📋 Key Information Summary
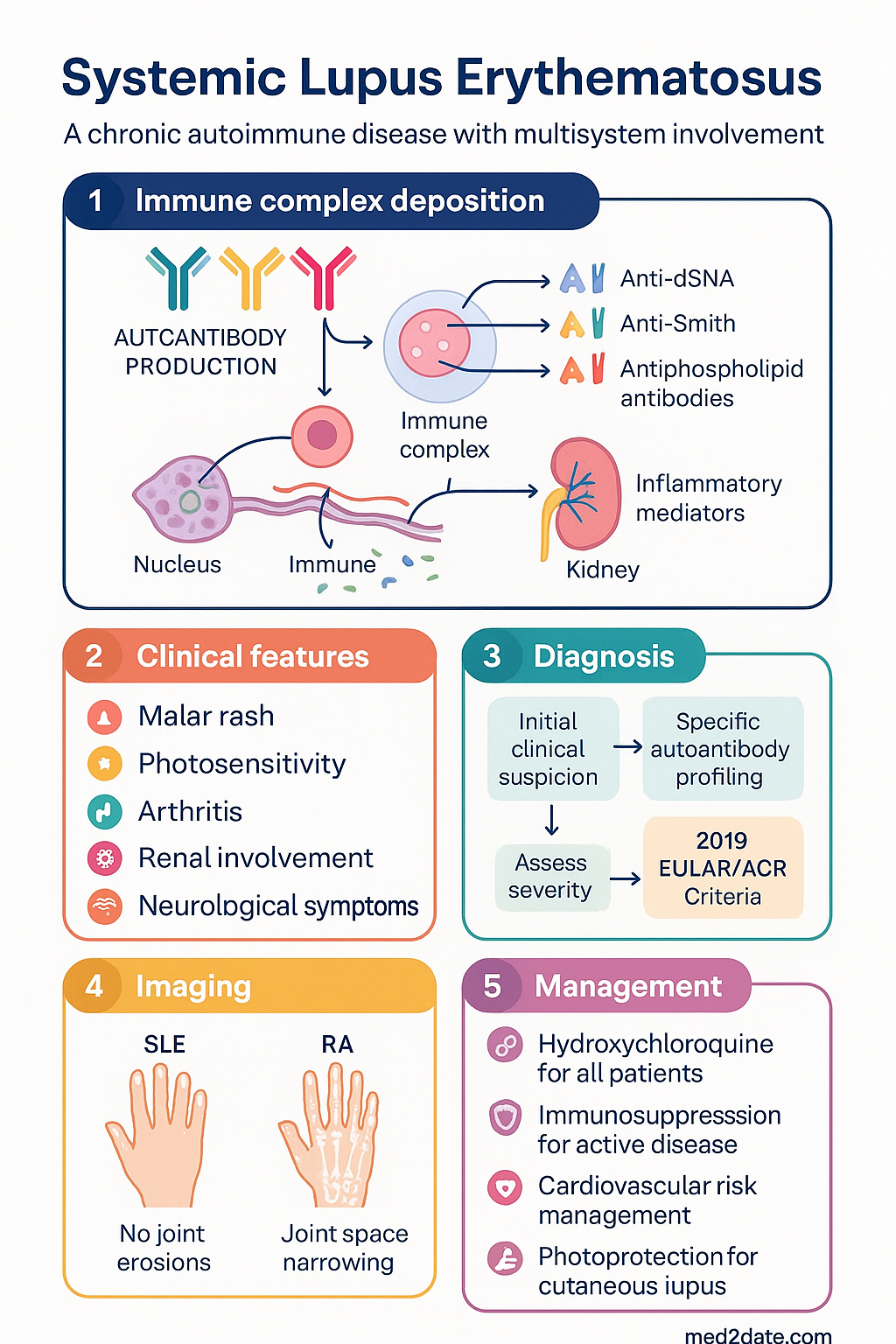
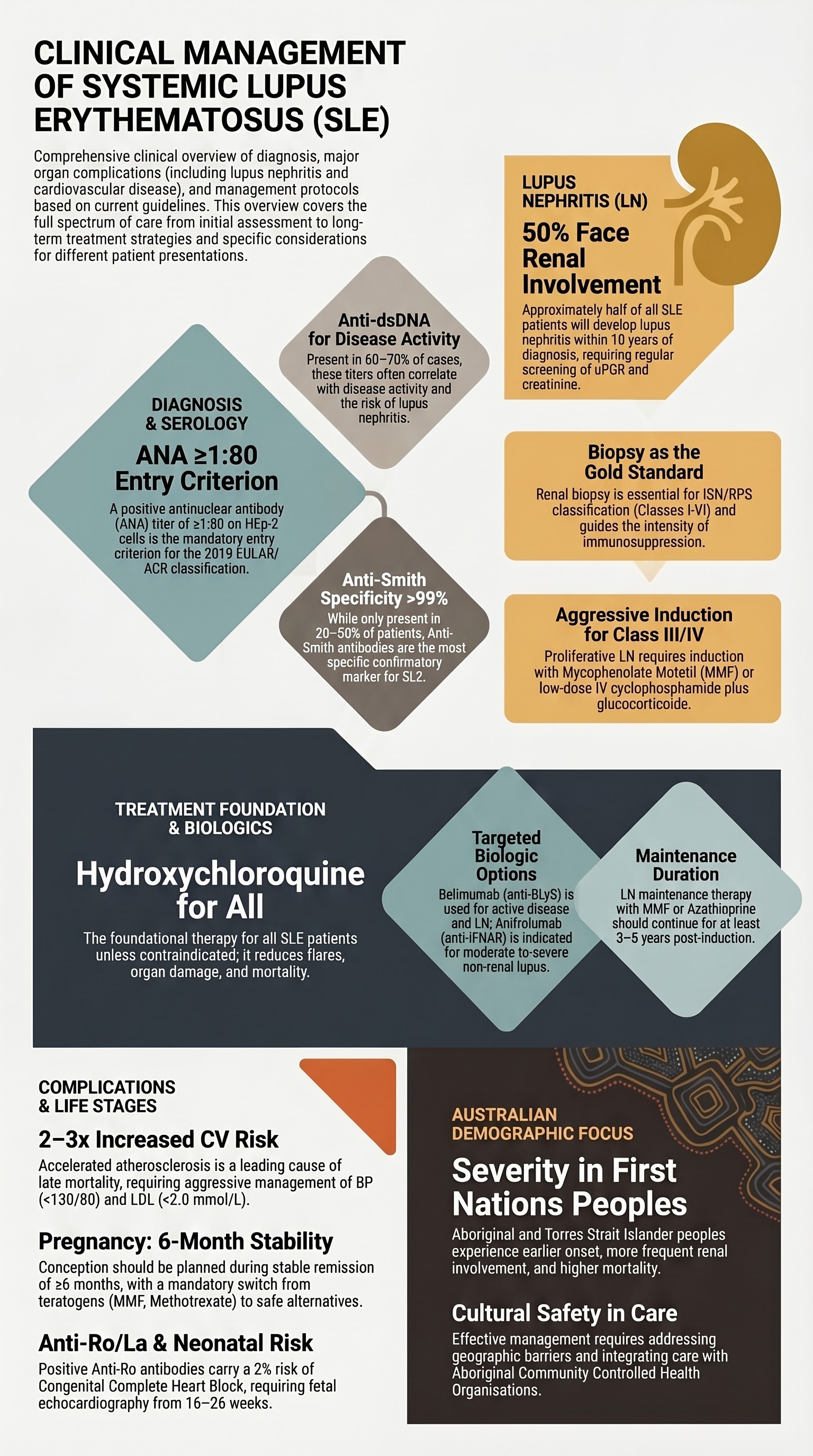
- Diagnosis: Based on 2019 EULAR/ACR criteria (ANA titre ≥1:80 is an entry criterion). No single pathognomonic test.
- Key Antibodies: Anti-dsDNA (disease activity, nephritis risk), Anti-Smith (highly specific), Anti-Ro/La (neonatal lupus, photosensitivity), Anti-RNP (mixed connective tissue disease overlap).
- Lupus Nephritis (LN): Occurs in ~50% of patients. Biopsy is gold standard for classification (ISN/RPS) and guides therapy. Class III/IV (±V) require aggressive immunosuppression.
- Induction Therapy for Active LN: Mycophenolate mofetil (MMF) or low-dose Euro-Lupus IV cyclophosphamide, PLUS glucocorticoids. Belimumab is an add-on option for active LN.
- Maintenance for LN: MMF or azathioprine for at least 3–5 years post-induction.
- Cutaneous Lupus: First-line is photoprotection (broad-spectrum SPF 50+). Topical calcineurin inhibitors or corticosteroids for localised disease. Hydroxychloroquine is first-line systemic agent.
- Pregnancy: Hydroxychloroquine should be continued. Plan pregnancy during stable remission (≥6 months). Avoid MMF, cyclophosphamide, methotrexate. Screen for anti-Ro/La antibodies (risk of congenital heart block).
- CV Risk: Accelerated atherosclerosis is a major cause of late mortality. Aggressive management of traditional risk factors (BP, lipids, smoking) is essential.
- Immunosuppression Backbone: Hydroxychloroquine for all patients unless contraindicated. Reduces flares, organ damage, thrombosis, and mortality.
- Biologics: Belimumab (anti-BLyS) for active disease despite standard therapy. Anifrolumab (anti-IFNAR) for moderate-severe non-renal lupus. Rituximab (off-label) for refractory cases.
- ATSI Considerations: Higher incidence and severity, particularly in younger patients. Barriers include remote access to specialist care and lower rates of renoprotective therapy.
- Vaccination: All patients should receive influenza and pneumococcal vaccines. Live vaccines are contraindicated on immunosuppression.
Introduction & Australian Epidemiology
Systemic Lupus Erythematosus (SLE) is a chronic, multisystem autoimmune disease characterised by the production of pathogenic autoantibodies and immune complex deposition, leading to inflammation and tissue damage. It follows a relapsing-remitting course with considerable heterogeneity in presentation and prognosis.
In Australia, the estimated prevalence is approximately 45–100 per 100,000 people. It disproportionately affects women (female:male ratio ~9:1) and individuals of non-European ancestry. Aboriginal and Torres Strait Islander peoples experience a higher incidence, earlier onset, more severe organ involvement (especially renal), and increased mortality compared to non-Indigenous Australians. The disease has a significant impact on quality of life and life expectancy, primarily due to active disease flares, infections from immunosuppression, and accelerated cardiovascular disease.
ANA & Autoantibody Patterns
A positive antinuclear antibody (ANA) test at a titre of ≥1:80 on HEp-2 cells is an entry criterion for the 2019 EULAR/ACR classification. However, ANA can be positive in other conditions and in ~15% of healthy individuals, so it is not diagnostic alone. Specific autoantibody profiling is crucial for diagnosis, prognostication, and monitoring.
| Antibody | Prevalence in SLE | Clinical Significance |
|---|---|---|
| Anti-dsDNA | 60–70% | Highly specific. Titres often correlate with disease activity, especially lupus nephritis. Can be used for monitoring. |
| Anti-Smith (Sm) | 20–30% | Most specific for SLE (>99%). Not associated with a particular manifestation but confirms diagnosis. |
| Anti-Ro (SSA) / Anti-La (SSB) | 30–40% / 10–15% | Associated with photosensitive cutaneous lupus, neonatal lupus, and congenital heart block. Can be present in ANA-negative SLE. |
| Anti-RNP | 25–40% | High titres associated with Mixed Connective Tissue Disease (MCTD) overlap (Raynaud's, swollen hands, myositis). |
| Anti-ribosomal P | 10–20% | Associated with lupus psychosis and depression. |
| Antiphospholipid Antibodies (aPL) | 30–40% | Lupus anticoagulant, anti-cardiolipin, anti-β2 glycoprotein I. Confers risk of arterial/venous thrombosis and obstetric complications. |
Lupus Nephritis (LN)
LN is a major cause of morbidity and mortality. It occurs in approximately 50% of SLE patients within 10 years of diagnosis. Early detection and aggressive treatment are critical to prevent end-stage kidney disease (ESKD).
Diagnosis & Classification
Screen with urine microscopy, urine protein:creatinine ratio (uPCR) and serum creatinine/eGFR at diagnosis and regularly thereafter. A renal biopsy is indicated for persistent proteinuria (uPCR >50 mg/mmol), active urinary sediment, or unexplained rise in creatinine. Biopsy is classified using the ISN/RPS system:
| ISN/RPS Class | Description | General Treatment Approach |
|---|---|---|
| I, II | Minimal mesangial / Mesangial proliferative | Treat systemic symptoms; usually no specific nephritis therapy needed. |
| III | Focal proliferative | Requires induction immunosuppression. |
| IV | Diffuse proliferative (most severe) | Requires intensive induction immunosuppression. |
| V | Membranous | Treat if nephrotic-range proteinuria. Often combined with III or IV. |
| VI | Advanced sclerosing | ESKD likely; immunosuppression usually futile. Supportive care. |
Management of Proliferative LN (Class III/IV)
Induction Therapy (3–6 months): Aim to control active inflammation.
Add-on Biologic: Belimumab can be added to standard therapy (MMF or azathioprine) for active LN to improve renal response and reduce flares.
Maintenance Therapy (≥3–5 years): After successful induction, switch to lower-dose oral therapy to prevent relapse.
Supportive Care in LN
- Hydroxychloroquine: Continue for all LN patients (reduces flares, thrombosis, and improves survival).
- Renin-Angiotensin System Blockade: ACE inhibitor or ARB for proteinuria >0.5 g/day, regardless of blood pressure.
- Cardiovascular Risk Reduction: Statin therapy, BP control (<130/80 mmHg).
- Infection Prophylaxis: Consider PJP prophylaxis (e.g., trimethoprim-sulfamethoxazole) during intensive immunosuppression, especially with cyclophosphamide.
Cutaneous Lupus
Cutaneous manifestations occur in >80% of SLE patients. They are broadly categorised as acute (e.g., malar rash), subacute (photosensitive, annular polycyclic lesions), or chronic (discoid lupus).
General Principles
- Photoprotection: Cornerstone of management. Broad-spectrum SPF 50+ sunscreen, protective clothing, and sun avoidance. Reapply sunscreen every 2 hours.
- Smoking Cessation: Smoking worsens cutaneous lupus and reduces response to hydroxychloroquine.
Pharmacological Therapy
First-line Systemic:
Second-line Systemic (if inadequate response to HCQ):
- Methotrexate: 7.5–25 mg once weekly PO/SC, with folic acid. Effective for inflammatory arthritis and cutaneous disease.
- Belimumab: Can be effective for mucocutaneous manifestations.
- Thalidomide/Lenalidomide: For refractory severe cutaneous lupus. Specialist use only due to neuropathy/teratogenicity risk.
Topical Therapy:
- Potent topical corticosteroids (e.g., mometasone furoate 0.1%) for limited duration (2–4 weeks) for active lesions.
- Topical calcineurin inhibitors (tacrolimus 0.1% ointment, pimecrolimus cream) for sensitive areas (face) and maintenance.
Pregnancy & Neonatal Lupus
Pregnancy in SLE requires careful planning and multidisciplinary care (rheumatology, obstetrics, neonatology). Outcomes are best when conception occurs during stable remission (≥6 months).
Pre-Conception Counselling & Medication Management
Anti-Ro/La Antibodies & Neonatal Lupus
All pregnant SLE patients should be screened for anti-Ro (SSA) and anti-La (SSB) antibodies. These antibodies can cross the placenta and cause:
- Congenital Complete Heart Block (CCHB): Risk ~2% in anti-Ro positive mothers (higher in subsequent pregnancies). Requires fetal echocardiography from 16–26 weeks gestation. First-degree block may be reversible with dexamethasone.
- Neonatal Lupus Syndrome: Transient rash, cytopenias, hepatitis. Usually self-resolves by 6–8 months as maternal antibodies clear.
Monitoring During Pregnancy
- Monthly disease activity assessment (SLEDAI).
- Regular urine PCR, blood pressure, complement (C3/C4), and anti-dsDNA monitoring (note: complement naturally rises in pregnancy).
- Screen for antiphospholipid antibodies (lupus anticoagulant, anticardiolipin, anti-β2GPI) – presence alters management (requires LMWH + aspirin).
Immunosuppression & Biologics
Treatment is tailored to disease severity and organ involvement. Hydroxychloroquine forms the foundational therapy for all patients.
Biologic Therapies (PBS Listed)
Off-label Biologics
Rituximab: Anti-CD20 B-cell depletor. Used off-label for refractory lupus, particularly severe LN, neuropsychiatric lupus, and autoimmune cytopenias. Dose: 1000 mg IV x 2 doses (2 weeks apart). Requires specialist initiation and monitoring.
Other Conventional Agents
Cardiovascular Risk in SLE
Cardiovascular disease (CVD) is a leading cause of late mortality in SLE. Patients have a 2–3 fold increased risk of atherosclerotic events due to a combination of chronic inflammation, traditional risk factors, corticosteroid use, and renal involvement.
Risk Factors
- Disease-Related: High disease activity, lupus nephritis, antiphospholipid antibodies, elevated type I interferon signature.
- Treatment-Related: Cumulative glucocorticoid dose, NSAID use.
- Traditional: Hypertension, dyslipidaemia, diabetes, smoking, obesity, sedentary lifestyle.
Management Strategies
- Blood Pressure: Target <130/80 mmHg. Use ACEi/ARB as first-line, especially with proteinuria.
- Antiplatelet/Anticoagulation: Low-dose aspirin for patients with antiphospholipid antibodies and no history of thrombosis. Full anticoagulation (usually warfarin, target INR 2.0–3.0) for definite antiphospholipid syndrome.
- Minimise Glucocorticoids: Aim for prednisolone ≤7.5 mg/day or, ideally, cessation.
- Lifestyle: Smoking cessation, regular aerobic exercise, Mediterranean-style diet, weight management.
Aboriginal and Torres Strait Islander Health
SLE disproportionately and severely affects Aboriginal and Torres Strait Islander peoples. Key considerations for clinical practice:
📚 References
- 1. Fanouriakis A, Kostopoulou M, Alunno A, et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann Rheum Dis. 2019;78(6):736-745.
- 2. Gordon C, Amissah-Arthur MB, Gayed M, et al. The British Society for Rheumatology guideline for the management of systemic lupus erythematosus in adults. Rheumatology (Oxford). 2018;57(1):e1-e45.
- 3. Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int. 2021;100(4S):S1-S276.
- 4. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework 2020 summary report. Canberra: AIHW; 2020.
- 5. Tiao J, Feng R, Carr K, et al. The prevalence of lupus in Indigenous Australians: A systematic review. Semin Arthritis Rheum. 2022;56:152063.
- 6. Choi MY, Bhatt DO, Costenbader KH. Cardiovascular disease in systemic lupus erythematosus: an update. Curr Opin Rheumatol. 2022;34(2):97-104.
- 7. Andreoli L, Bertsias GK, Agmon-Levin N, et al. EULAR recommendations for women's health and the management of family planning, assisted reproduction, pregnancy and menopause in patients with systemic lupus erythematosus and/or antiphospholipid syndrome. Ann Rheum Dis. 2017;76(3):476-485.
- 8. Furie R, Rovin BH, Houssiau F, et al. Two-Year, Randomized, Controlled Trial of Belimumab in Lupus Nephritis. N Engl J Med. 2020;383(12):1117-1128.
- 9. Morand EF, Furie R, Tanaka Y, et al. Trial of Anifrolumab in Active Systemic Lupus Erythematosus. N Engl J Med. 2020;382(3):211-221.
- 10. RACGP/Arthritis Australia. Musculoskeletal Care Guide for General Practice. East Melbourne: RACGP; 2023.
- 11. National Health and Medical Research Council (NHMRC). Australian guidelines for the prevention and control of infection in healthcare. Canberra: NHMRC; 2019.
- 12. Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook. Australian Government Department of Health, Canberra.