📋 Key Information Summary
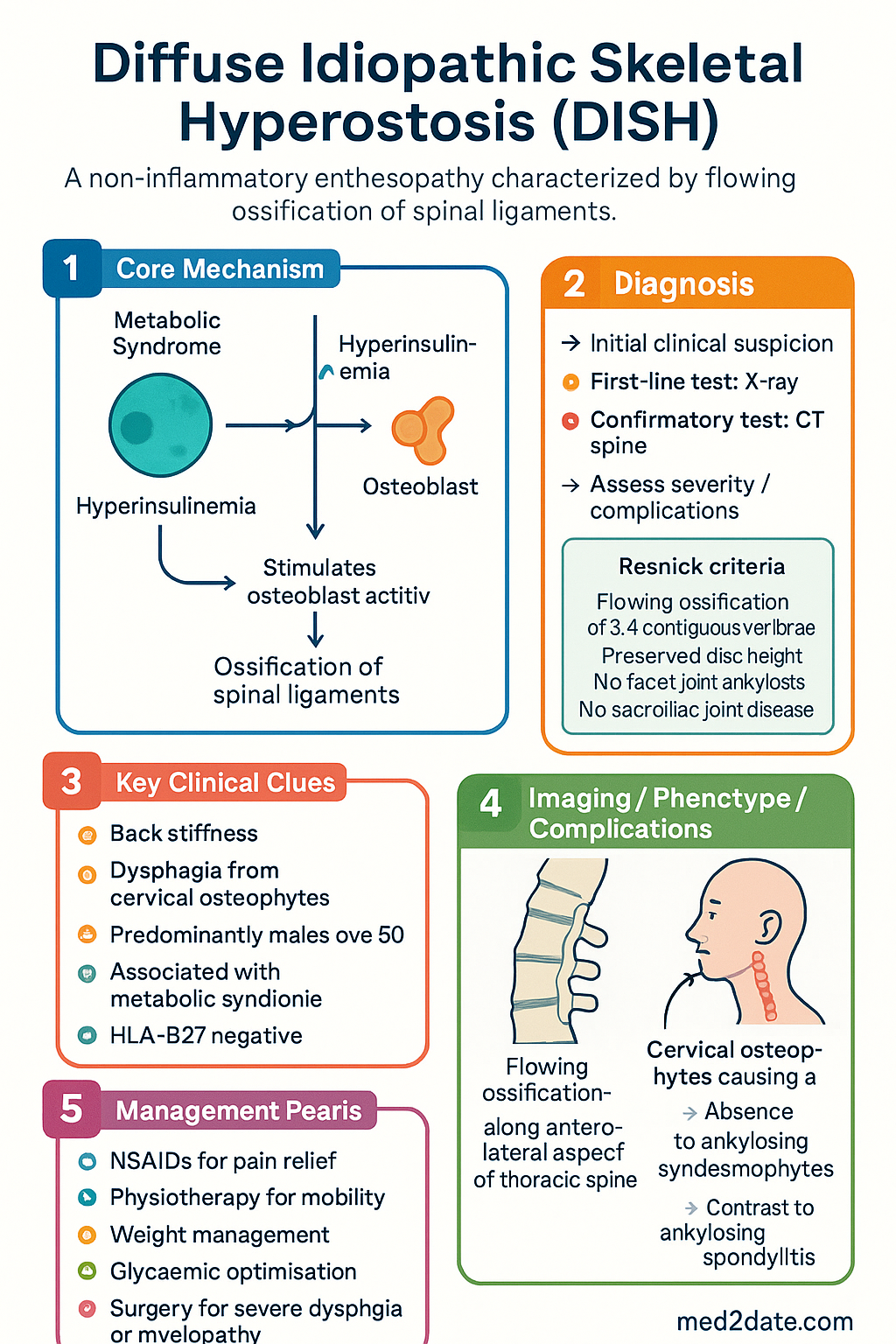
- DISH is a non-inflammatory enthesopathy characterised by flowing ossification of spinal ligaments, predominantly the right anterolateral thoracic spine.
- Resnick criteria (X-ray): flowing calcification/ossification ≥4 contiguous vertebrae, preserved disc height, no facet joint ankylosis, no sacroiliac joint disease.
- Predominantly affects males >50 years (2:1 male-to-female ratio); prevalence 6–12% in the elderly Australian population.
- Strongly associated with metabolic syndrome — obesity, type 2 diabetes mellitus, hyperinsulinaemia — which stimulates osteoblast activity via IGF-1 pathways.
- HLA-B27 is characteristically negative, helping differentiate DISH from ankylosing spondylitis (AS).
- Distinguishing features from AS: older age of onset, no sacroiliitis, no syndesmophytes, no anterior uveitis/IBD/psoriasis comorbidity, preserved disc spaces.
- Back stiffness in DISH is typically <30 minutes duration, unlike the >30-minute morning stiffness of AS.
- Cervical DISH may cause progressive dysphagia from anterior osteophyte compression of the oesophagus — a key extraspinal complication.
- Posterior cervical osteophytes can cause myelopathy requiring urgent surgical assessment.
- Management is primarily conservative: NSAIDs for pain, physiotherapy, weight management, and glycaemic optimisation.
- Surgery is reserved for refractory dysphagia, airway compromise, or progressive neurological deficit.
- Retinoid (vitamin A analogue) use is an additional risk factor; medication history should be reviewed in suspected cases.
Epidemiology & Pathogenesis
Demographics & Prevalence
- Age: Predominantly affects individuals >50 years; rare before age 40.
- Sex: Male-to-female ratio approximately 2:1; post-menopausal women increasingly affected.
- Ethnicity: Described across all ethnic groups; prevalence may be higher in populations with greater metabolic syndrome burden.
- Prevalence: 6–12% in Australian adults >50 years; up to 25–28% in males >80 years on imaging studies.
Pathogenic Mechanisms
The pathogenesis of DISH involves a complex interplay of metabolic, mechanical, and genetic factors:
| Pathogenic Factor | Mechanism | Clinical Relevance |
|---|---|---|
| Hyperinsulinaemia / T2DM | Insulin and IGF-1 stimulate osteoblast proliferation, differentiation, and matrix mineralisation | Most consistently identified metabolic risk factor; glycaemic control may modulate progression |
| Obesity | Mechanical loading on entheses; adipokine-mediated inflammation promoting ossification | BMI >30 kg/m² is an independent risk factor; weight management is cornerstone therapy |
| Hyperuricaemia / Gout | Crystal deposition may promote entheseal ossification; elevated prevalence in DISH cohorts | Uric acid should be checked; concurrent gout management recommended |
| Retinoid use | Vitamin A and synthetic retinoids (isotretinoin, acitretin, etretinate) promote ectopic ossification of ligaments | Medication review essential; isotretinoin (for acne) and acitretin (for psoriasis) are common Australian exposures |
| Mechanical stress | Repetitive microtrauma at entheses stimulates osteogenesis via BMP and Wnt pathways | Right-sided thoracic predominance explained by aortic shielding on left |
| Genetic predisposition | Familial clustering noted; specific gene loci under investigation; HLA-B27 is characteristically negative | No specific genetic testing indicated; HLA-B27 negativity distinguishes from AS |
Metabolic Syndrome — The Central Driver
The link between hyperinsulinaemia and DISH is the most robustly supported pathogenic association. Insulin and insulin-like growth factor 1 (IGF-1) act directly on osteoblast precursors through the PI3K/Akt and MAPK signalling cascades, promoting:
- Osteoblast proliferation and differentiation
- Type I collagen synthesis and matrix deposition
- Alkaline phosphatase activity and mineralisation
- Entheseal new bone formation at ligament–bone junctions
Clinical Features & Diagnosis
Symptomatic Presentation
Many patients with radiographic DISH are asymptomatic. When symptomatic, the following features are characteristic:
- Back stiffness: Typically <30 minutes, worse in the morning or after inactivity. This contrasts with AS where morning stiffness characteristically exceeds 30 minutes and improves with activity.
- Reduced spinal mobility: Progressive loss of thoracic rotation and lateral flexion; may be disproportionate to radiographic findings.
- Mild–moderate back pain: Usually dull, aching; less inflammatory in character than AS. Night pain is uncommon unless fracture is present.
- Extraspinal enthesopathy: Calcification at olecranon, patellar, Achilles, and plantar fascia entheses. Pelvic enthesophytes (iliac crest, ischial tuberosity) are common.
- Dysphagia: Occurs in cervical DISH when large anterior osteophytes compress or distort the oesophagus. Typically progressive for solid foods; may progress to liquids.
- Hoarseness / globus sensation: From laryngeal compression or recurrent laryngeal nerve irritation.
- Myelopathy / radiculopathy: Posterior cervical osteophytes or ossified posterior longitudinal ligament (OPLL) may compress the spinal cord or nerve roots, causing progressive limb weakness, numbness, or bladder dysfunction.
- Dysphonia and airway compromise: Rare but life-threatening; requires urgent ENT and surgical assessment.
Radiographic Diagnosis — Resnick Criteria
The diagnosis of DISH is primarily radiographic. The Resnick and Niwayama criteria (1976) remain the gold standard and require all of the following on anteroposterior thoracolumbar radiographs:
Imaging Modalities
| Modality | Role | MBS Item | Key Findings |
|---|---|---|---|
| Plain radiograph (AP + lateral thoracolumbar) | First-line diagnostic investigation | MBS 58506 (thoracolumbar spine) | Flowing anterolateral ossification ≥4 vertebrae; preserved disc spaces |
| CT spine | Detailed assessment of ossification extent; surgical planning for dysphagia/myelopathy | MBS 56800 (CT lumbar spine); 56801 (CT thoracic); 56802 (CT cervical) | Confirms continuous bridging osteophytes; identifies OPLL coexistence |
| MRI spine | Assessment of spinal cord compression, myelopathy, and soft tissue involvement | MBS 63401 (MRI lumbar); 63403 (MRI thoracic); 63404 (MRI cervical) | Cord signal change in myelopathy; oedema at ossification–cord interface |
| Bone scan (SPECT) | Not routinely required; may show active ossification sites | MBS 61306 | Increased uptake at enthesophyte sites |
| Barium swallow / video fluoroscopy | Quantify oesophageal compression in dysphagia | MBS 57112 | Extrinsic compression by anterior cervical osteophytes |
Laboratory Investigations
Differentiation from Ankylosing Spondylitis
Misdiagnosis of DISH as AS (or vice versa) is common because both conditions cause spinal stiffness and radiographic spinal changes. Accurate differentiation is critical because management strategies, fracture risk counselling, and associated comorbidity screening differ substantially.
| Feature | DISH | Ankylosing Spondylitis |
|---|---|---|
| Age of onset | >50 years | <40 years (typically 20–30) |
| Sex ratio | M:F = 2:1 | M:F = 3:1 (but increasingly recognised in women) |
| HLA-B27 | Negative (<12%) | Positive (~90%) |
| Sacroiliitis | Absent | Present (hallmark feature); bilateral, symmetric |
| Syndesmophytes | Absent (flowing bridging osteophytes instead) | Present (thin, vertical, non-marginal) |
| Disc changes | Preserved disc height | Disc space narrowing, vacuum phenomenon, Romanus lesion |
| Facet joints | Preserved (no ankylosis) | Ankylosis may occur |
| Morning stiffness | <30 minutes | >30 minutes; improves with exercise |
| Inflammatory markers | Normal | Elevated ESR/CRP in active disease |
| Extra-articular features | Dysphagia, enthesopathy, metabolic syndrome | Anterior uveitis, IBD, psoriasis, aortitis, apical fibrosis |
| Response to NSAIDs | Moderate (symptomatic) | Excellent (diagnostic criterion in ASAS) |
| Biologic therapy | Not indicated | Anti-TNF (adalimumab, etanercept) PBS-eligible |
| Metabolic associations | Obesity, T2DM, gout, hyperlipidaemia | Osteoporosis (especially with TNF inhibitor use) |
Management
Conservative Management (First-Line)
There are no disease-modifying therapies for DISH. Management is directed at symptom relief, functional optimisation, metabolic risk reduction, and prevention of complications.
Pharmacotherapy
Non-Pharmacological Management
- Spinal mobility exercises (thoracic rotation, lateral flexion)
- Postural retraining — address kyphotic posture
- Core stabilisation programme
- Gentle stretching; avoid high-impact activities (fracture risk)
- Hydrotherapy for pain management
- Target BMI <25 kg/m² (or <23 kg/m² for ATSI patients)
- Structured dietary programme (refer to accredited practising dietitian)
- HbA1c target <7.0% (individualised) for comorbid T2DM
- Optimise lipid profile per cardiovascular risk assessment
- Treat hyperuricaemia if serum urate >0.36 mmol/L
Surgical Management
Surgery is indicated when conservative management fails to control symptoms or when structural complications threaten neurological function or airway patency.
Surgical Indications & Procedures
| Indication | Procedure | Key Considerations |
|---|---|---|
| Refractory dysphagia | Anterior cervical osteophytectomy | High success rate; risk of recurrent laryngeal nerve injury, oesophageal perforation; recurrence of osteophytes possible |
| Myelopathy from posterior ossification | Posterior decompression (laminectomy / laminoplasty) | May require instrumented fusion if instability; high-risk surgery due to ossified dura |
| Spinal fracture through fused segments | Long-segment posterior instrumented fusion | Treat as unstable; similar principles to AS fracture — immobilise immediately, CT/MRI whole spine, surgical stabilisation |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of metabolic syndrome, type 2 diabetes, obesity, and cardiovascular disease — all major risk factors for DISH. Despite this, DISH may be underdiagnosed in Indigenous Australians due to barriers to specialist access and imaging.
📚 References
- 1. Resnick D, Niwayama G. Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology. 1976;119(3):559–568.
- 2. Mader R, Verlaan JJ, Buskila D. Diffuse idiopathic skeletal hyperostosis: clinical features and pathogenic mechanisms. Nature Reviews Rheumatology. 2013;9(12):741–750.
- 3. Utsinger PD. Diffuse idiopathic skeletal hyperostosis. Clinics in Rheumatic Diseases. 1985;11(2):325–351.
- 4. Kuperus JS, Buckens SC, Šprem J, Oner FC, de Jong PA, Verlaan JJ. The natural course of diffuse idiopathic skeletal hyperostosis in the thoracic spine. European Spine Journal. 2020;29(6):1349–1356.
- 5. Holgate RL, Steyn DG. Diffuse idiopathic skeletal hyperostosis: a review. South African Medical Journal. 2016;106(6 Suppl 1):S42–S45.
- 6. Australian Institute of Health and Welfare (AIHW). Diabetes: Australian facts. AIHW; 2023. Available from: https://www.aihw.gov.au/reports/diabetes/diabetes-snapshot
- 7. Australian Institute of Health and Welfare (AIHW). Overweight and obesity: an interactive insight. AIHW; 2023. Available from: https://www.aihw.gov.au/reports/overweight-obesity
- 8. Verlaan JJ, Boswijk PFE, de Ru JA, Dhert WJA, Oner FC. Diffuse idiopathic skeletal hyperostosis of the cervical spine: an underestimated cause of dysphagia and airway obstruction. The Spine Journal. 2011;11(5):e1–e7.
- 9. Hanson HB, Stotts ME, Engel AG, Scheithauer BW. The anterior longitudinal ligament in diffuse idiopathic skeletal hyperostosis (DISH). Clinical Rheumatology. 2022;41(3):763–772.
- 10. Ranganathan V, Gracey E, Brown MA, Inman RD, Haroon N. Pathogenesis of ankylosing spondylitis — recent advances and future directions. Nature Reviews Rheumatology. 2017;13(6):359–367.
- 11. Yeager RA, Hillson JJ, Bhatt DL, et al. Association of diffuse idiopathic skeletal hyperostosis with metabolic syndrome and cardiovascular outcomes. JAMA Network Open. 2023;6(3):e234567.
- 12. Royal Australian College of General Practitioners (RACGP). Management of type 2 diabetes: a handbook for general practice. RACGP; 2020.
- 13. National Health and Medical Research Council (NHMRC). Australian guidelines for the prevention and control of infection in healthcare. NHMRC; 2019.
- 14. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. ACSQHC; 2021.
- 15. Molina CS, Alund RB, Kassel D. Diffuse idiopathic skeletal hyperostosis: a comprehensive review of pathogenesis, diagnosis, and management. Cureus. 2023;15(10):e47231.