📋 Key Information Summary
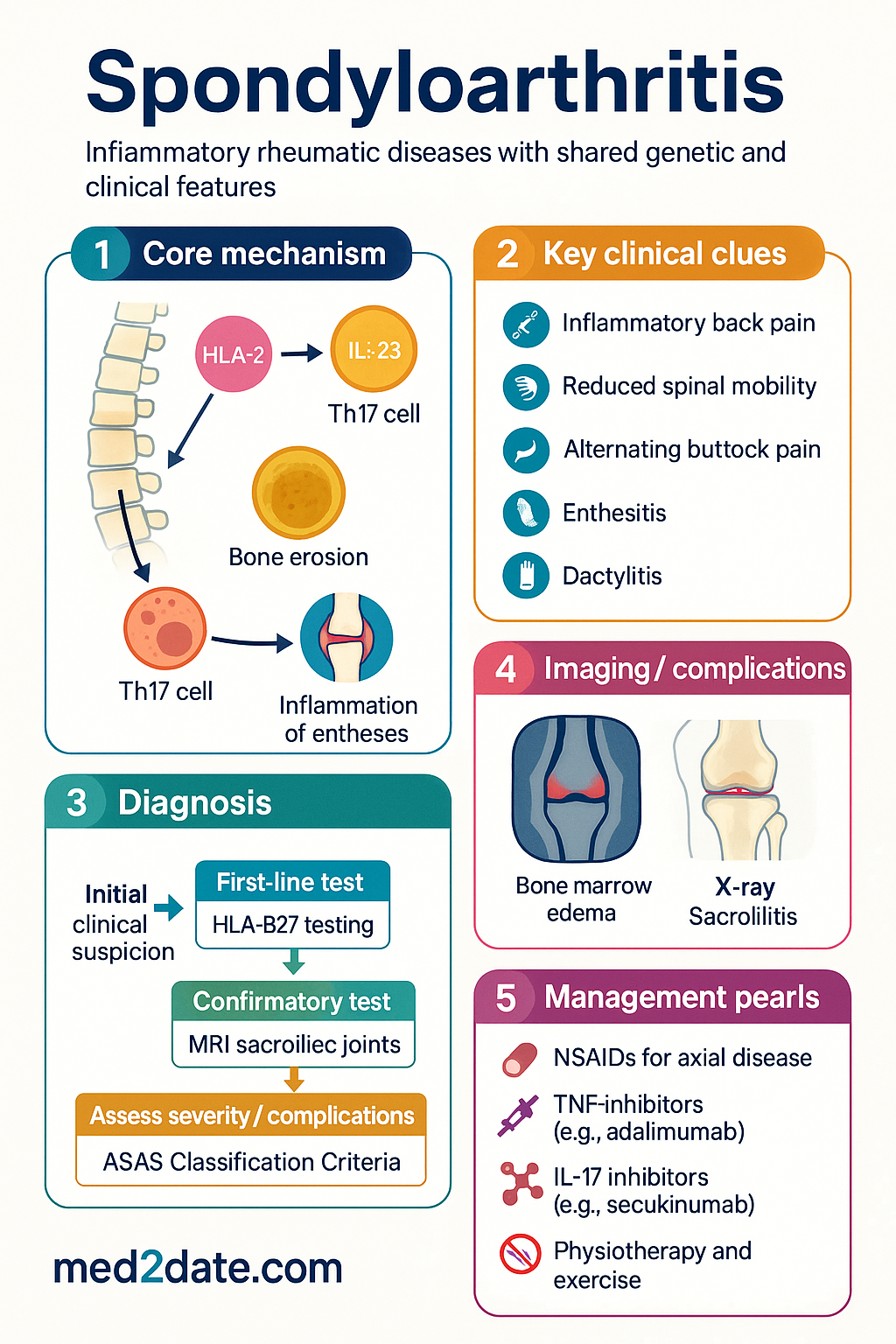
- Spondyloarthritis (SpA) encompasses a group of inflammatory rheumatic diseases with shared genetic (HLA-B27) and clinical features.
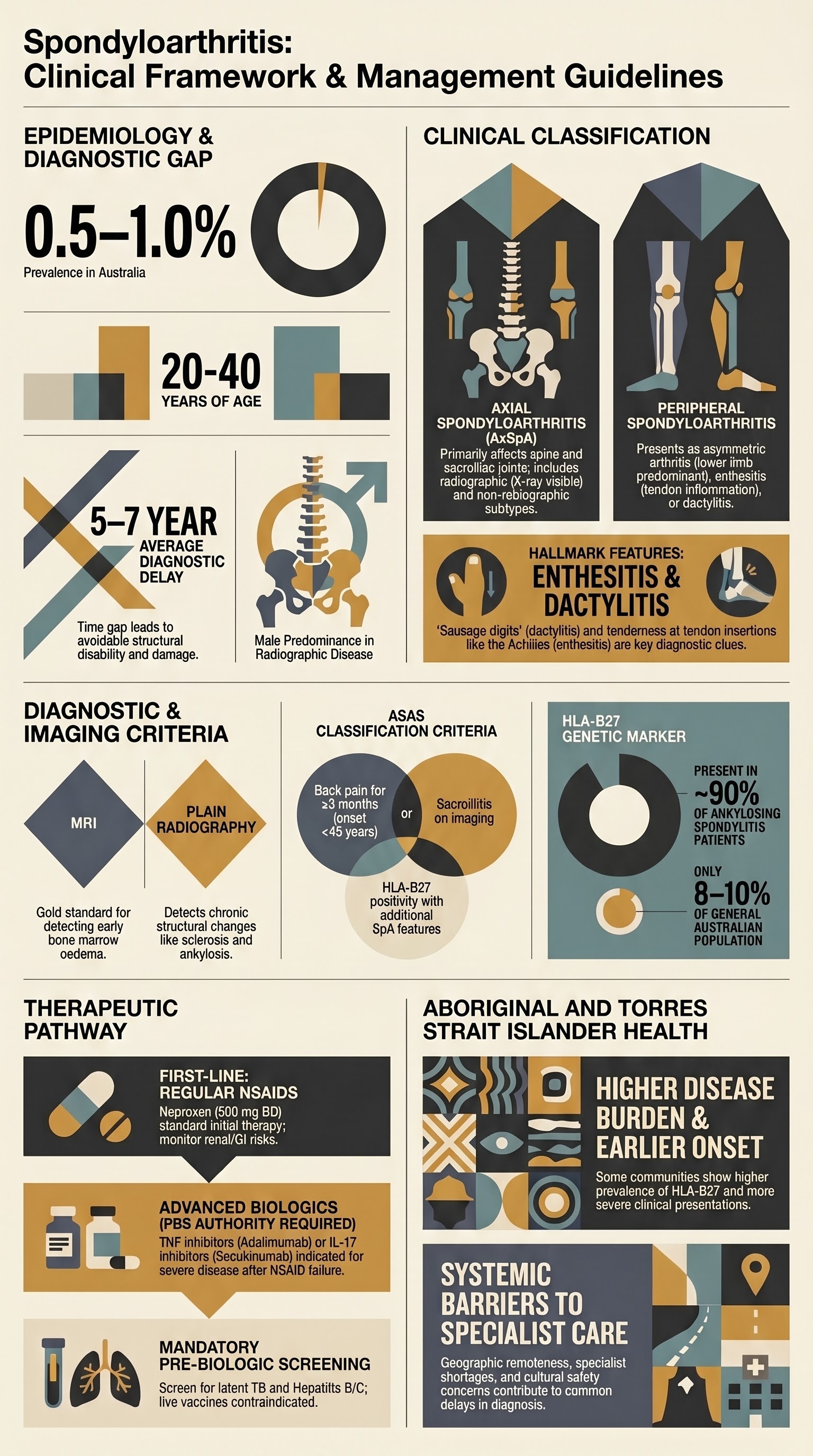
- Classification is split into axial SpA (including ankylosing spondylitis) and peripheral SpA.
- Diagnosis is clinical, supported by imaging (X-ray/MRI sacroiliac joints) and HLA-B27 testing per ASAS classification criteria.
- First-line pharmacotherapy for axial disease is regular NSAIDs (e.g., naproxen 500 mg BD); monitor renal/GI risk.
- TNF inhibitors (e.g., adalimumab) or IL-17 inhibitors (e.g., secukinumab) are PBS Authority Required for severe active axial SpA after NSAID failure.
- Peripheral arthritis may respond to DMARDs (sulfasalazine, methotrexate); evidence is limited.
- HLA-B27 testing is most useful in patients with intermediate pre-test probability of axial SpA; not a standalone diagnostic.
- MRI is more sensitive than X-ray for early sacroiliitis (bone marrow oedema).
- Enthesitis and dactylitis are hallmark clinical features; assess with clinical exam (e.g., Leeds Enthesitis Index).
- Non-pharmacological management is essential: physiotherapy, exercise, smoking cessation.
- Aboriginal and Torres Strait Islander peoples have higher HLA-B27 prevalence and SpA burden; ensure culturally safe care and access to specialist services.
Introduction & Australian Epidemiology
Spondyloarthritis (SpA) is a group of interrelated chronic inflammatory rheumatic diseases. In Australia, prevalence of axial SpA is estimated at 0.5–1.0%. Disease typically presents in young adults (20–40 years), with a male predominance for radiographic axial SpA (ankylosing spondylitis).
Axial Spondyloarthritis
Axial SpA primarily affects the spine and sacroiliac joints. It is subdivided into:
- Radiographic axial SpA (ankylosing spondylitis): Definite sacroiliitis on X-ray (≥Grade 2 bilateral or ≥Grade 3 unilateral).
- Non-radiographic axial SpA: Inflammatory back pain + sacroiliitis on MRI or HLA-B27 positivity, but without definitive X-ray changes.
Clinical Features
- Inflammatory back pain: age of onset <45 years, insidious onset, improves with exercise, not relieved by rest, night pain (second half of night).
- Reduced spinal mobility (Schober's test, lateral flexion).
- Alternating buttock pain.
Peripheral Spondyloarthritis
Peripheral SpA presents with one or more of:
- Peripheral arthritis: Typically oligoarticular, asymmetric, lower limb predominant.
- Enthesitis: Inflammation at tendon/ligament insertion (e.g., Achilles, plantar fascia).
- Dactylitis: "Sausage digit" (diffuse swelling of a finger or toe).
This may occur in isolation or with concurrent axial disease. Subtypes include psoriatic arthritis, reactive arthritis, and arthritis associated with inflammatory bowel disease.
HLA-B27 Testing
HLA-B27 is a genetic marker strongly associated with SpA, but not diagnostic.
| Aspect | Details |
|---|---|
| Prevalence in Australia | 8–10% general population; ~90% of ankylosing spondylitis patients. |
| MBS Item | MBS item 71151 (HLA typing, one locus). |
| When to test | Suspected axial SpA with intermediate pre-test probability (e.g., chronic back pain + ≥1 SpA feature). |
| Interpretation | Positive result increases likelihood; negative result makes axial SpA less likely (especially if pre-test probability low). |
Sacroiliitis (Imaging & ASAS Criteria)
ASAS Classification Criteria for Axial SpA
In patients with back pain ≥3 months and age of onset <45 years:
- Sacroiliitis on imaging* PLUS ≥1 SpA feature, OR
- HLA-B27 positivity PLUS ≥2 other SpA features.
*Imaging: X-ray (radiographic sacroiliitis) or MRI (active inflammation: bone marrow oedema).
Imaging Modalities
TNF & IL-17 Inhibitors
Indicated for severe active axial SpA (radiographic or non-radiographic) with inadequate response to ≥2 NSAIDs over 4 weeks total.
Key Considerations
- Screening: Mandatory for latent TB (IGRA/TST) and hepatitis B/C before initiation.
- Live vaccines contraindicated during therapy.
- Choice: TNF-i are first-line biologics. IL-17i are an alternative first-line or second-line if TNF-i fail/contraindicated.
Enthesitis & Dactylitis
These are hallmark clinical features of SpA.
Assessment
- Enthesitis: Tenderness at specific sites (e.g., lateral epicondyle, Achilles insertion, plantar fascia). Validated index: Leeds Enthesitis Index (LEI).
- Dactylitis: Diffuse swelling of entire digit ("sausage digit").
Management
- Local corticosteroid injection for severe focal enthesitis/dactylitis.
- Systemic therapy (NSAIDs, biologics) for widespread or refractory disease.
- IL-17 inhibitors (e.g., secukinumab) show particular efficacy for enthesitis.
Aboriginal and Torres Strait Islander Health
📚 References
- 1. Sieper J, Rudwaleit M, Baraliakos X, et al. The Assessment of SpondyloArthritis international Society (ASAS) handbook: a guide to assess spondyloarthritis. Ann Rheum Dis. 2009;68(Suppl 2):ii1-ii44.
- 2. van der Heijde D, Ramiro S, Landewé R, et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Ann Rheum Dis. 2017;76(6):978-991.
- 3. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2017.
- 4. Australian Institute of Health and Welfare (AIHW). Arthritis and other musculoskeletal conditions across the life stages. Cat. no. PHE 186. Canberra: AIHW; 2014.
- 5. Robinson PC, Brown MA. Genetics of ankylosing spondylitis. Mol Immunol. 2014;57(1):2-11.
- 6. Navarro-Compán V, Sepriano A, El-Zorkany B, van der Heijde D. Axial spondyloarthritis on MRI. Best Pract Res Clin Rheumatol. 2017;31(6):795-809.
- 7. Ward MM, Deodhar A, Gensler LS, et al. 2019 Update of the American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network Recommendations for the Treatment of Ankylosing Spondylitis and Nonradiographic Axial Spondyloarthritis. Arthritis Rheumatol. 2019;71(10):1599-1613.
- 8. Maksymowych WP, Mallon C, Spady B, et al. The Canadian Research Group of Axial Spondyloarthritis (CARGO) recommendations for the use of tumour necrosis factor inhibitors in axial spondyloarthritis. J Rheumatol. 2010;37(11):2435-2440.
- 9. Australian Government Department of Health. Pharmaceutical Benefits Scheme (PBS). Available at: www.pbs.gov.au. [Accessed 2024].
- 10. Telethon Kids Institute. Aboriginal Arthritis and Musculoskeletal Health Research. Perth; 2022.
- 11. Ramiro S, Nikiphorou E, Sepriano A, et al. ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update. Ann Rheum Dis. 2023;82(1):19-34.