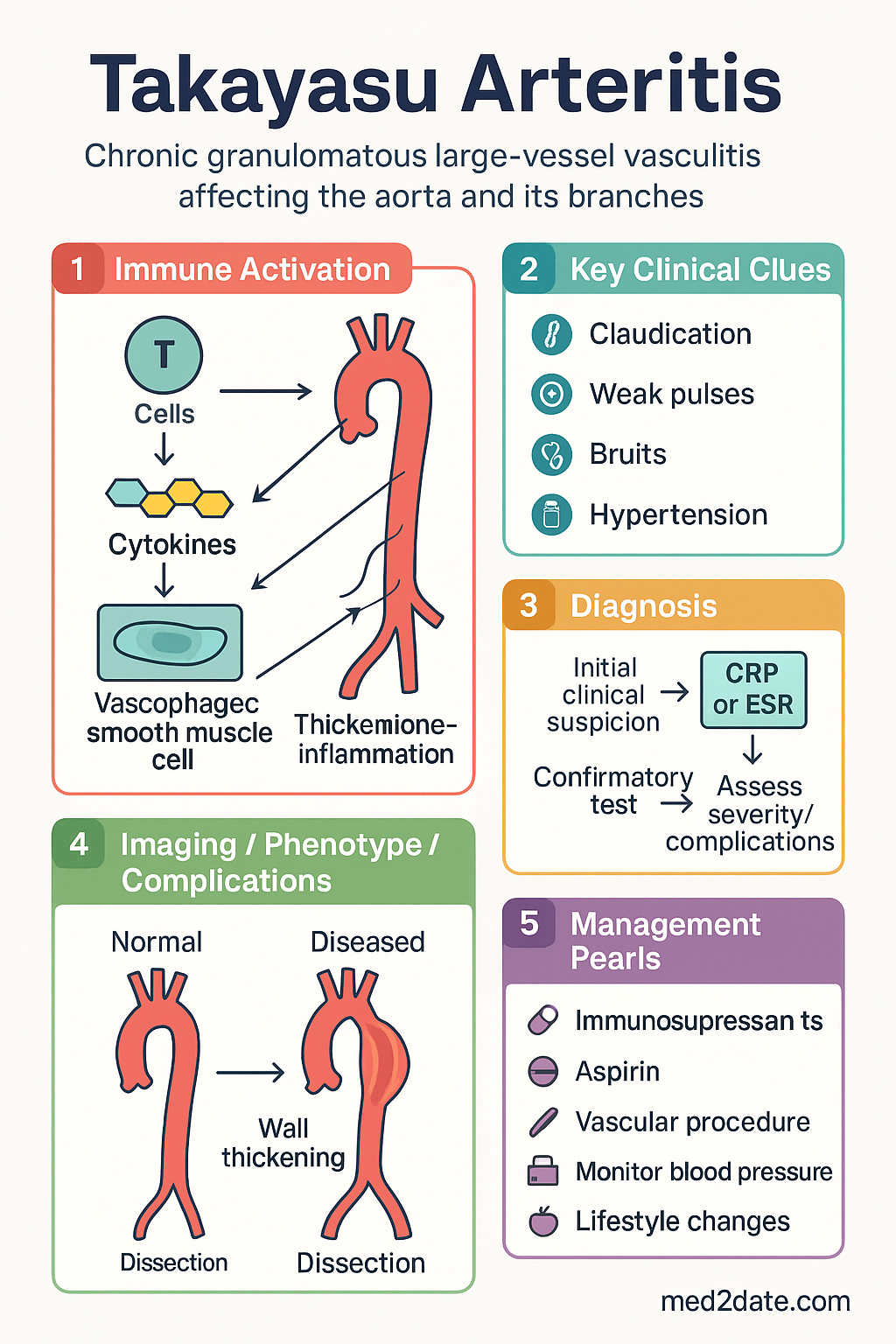
- Takayasu arteritis (TAK) is a chronic granulomatous large-vessel vasculitis predominantly affecting the aorta and its primary branches, causing progressive stenosis, occlusion, or aneurysm formation.
- Young women are predominantly affected — female-to-male ratio approximately 8:1, with peak onset between 15 and 30 years of age.
- Also known as "pulseless disease" — characteristic absent or diminished peripheral pulses, limb claudication, and blood pressure discrepancy between arms (>10 mmHg systolic difference).
- HLA-B52 association is well documented, particularly in Asian populations; also associated with increased disease severity and aortic regurgitation.
- ACR/EULAR 2022 classification criteria use a weighted scoring system (≥5 points = classified as TAK): age at onset ≤40 years, female sex, angina, limb claudication, arterial bruit, reduced pulse, BP discrepancy, and imaging findings.
- Numano angiographic classification (types I–VI) describes the pattern of vessel involvement and guides treatment planning and prognosis.
- Diagnosis requires cross-sectional imaging — CTA or MRA of the entire aorta showing concentric vessel wall thickening; FDG-PET may demonstrate active vascular inflammation before luminal changes appear.
- First-line therapy is high-dose corticosteroids — prednisolone 1 mg/kg/day (max 60 mg), with a slow taper over 6–12 months; relapse rate is high (60–80%) with steroids alone.
- Steroid-sparing agents are almost universally required — methotrexate (first-line conventional DMARD), azathioprine, or mycophenolate mofetil.
- Biologic agents for refractory disease — anti-TNF agents (infliximab, adalimumab) or tocilizumab (anti-IL-6R) are recommended when conventional DMARDs fail; both are PBS Authority Required in Australia.
- Revascularisation procedures (surgical bypass or endovascular angioplasty/stenting) should only be performed during stable clinical remission, ideally ≥6 months of quiescent disease on imaging.
- Indefinite immunosuppression is generally recommended given the high relapse risk on withdrawal; long-term cardiovascular risk management is essential.
- Aboriginal and Torres Strait Islander Australians may present with more advanced vascular damage at diagnosis; culturally safe, multidisciplinary care and remote access pathways are essential.
Introduction & Australian Epidemiology
Takayasu arteritis (TAK) is a chronic, granulomatous large-vessel vasculitis that predominantly affects the aorta and its primary branches. Progressive inflammation of the vessel wall leads to stenosis, occlusion, and — less commonly — aneurysm formation. The disease was first described by Mikito Takayasu in 1908, who noted retinal arteriovenous anastomoses in a young woman with absent radial pulses.
The clinical course typically progresses through three overlapping phases: (1) a systemic inflammatory (pre-pulseless) phase with constitutional symptoms such as fever, malaise, arthralgia, and weight loss; (2) a vascular inflammatory phase with arteritis causing vessel wall thickening and pain; and (3) a "burnt-out" or fibrotic phase characterised by fixed stenotic and occlusive lesions leading to ischaemic complications including limb claudication, renovascular hypertension, and cerebrovascular insufficiency.
Australian context: TAK is rare in Australia, with an estimated prevalence of 2–3 per million. However, it is the most common childhood-onset large-vessel vasculitis and carries significant morbidity if not diagnosed early. Australian tertiary vasculitis centres (e.g., Royal Adelaide Hospital, Monash Health, St Vincent's Hospital Melbourne) manage the majority of cases. The disease may be under-recognised in remote and Indigenous communities where access to specialist imaging and rheumatology services is limited.
Epidemiology & Classification
Epidemiology
TAK is rare in Western populations (incidence 1–3 per million per year) but more common in Asia, particularly Japan, India, China, and Southeast Asia, where incidence may reach 15–40 per million per year. It predominantly affects women (female-to-male ratio approximately 8:1) with a peak age of onset between 15 and 30 years. Disease onset after age 40 is uncommon and should prompt consideration of giant cell arteritis (GCA), particularly in patients of Northern European descent.
| Feature | Detail |
|---|---|
| Global prevalence | 4.7–26 per million (higher in Asia) |
| Australian prevalence | Estimated 2–3 per million |
| Female : Male ratio | 8 : 1 |
| Peak onset age | 15–30 years |
| Ethnic predominance | Asian > Hispanic > African > Caucasian |
| HLA association | HLA-B52 (especially Japanese, Korean populations) |
| 5-year survival (untreated) | ~80–90% |
| 10-year event-free survival | ~50–60% with treatment |
Genetic & Immunological Factors
HLA-B52 is the strongest genetic risk factor, particularly in East Asian populations, where it confers an odds ratio of approximately 3–5. HLA-B52-positive patients are more likely to have aortic regurgitation, systemic hypertension, and more extensive aortic involvement. Polymorphisms in IL-12B, FCGR2A, and TNFAIP3 have also been implicated in genome-wide association studies. The immunopathogenesis involves an initial innate immune response in the adventitia, with subsequent T-cell (particularly Th1 and Th17) mediated granulomatous inflammation propagating through the vessel wall.
ACR/EULAR 2022 Classification Criteria
The 2022 ACR/EULAR classification criteria replaced the earlier 1990 criteria and use a weighted additive scoring system. Patients with suspected vasculitis who score ≥5 points are classified as having TAK.
| Criterion | Points |
|---|---|
| Age at onset ≤40 years | +2 |
| Female sex | +1 |
| Angina or ischaemic pain | +2 |
| Limb claudication | +2 |
| Vascular bruit (subclavian/abdominal aorta) | +2 |
| Reduced/absent pulse, pulse asymmetry, or BP discrepancy ≥20 mmHg | +2 |
| Bilateral subclavian or axillary artery involvement on imaging | +3 |
| Concentric wall thickening of ≥2 large arteries on imaging | +1 |
| Involvement of ≥2 large-vessel territories | +1 |
| Saccular or fusiform aneurysm | +1 |
| Requires exclusion of other vasculitides, fibromuscular dysplasia, and IgG4-related disease | |
Numano Angiographic Classification
The Numano classification describes the anatomical pattern of vascular involvement and helps guide therapeutic and surgical planning:
| Type | Vessels Involved | Prevalence |
|---|---|---|
| Type I | Branches of the aortic arch | ~15–20% |
| Type IIa | Ascending aorta, aortic arch, and its branches | ~10–15% |
| Type IIb | Type IIa + descending thoracic aorta | ~15–20% |
| Type III | Descending thoracic aorta, abdominal aorta, and/or renal arteries | ~10–15% |
| Type IV | Abdominal aorta and/or renal arteries | ~15–20% |
| Type V | Combined features of types IIb and IV (entire aorta) | ~20–30% |
Type V disease is the most common pattern in Asian cohorts, whereas type I (branch vessel-only) disease may be more common in European series. The pattern of involvement influences complications — type IIa is associated with aortic regurgitation and coronary ostial stenosis, while types III–IV are more commonly associated with renovascular hypertension.
Pathophysiology
TAK is characterised by granulomatous inflammation of the vessel wall, primarily affecting the media and adventitia of the aorta and its major branches. The immunopathogenesis involves both innate and adaptive immune responses:
- Initiation: A triggering event (possibly infectious or mechanical stress at the aortic root) activates dendritic cells in the adventitia, producing IL-12, IL-18, and IL-6.
- Adaptive response: Activated dendritic cells promote Th1 (IFN-γ-producing) and Th17 (IL-17-producing) responses. Cytotoxic CD8+ T cells and natural killer (NK) cells contribute to vascular wall destruction.
- Vasa vasorum: Obliterative panarteritis of the vasa vasorum compromises nutrient supply to the vessel wall, accelerating tissue ischaemia and fibrosis.
- Vascular remodelling: Progressive intimal hyperplasia and adventitial fibrosis lead to luminal stenosis. Degradation of the elastic lamina may result in aneurysm formation.
- B-cell contribution: B-cell lymphoid neogenesis occurs within the vessel wall, and rituximab has shown efficacy in refractory cases, supporting a pathogenic role for B cells.
Clinical Features & Diagnostic Criteria
Three Phases of Disease
The clinical presentation of TAK progresses through overlapping phases, although not all patients experience a recognisable systemic prodrome:
Clinical Features by Vascular Territory
| Territory | Manifestation | Frequency |
|---|---|---|
| Subclavian/axillary | Upper limb claudication, absent/radial pulse, BP discrepancy >10 mmHg, Raynaud-like symptoms | 80–90% |
| Carotid/vertebral | Carotidyngia, bruits, TIA, stroke, visual disturbances, dizziness | 50–60% |
| Renal arteries | Renovascular hypertension (often severe and resistant), renal impairment | 30–40% |
| Ascending aorta/aortic root | Aortic regurgitation, aortitis, coronary ostial stenosis | 20–30% |
| Descending/abdominal aorta | Abdominal aortic aneurysm, mesenteric ischaemia, lower limb claudication | 40–60% |
| Pulmonary arteries | Pulmonary hypertension, pulmonary artery stenosis (often asymptomatic) | 15–20% |
Key Examination Findings
- Blood pressure discrepancy: Systolic BP difference ≥10 mmHg between arms — perform bilateral BP measurement in all suspected cases.
- Pulse deficits: Absent, diminished, or delayed radial, brachial, or carotid pulses.
- Arterial bruits: Listen over the carotid, subclavian, abdominal aorta, and femoral arteries.
- Carotidyngia: Palpable tenderness over the carotid arteries — a distinguishing feature from atherosclerotic disease.
- Aortic regurgitation murmur: Early diastolic murmur at the left sternal border in type IIa disease.
Investigations
Laboratory Investigations
Imaging
Risk Stratification & Disease Activity Assessment
Assessment of Disease Activity
Disease activity assessment in TAK is challenging because traditional inflammatory markers (ESR, CRP) may be normal despite active disease, and established vascular damage does not improve with immunosuppression. Multiple tools should be used in combination:
| Tool | Details | Limitations |
|---|---|---|
| ITAS2010 | Indian Takayasu Clinical Activity Score — 44 items; ITAS-A includes ESR. Active disease: ITAS ≥1 or ITAS-A ≥2 | May over-score irreversible damage |
| Kerr criteria | ≥2 of: systemic symptoms, elevated ESR, new/worsening claudication, new bruit, new BP discrepancy, new pulse deficit | Lower sensitivity for subclinical activity |
| DEI-TAK | Disease Extent Index for TAK — assesses extent of vascular involvement | Measures extent not activity |
| Imaging | Vessel wall oedema on MRI, FDG uptake on PET, new/worsening lesions on CTA/MRA | FDG-PET availability; radiation with serial CTA |
Factors Predicting Relapse
- Young age at onset (<20 years)
- Type V (extensive) disease
- Involvement of the ascending aorta or aortic root
- Elevated CRP at time of apparent remission
- Persistent vessel wall oedema on MRI
- Rapid corticosteroid taper
Empirical & First-Line Therapy
Induction — Corticosteroids
High-dose corticosteroids are the cornerstone of initial therapy and produce remission in approximately 50–60% of patients as monotherapy. However, relapse rates on steroid taper are high (60–80%), and steroid-sparing agents should be started early.
Steroid-Sparing Agents — Conventional DMARDs
Conventional DMARDs should be co-initiated with corticosteroids in virtually all patients given the high relapse rate. The choice depends on patient factors including pregnancy planning, hepatic function, and thiopurine methyltransferase (TPMT) status.
Directed / Biologic Therapy for Refractory Disease
For patients who relapse on or fail to respond to conventional DMARDs, biologic agents targeting TNF-α or IL-6 receptor have demonstrated efficacy. There is no randomised head-to-head trial; choice is based on comorbidities, patient preference, and PBS access.
Monitoring & Follow-Up
Routine Monitoring Schedule
| Parameter | Frequency | Notes |
|---|---|---|
| ESR, CRP | Every 1–3 months (active disease); every 3–6 months (remission) | Normal values do not exclude active disease |
| FBC, LFTs, UEC | Monthly initially with DMARDs; every 2–3 months once stable | DMARD toxicity monitoring |
| Bilateral blood pressure | Every visit | Document arm used; monitor discrepancy |
| Pulse examination | Every visit | Record all palpable pulses; note new deficits |
| Vascular imaging (CTA or MRA) | Every 6–12 months (active); annually (remission) | MRA preferred to minimise radiation in young patients |
| Echocardiography | Annually | Assess aortic regurgitation, root dilation |
| FDG-PET (if available) | When clinical/imaging discordance | Detect subclinical inflammation |
| DEXA scan | Baseline and annually if on prednisolone >5 mg | Osteoporosis prevention |
| Cardiovascular risk assessment | Annually | Lipids, HbA1c, smoking status, Framingham risk |
Definition of Remission
Complete remission in TAK requires: (1) absence of systemic symptoms attributable to active vasculitis; (2) no new vascular symptoms (claudication, pulse deficits, BP discrepancy); (3) normalisation or stable/improving inflammatory markers (ESR, CRP); and (4) absence of new/worsening vascular lesions on imaging.
Surgical & Endovascular Revascularisation
Vascular intervention is indicated for critical stenoses causing symptomatic ischaemia (limb-threatening, cerebrovascular, renovascular hypertension refractory to medical therapy). Procedures should only be performed during stable clinical and serological remission — ideally ≥6 months of disease quiescence — as intervention during active inflammation carries a high risk of restenosis and graft failure.
Interventional Options
| Procedure | Indication | Considerations |
|---|---|---|
| Surgical bypass grafting | Long-segment occlusions, aortic arch syndrome, complex renovascular disease | Higher durability than endovascular; requires expertise in large-vessel surgery; use autologous vein where possible |
| Percutaneous transluminal angioplasty (PTA) | Short-segment stenoses (especially renal arteries) | Lower procedural risk; higher restenosis rate than surgery; avoid stenting in inflamed vessel wall |
| Aortic valve replacement | Severe aortic regurgitation | Mechanical vs bioprosthetic valve — use a bioprosthesis if future immunosuppression is planned |
| Endovascular aortic repair (EVAR/TEVAR) | Aortic aneurysm | May be suitable for anatomically favourable aneurysms; long-term data limited in TAK |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
While large-vessel vasculitis data specific to Aboriginal and Torres Strait Islander populations are limited, there are important considerations for equitable and culturally safe care in the Australian context.
📚 References
- 1. Grayson PC, Alehashemi S, Bagheri AA, et al. 2022 American College of Rheumatology/EULAR classification criteria for Takayasu arteritis. Ann Rheum Dis. 2022;81(12):1654–1660.
- 2. Misra DP, Wakhlu A, Agarwal V, Danda D. Recent advances in the management of Takayasu arteritis. Int J Rheum Dis. 2019;22(Suppl 1):54–59.
- 3. Tombetti E, Mason JC. Takayasu arteritis: advanced understanding is leading to new horizons. Rheumatology (Oxford). 2019;58(Suppl 4):iv41–iv52.
- 4. Nakaoka Y, Isobe M, Tanaka Y, et al. Long-term efficacy and safety of tocilizumab in refractory Takayasu arteritis: final results of the randomized controlled phase 3 TAKT trial. Rheumatology (Oxford). 2020;59(9):2427–2434.
- 5. Langford CA, Cuthbertson D, Ytterberg SR, et al. A randomized, double-blind trial of abatacept (CTLA-4-Ig) for the treatment of Takayasu arteritis. Arthritis Rheumatol. 2017;69(4):846–853.
- 6. Hoffman GS, Leavitt RY, Kerr GS, Rottem M, Sneller MC, Fauci AS. Treatment of glucocorticoid-resistant or relapsing Takayasu arteritis with methotrexate. Arthritis Rheum. 1994;37(4):578–582.
- 7. Mekinian A, Biard L, Dagna L, et al. Efficacy and safety of TNF-α antagonists and tocilizumab in Takayasu arteritis: multicentre retrospective study. J Autoimmun. 2022;128:102801.
- 8. Association Suisse Romande de Rhumatologie (Swiss) and European Takayasu arteritis consensus. Mason JC. Takayasu arteritis — surgical interventions. Best Pract Res Clin Rheumatol. 2009;23(3):365–376.
- 9. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Aboriginal and Torres Strait Islander people. AIHW Cardiovascular disease series. Canberra: AIHW; 2023.
- 10. Hellmich B, Agueda A, Monti S, et al. 2018 update of the EULAR recommendations for the management of large vessel vasculitis. Ann Rheum Dis. 2020;79(1):19–30.
-