📋 Key Information Summary
- Gout affects approximately 6.8% of Australian men and 2.0% of women, with significantly higher prevalence in Aboriginal and Torres Strait Islander peoples and those of Māori or Pacific Islander descent.
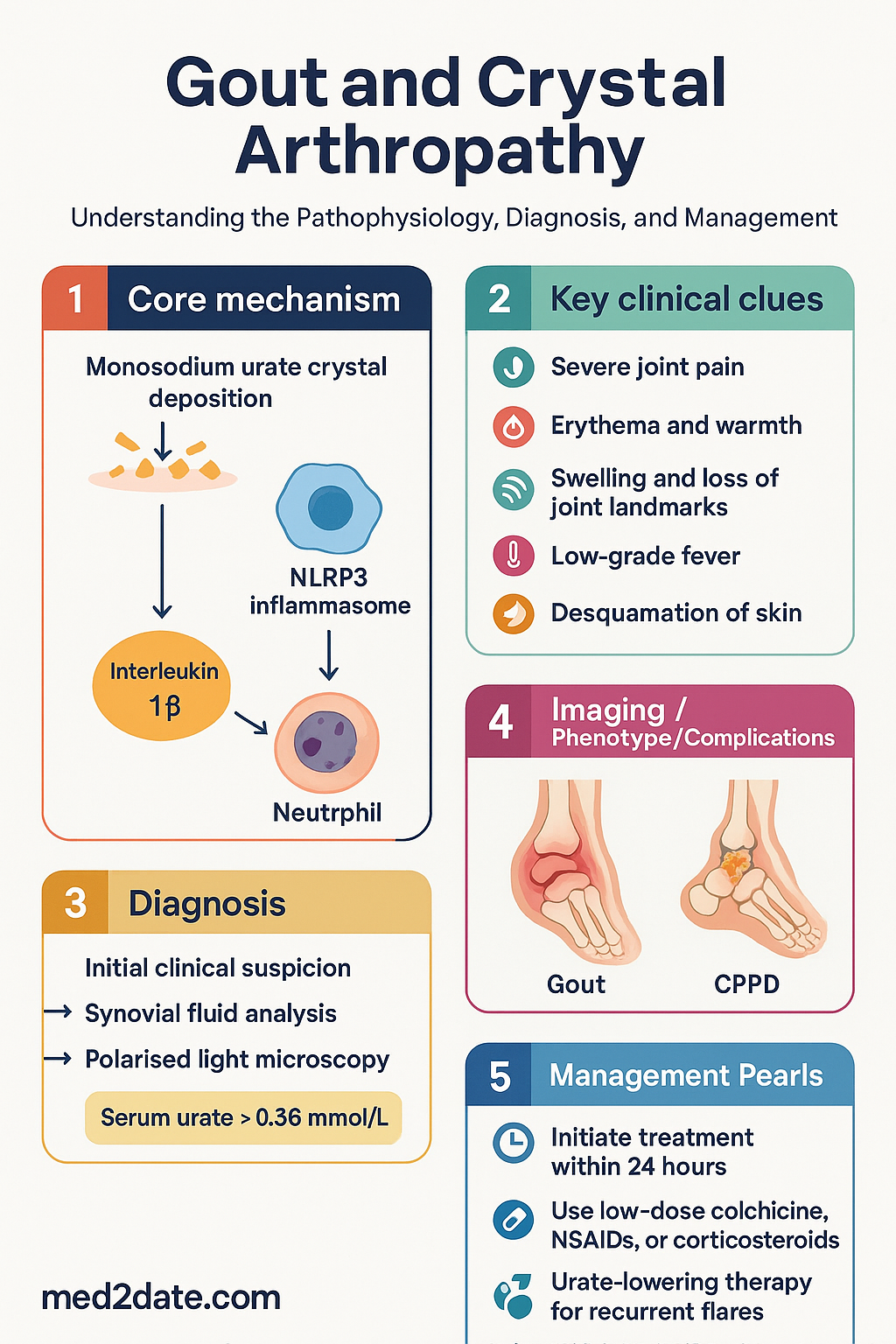
- Acute gout flare should be treated within 24 hours of symptom onset; colchicine (low-dose regimen), NSAIDs, or oral/intra-articular corticosteroids are all first-line options.
- Low-dose colchicine regimen: 0.5 mg twice daily for up to 3–5 days after flare onset — avoid old high-dose loading regimens due to toxicity risk.
- Urate-lowering therapy (ULT) should be considered after ≥2 flares per year, tophi, radiographic damage, or urate nephrolithiasis; target serum urate <0.36 mmol/L (or <0.30 mmol/L if tophi present).
- Allopurinol is first-line ULT; start at 50–100 mg daily, titrate by 50–100 mg every 2–4 weeks to serum urate target; requires renal dose adjustment.
- HLA-B*5801 testing is MANDATORY before initiating allopurinol in patients of South-East Asian, African American, or Han Chinese descent due to severe cutaneous adverse reaction (SCAR) risk.
- Febuxostat is second-line ULT for allopurinol-intolerant patients; PBS Authority Required; consider cardiovascular risk (CARES trial findings).
- Prophylaxis with low-dose colchicine (0.5 mg once daily) or low-dose NSAID is essential when commencing ULT to prevent flares triggered by urate mobilisation.
- CPPD (calcium pyrophosphate deposition) presents as acute pseudogout or chronic pyrophosphate arthropathy; diagnosis requires synovial fluid analysis showing weakly positively birefringent rhomboid crystals.
- Dietary modification (reduce purine-rich foods, alcohol, fructose-sweetened beverages; increase dairy intake) and weight management are important adjuncts to pharmacotherapy.
- ATSI communities experience gout at higher rates with earlier onset, more tophaceous disease, and significant barriers to specialist access in remote areas.
- Asymptomatic hyperuricaemia does not require treatment; ULT is indicated only for symptomatic gout or specific clinical scenarios (urate nephrolithiasis, tumour lysis prophylaxis).
Introduction & Australian Epidemiology
Gout is the most common form of inflammatory arthritis in Australia, resulting from the deposition of monosodium urate (MSU) crystals in joints, soft tissues, and kidneys. It represents a significant and growing burden on the Australian healthcare system, with prevalence increasing in parallel with rising rates of metabolic syndrome, obesity, and chronic kidney disease.
The Australian Institute of Health and Welfare (AIHW) estimates that gout affects approximately 6.8% of Australian men and 2.0% of women, with a marked increase in prevalence with age — exceeding 15% in men over 70 years. Aboriginal and Torres Strait Islander peoples experience gout at 1.5–2 times the rate of non-Indigenous Australians, with earlier onset and more severe disease including tophaceous gout.
Crystal arthropathy encompasses two major conditions: gout (monosodium urate crystal deposition) and calcium pyrophosphate deposition (CPPD) disease, historically termed pseudogout. Both conditions share overlapping risk factors including age, metabolic disease, and chronic kidney disease, and may coexist in the same patient.
The economic burden is substantial: gout accounts for over 500,000 general practice consultations annually in Australia, with significant direct costs from pharmaceuticals, emergency department presentations, and indirect costs from work disability.
Pathophysiology
Gout — Monosodium Urate Crystal Deposition
Uric acid is the end product of purine metabolism, generated by xanthine oxidase. Humans lack uricase, resulting in higher serum urate concentrations compared with other mammals. When serum urate exceeds the saturation point (~0.36 mmol/L at physiological pH and temperature), MSU crystals may nucleate and deposit in synovial fluid, cartilage, tendons, and periarticular soft tissues.
The acute gout flare is triggered by innate immune recognition of deposited MSU crystals. Monocytes and synoviocytes phagocytose crystals, activating the NLRP3 inflammasome and triggering release of interleukin-1β (IL-1β). This drives neutrophil recruitment, intense local inflammation, and the characteristic severe pain, swelling, and erythema.
CPPD — Calcium Pyrophosphate Deposition
CPPD results from deposition of calcium pyrophosphate dihydrate (CPP) crystals in articular cartilage (chondrocalcinosis) and periarticular structures. The pathogenesis involves excess pyrophosphate generation by chondrocytes (via ectonucleotide pyrophosphatase/phosphodiesterase activity) combined with elevated local calcium concentrations. CPPD is strongly associated with ageing, osteoarthritis, metabolic diseases (hyperparathyroidism, haemochromatosis, hypomagnesaemia, hypophosphatasia), and prior joint trauma.
Acute Gout Flare
Clinical Presentation
The acute gout flare typically presents as a monoarticular or oligoarticular inflammatory arthritis with rapid onset (reaching maximum intensity within 6–24 hours). The first metatarsophalngeal joint (podagra) is affected in approximately 50% of first episodes and 90% of patients at some point. Other commonly involved joints include the midfoot, ankle, knee, wrist, and small joints of the hand.
Characteristic features include:
- Severe pain — often described as the "worst pain ever experienced"
- Erythema and warmth of the overlying skin (may mimic cellulitis)
- Marked swelling with loss of joint landmarks
- Low-grade fever and systemic malaise may accompany severe flares
- Desquamation of skin as flare resolves (peeling sign)
Diagnosis
Definitive diagnosis requires identification of negatively birefringent needle-shaped MSU crystals in synovial fluid or tophus aspirate under polarised light microscopy. In clinical practice, a presumptive diagnosis may be made based on characteristic clinical features, particularly in the context of known hyperuricaemia, tophi, or previous confirmed episodes.
| Feature | Gout (MSU) | CPPD | Septic Arthritis |
|---|---|---|---|
| Crystal morphology | Needle-shaped, negatively birefringent | Rhomboid, weakly positively birefringent | No crystals; positive Gram stain/culture |
| Classic joint | 1st MTP, midfoot, ankle | Knee, wrist, 2nd/3rd MCP | Knee (most common), hip |
| Onset | Rapid (6–24 h) | Rapid (hours–days) | Rapid |
| WCC (synovial fluid) | >2,000/µL, neutrophil-predominant | >2,000/µL, neutrophil-predominant | >50,000/µL (often >100,000) |
| Treatment | Colchicine, NSAIDs, steroids | NSAIDs, intra-articular steroids, colchicine | Urgent IV antibiotics + drainage |
Management of the Acute Flare
Treatment should be initiated as early as possible, ideally within 24 hours of symptom onset. Choice of agent depends on patient comorbidities, renal function, and concurrent medications.
First-Line Therapies
Intra-articular Corticosteroid Injection
For monoarticular or oligoarticular flares, intra-articular corticosteroid injection (e.g., methylprednisolone 40–80 mg or triamcinolone 20–40 mg depending on joint size) provides rapid and effective relief, particularly when systemic therapies are contraindicated. Ultrasound guidance improves accuracy for deeper joints.
IL-1 Inhibitors (Refractory Cases)
Anakinra (IL-1 receptor antagonist) 100 mg SC daily for 3–5 days may be considered in patients with contraindications or inadequate response to all first-line agents. It is not PBS-listed for gout but may be used off-label in specialist settings. Canakinumab is TGA-approved for gout but is not PBS-listed.
Chronic Tophaceous Gout
Chronic tophaceous gout represents the most severe end of the gout spectrum, characterised by visible or palpable tophi (aggregates of MSU crystals surrounded by a granulomatous inflammatory response), chronic inflammatory arthritis, and structural joint damage. It typically develops after 5–10 years of inadequately treated or untreated gout, though it may present earlier in patients with CKD, myeloproliferative disorders, or on cyclosporine therapy.
Clinical Features
- Tophi: firm nodules on extensor surfaces of fingers, olecranon bursae, Achilles tendons, pinnae of ears, and periarticular regions
- Chronic polyarticular joint inflammation with reduced range of motion
- Radiographic erosions with overhanging edges (rat-bite erosions) and relative preservation of joint space
- Tophus ulceration through skin with chalky white discharge
- Secondary osteoarthritic changes
- Urate nephrolithiasis and chronic urate nephropathy
Management Principles
The cornerstone of chronic tophaceous gout management is sustained serum urate lowering below 0.30 mmol/L (lower than the standard target of 0.36 mmol/L) to promote gradual tophus dissolution. Key principles include:
- Start ULT at low dose with gradual up-titration to minimise flare risk
- Mandatory flare prophylaxis with low-dose colchicine or low-dose NSAID for first 3–6 months of ULT (longer if tophi persist)
- Regular serum urate monitoring every 2–4 weeks during titration, then every 6 months once stable
- Combination therapy (xanthine oxidase inhibitor + uricosuric) may be required for refractory hyperuricaemia
- Patient education regarding medication adherence — ULT is typically lifelong
- Tophus resolution may take 6–36 months of sustained urate lowering
CPPD (Pseudogout)
Calcium pyrophosphate deposition (CPPD) disease encompasses a spectrum of clinical presentations unified by the deposition of calcium pyrophosphate dihydrate crystals in articular and periarticular tissues. CPPD is strongly age-related, affecting up to 25–50% of individuals over 80 years, and is visible as chondrocalcinosis on plain radiographs.
Clinical Presentations
Diagnosis
Definitive diagnosis: identification of weakly positively birefringent rhomboid CPP crystals in synovial fluid by compensated polarised light microscopy. Chondrocalcinosis on radiograph (calcification of hyaline cartilage or fibrocartilage) supports the diagnosis but is not specific.
Investigations for Underlying Metabolic Causes
CPPD in patients under 55 years, polyarticular involvement, or unusual joint distribution warrants investigation for underlying metabolic diseases:
- Serum calcium, phosphate, alkaline phosphatase, magnesium, ferritin, transferrin saturation
- Parathyroid hormone (hyperparathyroidism)
- Iron studies (haemochromatosis — HFE gene testing if elevated)
- Serum magnesium (hypomagnesaemia)
- Thyroid function tests
- Consider hypophosphatasia (low alkaline phosphatase) — rare but important
Treatment
No disease-modifying therapy for CPPD currently exists. Management is directed at symptom relief:
- Acute pseudogout: NSAIDs (first-line), intra-articular corticosteroid injection, colchicine (0.5 mg BD), or short course oral prednisolone
- Chronic pyrophosphate arthropathy: Paracetamol, low-dose NSAIDs, physiotherapy, intra-articular corticosteroid injections, joint replacement for end-stage disease
- Prophylaxis for recurrent acute pseudogout: Low-dose colchicine 0.5 mg daily; evidence is extrapolated from gout literature
- Treat underlying metabolic cause: Correction of hyperparathyroidism, haemochromatosis, or hypomagnesaemia may reduce recurrence
Urate-Lowering Therapy (ULT)
Indications for ULT Initiation
ULT should be considered in patients with:
- ≥2 gout flares per year
- Presence of tophi (clinical or imaging-detected)
- Radiographic evidence of gout-related joint damage
- Urate nephrolithiasis
- First flare with additional risk factors (eGFR <60, urate >0.54 mmol/L, young age at onset)
- CKD stage 3+ with any gout flare
Allopurinol — First-Line ULT
Febuxostat — Second-Line ULT
Uricosuric Agents
Flare Prophylaxis During ULT Initiation
Mandatory when starting or up-titrating ULT — continue for at least the first 3–6 months (longer if tophi present or flares continue):

HLA-B*5801 Testing
Rationale
HLA-B*5801 is a strong genetic risk factor for allopurinol-induced severe cutaneous adverse reactions (SCAR), including Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN). The allele frequency varies significantly by ethnicity:
| Population | HLA-B*5801 Allele Frequency | Testing Recommendation |
|---|---|---|
| Han Chinese | 6–8% | Mandatory |
| Korean | 6–8% | Mandatory |
| Thai | 6–12% | Mandatory |
| South-East Asian (general) | 2–8% | Mandatory |
| African American | 4–8% | Mandatory |
| Māori / Pacific Islander | 2–4% | Strongly recommended |
| ATSI populations | Data limited — consult local guidance | Consider testing |
| European / Caucasian | <1% | Not routinely required |
Australian Practice Points
- MBS item 71162 provides Medicare rebate for HLA-B*5801 genotyping — no out-of-pocket cost to patients when clinically indicated
- Testing is performed on a standard blood sample — results typically available within 7–14 business days
- If HLA-B*5801 positive: allopurinol is contraindicated. Use febuxostat (PBS Authority Required) or probenecid as alternatives
- If HLA-B*5801 negative: allopurinol may be commenced with standard precautions (low starting dose, gradual titration)
- HLA-B*5801 testing is not required for febuxostat or probenecid
- Additional risk factors for SCAR: CKD (especially eGFR <30), concurrent thiazide diuretics, rapid dose up-titration, female sex
Diet & Lifestyle Modifications
Dietary and lifestyle modifications are important adjuncts to pharmacotherapy in gout management. While dietary measures alone are rarely sufficient to normalise serum urate in patients with established gout, they can reduce flare frequency and are essential for addressing the metabolic comorbidities that frequently coexist.
Dietary Recommendations
- Low-fat dairy products (contain orotic acid, which promotes renal urate excretion)
- Cherries and cherry extract (associated with reduced flare risk — observational data)
- Coffee (regular consumption associated with lower serum urate — not decaf)
- Vitamin C supplementation (500 mg daily modestly reduces serum urate by ~0.05 mmol/L)
- Plant-based proteins (legumes, tofu) — lower risk than animal purines
- Complex carbohydrates, whole grains
- Organ meats (liver, kidney, sweetbreads — very high purine content)
- Shellfish, anchovies, sardines
- Red meat (limit to small portions)
- Beer and spirits (beer contains guanosine — a purine; spirits increase urate)
- Sugar-sweetened beverages and foods with high-fructose corn syrup
- Excessive fruit juice (fructose load)
Alcohol
Alcohol is a significant modifiable risk factor for gout. Beer has the strongest association due to its high guanosine (purine) content and the metabolic effects of ethanol on renal urate excretion. Spirits increase gout risk, while moderate wine consumption appears to have a weaker association. Recommendation: minimise alcohol, particularly beer and spirits. If consuming alcohol, limit to ≤2 standard drinks per day with at least 2 alcohol-free days per week.
Weight Management
Obesity is one of the strongest modifiable risk factors for gout. Weight loss (even 5–10% of body weight) reduces serum urate, decreases flare frequency, and improves metabolic comorbidities. Extreme fasting or crash dieting should be avoided as ketosis increases serum urate and may trigger flares.
Hydration
Maintaining adequate hydration (≥2 litres of water daily) promotes renal urate excretion and reduces risk of urate nephrolithiasis. This is particularly important for patients on uricosuric therapy (probenecid).
Exercise
Regular moderate exercise improves metabolic health, aids weight management, and may independently reduce gout risk. Avoid dehydration during exercise. High-intensity exercise that causes tissue breakdown may transiently increase serum urate.
Medication Review
Common medications that raise serum urate and should be reviewed:
- Thiazide and loop diuretics — consider alternatives (e.g., losartan, which has mild uricosuric properties)
- Low-dose aspirin — generally continued for cardiovascular indications despite effect on urate
- Ciclosporin — causes both hyperuricaemia and reduced renal urate excretion
- Pyrazinamide — used in tuberculosis treatment
- Ethambutol
- Tacrolimus
- Niacin (vitamin B3)
Monitoring
Serum Urate Monitoring
Assessing Tophus Resolution
- Clinical examination for tophi at each visit — document size, number, and location
- Ultrasound or dual-energy CT (DECT) may be used for objective tophi quantification
- Tophus resolution typically requires 6–36 months of sustained urate below 0.30 mmol/L
Flare Frequency Tracking
Maintain a flare diary. A reduction in flare frequency is one of the most clinically meaningful outcomes of successful ULT. Patients should be counselled that flares may increase in the first 3–6 months of ULT as previously deposited crystals mobilise — this does not indicate treatment failure.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Kuo CF, Grainge MJ, Mallen C, Zhang W, Doherty M. Rising burden of gout in the UK but continuing suboptimal management: a nationwide population study. Ann Rheum Dis. 2015;74(4):661-667. doi:10.1136/annrheumdis-2013-204463
- 2. Robinson PC, Taylor WJ, Merriman TR. Systematic review of the prevalence of gout and hyperuricaemia in Australia. Intern Med J. 2012;42(9):997-1007. doi:10.1111/j.1445-5994.2012.02835.x
- 3. Richette P, Doherty M, Pascual E, et al. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann Rheum Dis. 2017;76(1):29-42. doi:10.1136/annrheumdis-2016-209707
- 4. FitzGerald JD, Dalbeth N, Mikuls T, et al. 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis Care Res. 2020;72(6):744-760. doi:10.1002/acr.24180
- 5. Stamp LK, Chapman PT, Barclay ML, et al. A randomised controlled trial of the efficacy and safety of allopurinol dose optimization with serum urate target to treat gout in the New Zealand health system (ALLO): a study protocol. BMC Musculoskelet Disord. 2020;21(1):45. doi:10.1186/s12891-020-3052-6
- 6. White WB, Saag KG, Becker MA, et al. Cardiovascular safety of febuxostat or allopurinol in patients with gout (CARES trial). N Engl J Med. 2018;378(13):1200-1210. doi:10.1056/NEJMoa1710895
- 7. Hung SI, Chung WH, Liou LB, et al. HLA-B*5801 allele as a genetic marker for severe cutaneous adverse reactions caused by allopurinol. Proc Natl Acad Sci USA. 2005;102(11):4134-4139. doi:10.1073/pnas.0409500102
- 8. Dalbeth N, Gosling AL, Gaffo A, Abhishek A. Gout. Lancet. 2021;397(10287):1843-1855. doi:10.1016/S0140-6736(21)00569-9
- 9. Zhang W, Doherty M, Bardin T, et al. European League Against Rheumatism recommendations for calcium py