📋 Key Information Summary
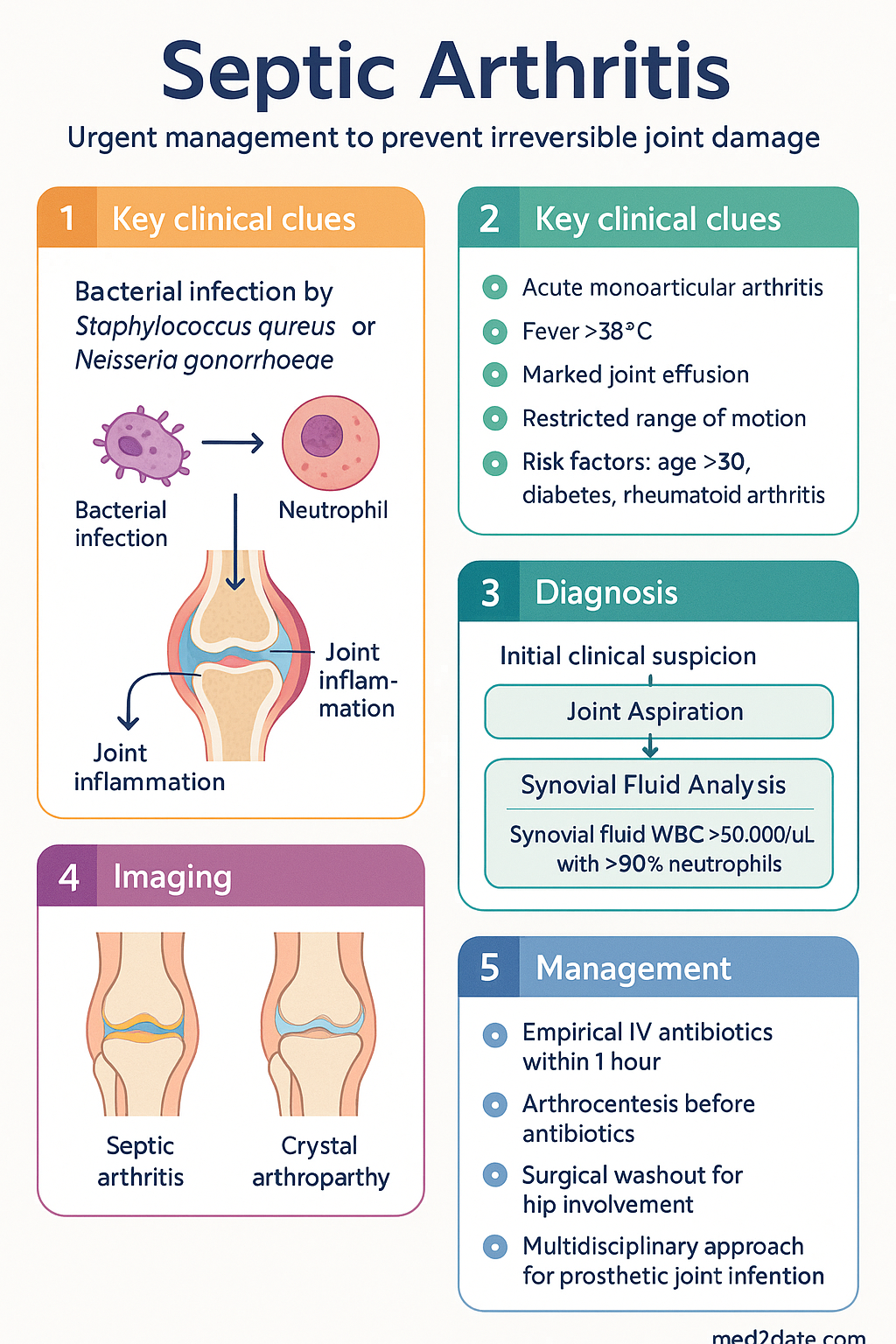
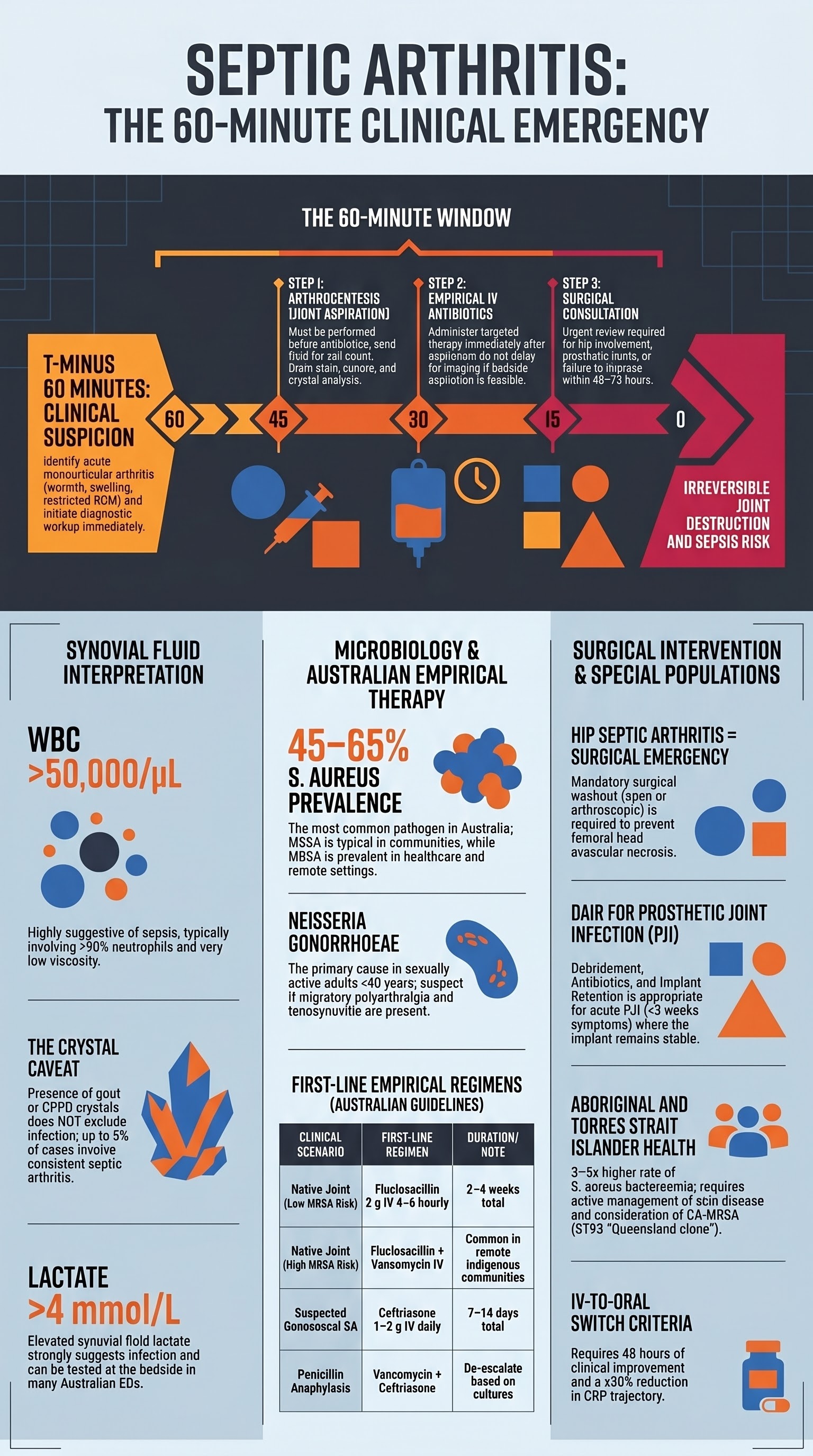
- Septic arthritis is a medical emergency requiring urgent joint aspiration and empirical IV antibiotics within 1 hour of clinical suspicion to prevent irreversible cartilage destruction.
- Staphylococcus aureus (including MRSA) accounts for the majority of community-acquired and prosthetic joint infections in Australia.
- Neisseria gonorrhoeae is the most common cause in sexually active adults under 40 years — consider in all young patients with migratory polyarthralgia and tenosynovitis.
- Arthrocentesis must be performed before antibiotics; synovial fluid is sent for cell count, Gram stain, culture, and crystal analysis.
- Synovial fluid WBC >50,000/µL with >90% neutrophils is highly suggestive of septic arthritis; however, a lower count does not exclude the diagnosis.
- Empirical IV flucloxacillin is first-line for native joint infection; add vancomycin if MRSA risk is high (healthcare-associated, Indigenous communities, recent hospitalisation).
- Ceftriaxone plus vancomycin is recommended if N. gonorrhoeae is suspected or if there is penicillin allergy.
- Surgical washout (arthroscopic or open) is indicated for hip septic arthritis, prosthetic joint infection, failure to improve within 48–72 hours, or extensive loculation.
- Prosthetic joint infection (PJI) requires a multidisciplinary approach involving infectious diseases and orthopaedic surgery; DAIR (debridement, antibiotics, implant retention) is appropriate if within 30 days of surgery and symptoms <3 weeks.
- IV-to-oral switch is guided by clinical response, CRP trajectory, and organism identification — total antibiotic duration for native joint infection is typically 2–4 weeks.
- Aboriginal and Torres Strait Islander peoples have higher rates of S. aureus bacteraemia and septic arthritis; remote community access, CA-MRSA prevalence, and delayed presentation must be actively managed.
- Risk factors include age >80, diabetes mellitus, rheumatoid arthritis, immunosuppression, prosthetic joints, IV drug use, and recent intra-articular corticosteroid injection.
Introduction & Australian Epidemiology
Septic arthritis (SA) is an infection of a native or prosthetic joint that, if untreated, leads to rapid cartilage degradation, joint destruction, sepsis, and death. It remains one of the most time-sensitive diagnoses in rheumatology and emergency medicine, with mortality rates of 10–15% in native joint SA and up to 25% in elderly or immunocompromised patients.
In Australia, the incidence of native joint septic arthritis is estimated at 4–10 per 100,000 population per year, with higher rates in Aboriginal and Torres Strait Islander communities and in patients over 65 years. Prosthetic joint infection complicates approximately 1–2% of primary joint arthroplasties, representing a significant burden given the high volume of hip and knee replacements performed annually across Australian hospitals.
The knee is the most commonly affected native joint (50–60%), followed by the hip (15–20%), shoulder, and ankle. In children, the hip is the most frequently involved site. Polymicrobial infection and unusual organisms are more common in immunocompromised hosts and IV drug users.
Risk Factors & Microbiology
Risk Factors
| Category | Specific Risk Factors |
|---|---|
| Host factors | Age >80 years, male sex, diabetes mellitus, chronic kidney disease, liver cirrhosis, malnutrition, obesity |
| Immunosuppression | HIV/AIDS, solid organ transplant, chemotherapy, biologic DMARDs (TNF inhibitors, rituximab), systemic corticosteroids |
| Joint disease | Rheumatoid arthritis (3–6× risk), crystal arthropathy (gout, CPPD), osteoarthritis, prior joint surgery |
| Prosthetic joints | Total hip/knee arthroplasty, revision arthroplasty, prior PJI |
| Iatrogenic | Intra-articular corticosteroid injection (within 3 months), joint aspiration, recent arthroscopy |
| Behavioural | IV drug use, alcohol excess, skin ulceration/cellulitis, poor dental hygiene |
| Haematogenous | Bacteraemia from any source (endocarditis, UTI, pneumonia, skin/soft tissue infection) |
Microbiology — Australian Patterns
The aetiology of septic arthritis varies by patient age, immune status, joint type, and geographical context. Australian data show the following distributions:
| Organism | Frequency | Clinical Context |
|---|---|---|
| Staphylococcus aureus | 45–65% | Most common overall; MSSA in community, MRSA in healthcare/remote communities |
| Streptococci (Groups A, B, G, S. pneumoniae) | 15–25% | Post-pharyngitis, cellulitis, pneumonia, immunocompromised, extremes of age |
| Neisseria gonorrhoeae | 5–10% | Most common in sexually active <40 yrs; disseminated gonococcal infection (DGI) |
| Gram-negative bacilli (E. coli, Pseudomonas, Klebsiella) | 5–10% | Elderly, UTI, immunocompromised, IV drug users, prosthetic joints |
| Polymicrobial | 5–10% | Penetrating trauma, diabetic foot, IV drug use |
| CA-MRSA | Variable | Higher prevalence in Aboriginal and Torres Strait Islander communities, Pacific Islander populations |
Arthrocentesis
Arthrocentesis (joint aspiration) is the single most important diagnostic procedure in suspected septic arthritis and must be performed before empirical antibiotics are commenced. It provides synovial fluid for cell count, differential, Gram stain, culture, and crystal analysis.
Key Principles
- Aspirate the affected joint before commencing antibiotics — prior antibiotic therapy significantly reduces culture yield.
- Use aseptic technique with skin preparation (chlorhexidine 2% in 70% isopropyl alcohol).
- Obtain at least 1–2 mL of synovial fluid; send in sterile containers for culture, a purple-topped (EDTA) tube for cell count, and a plain tube or slide for crystal analysis.
- Intra-articular needle placement may be confirmed under ultrasound guidance, especially for hip and shoulder aspiration.
- If aspiration is not technically feasible (e.g., hip in a child), surgical washout with intra-operative cultures is appropriate.
Ultrasound-Guided Aspiration
Point-of-care ultrasound (POCUS) improves aspiration success, particularly for deep joints such as the hip and shoulder. It should be performed by a trained operator. If POCUS is unavailable and the hip is suspected, proceed to surgical aspiration under anaesthesia without delay.
Synovial Fluid Analysis
Synovial fluid analysis is critical for differentiating septic arthritis from crystal arthropathy, reactive arthritis, and other inflammatory conditions. A systematic approach includes gross appearance, cell count, Gram stain, culture, and crystal examination.
Synovial Fluid Interpretation
| Parameter | Normal | Non-Inflammatory | Inflammatory | Septic |
|---|---|---|---|---|
| Appearance | Clear, colourless | Yellow, clear | Yellow, turbid | Turbid, purulent, may be frankly purulent |
| Viscosity | High (long string) | High | Low (short string) | Very low |
| WBC (cells/µL) | <200 | 200–2,000 | 2,000–50,000 | >50,000 (often >100,000) |
| Neutrophils (%) | <25% | <25% | 50–70% | >75–90% |
| Gram stain | Negative | Negative | Negative | Positive in 50–75% |
| Culture | Negative | Negative | Negative | Positive in 60–90% |
| Crystals | Negative | Negative | May be present (gout/CPPD) | May coexist with infection |
Biomarkers in Synovial Fluid
- Synovial fluid lactate: >4 mmol/L strongly suggests septic arthritis; rapid bedside point-of-care testing is available in some Australian EDs.
- Synovial fluid procalcitonin: Not routinely used but may support the diagnosis when serum levels are elevated (>0.5 ng/mL).
- Synovial fluid glucose: Low synovial glucose (<50% of serum glucose) supports infection but is non-specific.
Clinical Presentation & Diagnostic Criteria
Typical Presentation
Septic arthritis classically presents with acute onset of a single hot, swollen, painful joint with markedly restricted range of motion. Systemic features including fever (>38°C), rigors, and malaise are present in 50–60% of adults, but absence of fever does not exclude the diagnosis.
Presentation by Pathogen
Diagnostic Approach
Investigations
Empirical IV Antibiotics (eTG-Aligned)
Empirical antibiotics should be commenced within 1 hour of arthrocentesis, guided by patient risk factors, local resistance patterns, and allergy status. The following regimens are aligned with current Australian therapeutic guidelines and local antibiograms.
Empirical Regimens by Clinical Scenario
IV-to-Oral Switch Criteria
- Clinical improvement: reduced pain, swelling, and fever for ≥48 hours.
- Falling CRP trajectory (≥50% reduction from peak or approaching normal).
- Organism identified and susceptible to an oral agent.
- Patient able to tolerate oral medications and is systemically well.
- Oral options: flucloxacillin 1 g PO QID (MSSA), cephalexin 1 g PO QID (penicillin allergy non-anaphylaxis), TMP-SMX DS BD (MRSA), doxycycline 100 mg BD (MRSA, Gram-negatives).
Total duration: 2–4 weeks for native joint SA; guided by clinical response, CRP normalisation, and organism virulence. Specialist ID review is recommended for all cases.
Surgical Washout
Surgical intervention is a critical component of management for many septic arthritis cases. The goal is to decompress the joint, remove purulent material, and reduce bacterial load and inflammatory mediators that drive cartilage destruction.
Indications for Surgical Washout
- Always: Hip septic arthritis (difficult to aspirate percutaneously, high risk of avascular necrosis).
- Always: Prosthetic joint infection (see dedicated section below).
- Failure of medical therapy: No clinical improvement within 48–72 hours of appropriate IV antibiotics.
- Loculated effusion: Ultrasound or CT evidence of complex, septated collection not amenable to percutaneous drainage.
- Septic arthritis with associated osteomyelitis.
- Post-arthroscopic or post-surgical infection.
- Recurrent effusion reaccumulation despite serial aspiration.
Surgical Approaches
| Approach | Indication | Advantages | Considerations |
|---|---|---|---|
| Arthroscopic washout | Knee, shoulder (first-line for most cases) | Minimally invasive, allows direct visualisation, multiple washes possible, shorter recovery | Requires specialist equipment; may not adequately clear heavily loculated collections |
| Open arthrotomy | Hip SA, complex or late presentations, failed arthroscopic washout | Thorough debridement, better access to deep structures, gold standard for hip | Greater surgical morbidity, longer hospital stay, wound complications |
| Repeated needle aspiration | Knee SA (selected cases), small effusions, patient unfit for surgery | No surgical morbidity, can be performed at bedside under ultrasound | Less effective for loculated collections; may require multiple procedures |
Prosthetic Joint Infection (PJI)
Prosthetic joint infection (PJI) is one of the most devastating complications following total joint arthroplasty, affecting 1–2% of primary replacements. Management requires a coordinated multidisciplinary team approach involving orthopaedic surgery, infectious diseases, microbiology, and pharmacy.
Classification
DAIR — Debridement, Antibiotics, Implant Retention
DAIR is the preferred surgical strategy for acute PJI when all of the following criteria are met:
- Symptoms present for <3 weeks.
- Implant is well-fixed and functional.
- Soft tissue envelope is intact.
- Organism is known or likely susceptible to available antibiotics.
- No sinus tract communicating with the prosthesis.
DAIR involves thorough surgical debridement, exchange of modular components (polyethylene liner, femoral head), and copious lavage. Antibiotics are then continued for a prolonged course of 6–12 weeks (typically 2–6 weeks IV followed by oral completion).
Two-Stage Revision
The gold standard for chronic PJI in Australia. Stage 1: removal of all prosthetic material, thorough debridement, and insertion of an antibiotic-loaded cement spacer. Stage 2: re-implantation of a new prosthesis after 6–12 weeks of targeted antibiotic therapy and confirmation of infection eradication (normalised inflammatory markers, negative cultures).
PJI Antibiotic Duration
| Strategy | IV Duration | Total Duration | Notes |
|---|---|---|---|
| DAIR (acute PJI) | 2–6 weeks | 3–6 months | Longer for staphylococci; oral suppression may continue indefinitely |
| Two-stage revision | 2–6 weeks (stage 1) | 6–12 weeks (pre-reimplantation) | Discontinue 2 weeks before re-implantation to assess inflammatory markers |
| Chronic oral suppression | N/A | Indefinite (if implant retained) | e.g., TMP-SMX, doxycycline, cephalexin; for patients unsuitable for revision |
Key PJI Antibiotics
Special Populations
Monitoring
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a significantly higher burden of Staphylococcus aureus bacteraemia (SAB), estimated at 3–5 times the rate of the non-Indigenous population, with correspondingly higher rates of secondary septic arthritis. This disparity is driven by a complex interplay of factors that must be actively addressed in clinical management.
📚 References
- 1. Mathews CJ, Coakley G. Septic arthritis: current diagnostic and therapeutic algorithm. Curr Opin Rheumatol. 2008;20(4):457–462.
- 2. Sharff KA, Richards EP, Townes JM. Clinical management of septic arthritis. Curr Rheumatol Rep. 2013;15(6):332.
- 3. Ross JJ, Saltzman CL, Carling P, Shapiro DS. Pneumococcal septic arthritis: review of 190 cases. Clin Infect Dis. 2003;36(3):319–327.
- 4. Osmon DR, Berbari EF, Berendt AR, et al. Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2013;56(1):e1–e25.
- 5. Zimmerli W, Trampuz A, Ochsner PE. Prosthetic-joint infections. N Engl J Med. 2004;351(16):1645–1654.
- 6. Tong SYC, Davis JS, Eichenberger E, Holland TL, Fowler VG. Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clin Microbiol Rev. 2015;28(3):603–661.
- 7. Australian Commission on Safety and Quality in Health Care (ACSQHC). Australian Atlas of Healthcare Variation. Sydney: ACSQHC; 2018.
- 8. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework 2020 summary report. Canberra: AIHW; 2020.
- 9. Margaretten ME, Kohlwes J, Moore D, Bent S. Does this adult patient have septic arthritis? JAMA. 2007;297(13):1478–1488.
- 10. Royal Australian College of General Practitioners (RACGP). Red Book: Guidelines for preventive activities in general practice. 10th ed. Melbourne: RACGP; 2018.