📋 Key Information Summary
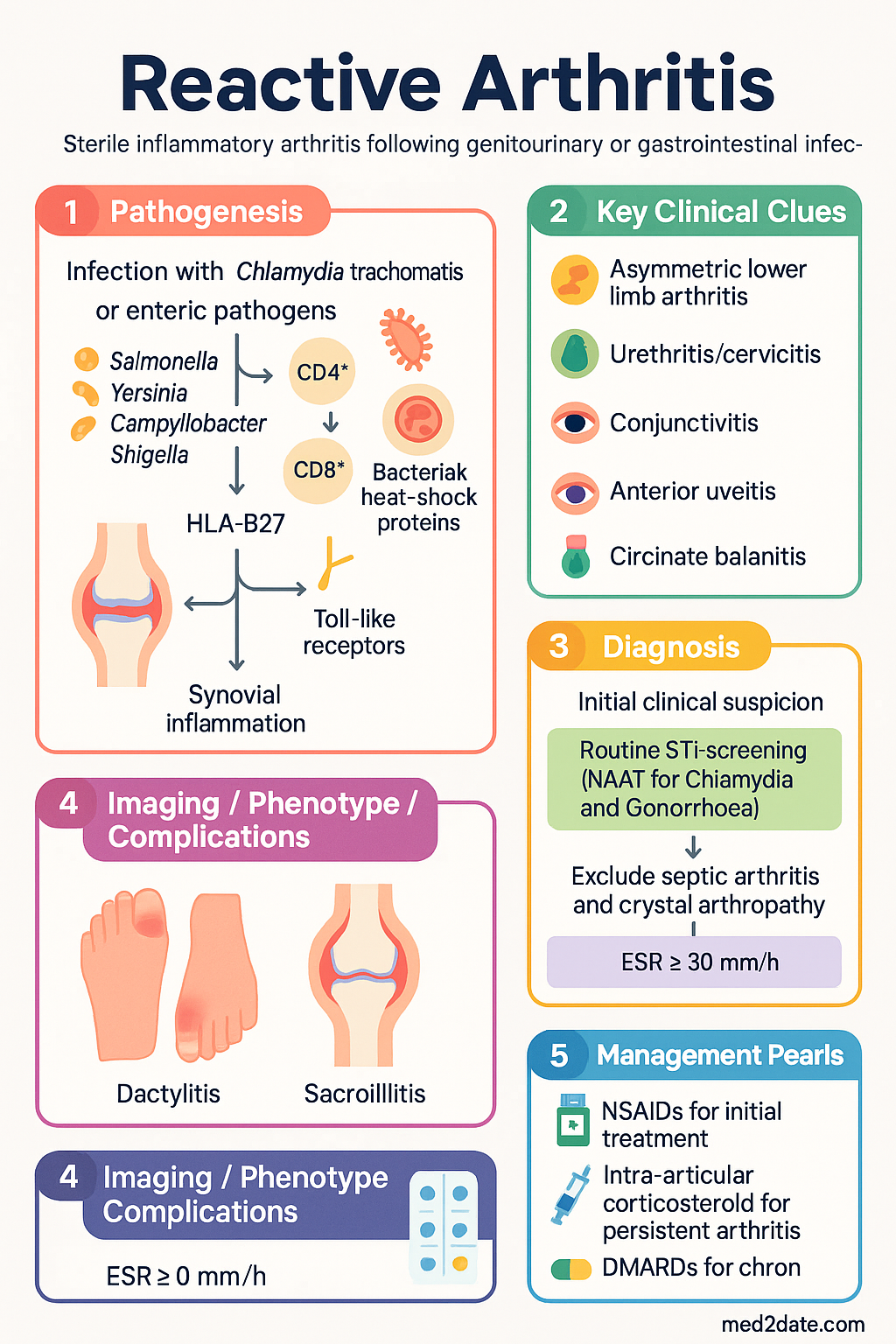
- Definition: Reactive arthritis (ReA) is a sterile, inflammatory arthritis occurring 1–4 weeks after a genitourinary or gastrointestinal infection, typically involving the lower limbs asymmetrically.
- Classic triad (Reiter syndrome): Arthritis + urethritis/cervicitis + conjunctivitis — though the full triad is present in only ~30% of cases.
- Key triggers: Chlamydia trachomatis (urogenital) and enteric pathogens — Salmonella, Yersinia, Campylobacter, Shigella.
- HLA-B27: Present in 60–80% of patients; associated with more severe disease, sacroiliitis, and chronicity.
- Diagnosis: Clinical — no single confirmatory test. Arthritis with characteristic timing following a documented infection; exclude septic arthritis and crystal arthropathy.
- Extra-articular features: Anterior uveitis (15–25%), circinate balanitis, keratoderma blennorrhagicum, enthesitis, dactylitis.
- First-line treatment: NSAIDs (naproxen 500 mg BD or indomethacin 25–50 mg TDS); use lowest effective dose for shortest duration.
- Intra-articular corticosteroids for persistent mono- or oligoarthritis; systemic corticosteroids reserved for refractory cases.
- DMARDs: Sulfasalazine 500 mg BD up to 1 g BD (PBS Authority Required) for chronic/remitting disease ≥6 weeks; methotrexate if sulfasalazine fails.
- Antibiotics: NOT recommended for established arthritis (no benefit in RCTs); however, treat any active concurrent Chlamydia infection with doxycycline 100 mg BD × 7 days.
- Prognosis: ~60–75% achieve complete remission within 6–12 months; ~15–20% develop chronic disease; HLA-B27-positive patients have higher relapse risk.
- ATSI considerations: Higher rates of enteric infections in remote communities; increased Chlamydia prevalence; barriers to rheumatology access.
- Referral: Ophthalmology urgently if uveitis suspected (red eye + pain + photophobia); rheumatology if arthritis persists >6 weeks or DMARD therapy considered.
Introduction & Australian Epidemiology
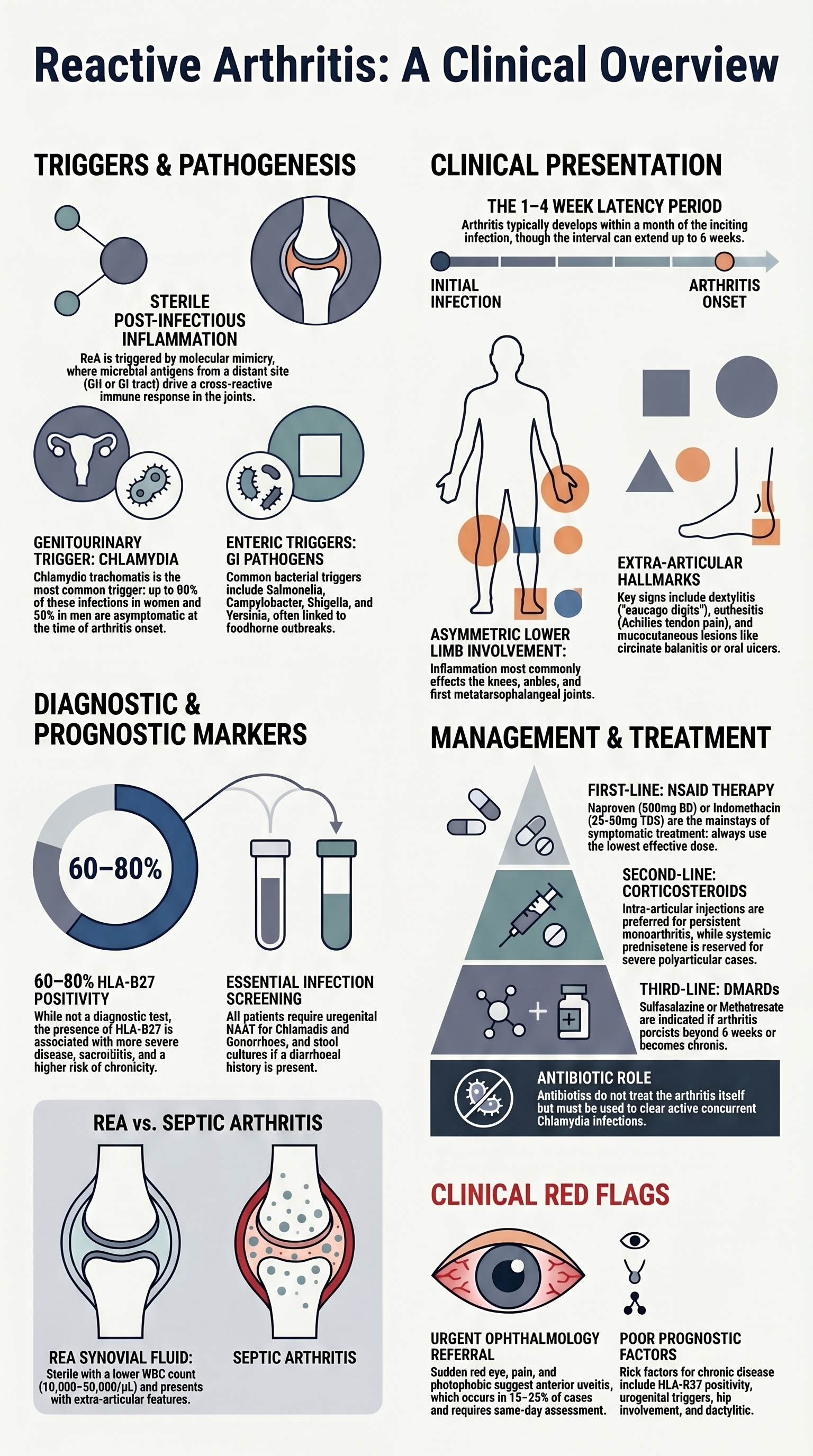
Reactive arthritis (ReA) is a form of spondyloarthropathy characterised by sterile inflammation of the joints and entheses following a remote infection, typically of the genitourinary or gastrointestinal tract. The term "reactive" was introduced by Ahvonen et al. in 1969 to describe arthritis developing after Yersinia infection, and has largely replaced the older eponym "Reiter syndrome," which is now considered eponymously inappropriate given Hans Reiter's association with Nazi-era human experimentation.
In Australia, ReA is estimated to account for approximately 3–5% of new presentations to rheumatology clinics. The urogenital form predominates in sexually active adults aged 20–40 years, while the post-enteric form affects all age groups and is often linked to foodborne outbreaks. The Australian Institute of Health and Welfare (AIHW) data indicate that spondyloarthropathy collectively affects approximately 0.3–0.5% of the Australian population, with ReA representing a significant proportion of new-onset inflammatory arthritis referrals.
Post-Chlamydia ReA is likely underdiagnosed because many genitourinary infections are asymptomatic. Enteric-triggered ReA may present in clusters following documented outbreaks of Salmonella or Campylobacter, which are notifiable conditions under Australian state and territory public health legislation. The incidence is higher in Aboriginal and Torres Strait Islander communities due to greater exposure to enteric pathogens and higher rates of sexually transmitted infections (STIs).
Postinfectious Arthritis
Reactive arthritis is the prototypical postinfectious arthritis — an inflammatory joint disease triggered by a distant infection but with no viable organisms recovered from synovial fluid or tissue. The mechanism involves molecular mimicry, whereby microbial antigens (particularly peptides from Chlamydia or enteric bacteria) share structural homology with self-antigens in the joint, leading to a cross-reactive immune response.
Pathogenic Mechanisms
- Molecular mimicry: Bacterial heat-shock proteins (GroEL/Hsp60) and outer-membrane proteins resemble human joint antigens, driving CD4+ and CD8+ T-cell responses within the synovium.
- Bacterial persistence: Particularly with Chlamydia trachomatis, there is evidence of aberrant, persistent forms (reticulate bodies) within the synovium that may drive ongoing inflammation without replicating.
- Innate immune activation: Toll-like receptor (TLR) stimulation by bacterial lipopolysaccharide (LPS) and peptidoglycan fragments activates macrophages and neutrophils in the synovial membrane.
- Genetic susceptibility: HLA-B27 presents microbial peptides aberrantly, promoting cytotoxic T-cell responses; the MHC class I allele also alters intracellular bacterial handling (HLA-B27 misfolding hypothesis).
Temporal Relationship
Arthritis typically develops 1–4 weeks after the inciting infection, though intervals of up to 6 weeks have been described. The index infection may be clinically apparent (diarrhoea, urethritis) or entirely subclinical — particularly relevant for Chlamydia, where up to 70–80% of urogenital infections in women and 50% in men are asymptomatic.
Distinguishing Postinfectious Arthritis from Septic Arthritis
| Feature | Reactive Arthritis | Septic Arthritis |
|---|---|---|
| Synovial fluid culture | Sterile | Positive (usually S. aureus) |
| WBC count | 10,000–50,000/µL | Usually >50,000/µL |
| Pattern | Asymmetric, oligoarticular, lower limb | Usually monoarticular |
| Systemic toxicity | Mild–moderate | Fever, rigors, sepsis |
| Extra-articular features | Uveitis, skin, enthesitis | Absent |
| Antibiotic response | No benefit for arthritis | Essential treatment |
Chlamydia-Associated Triggers
Chlamydia trachomatis (serovars D–K) is the most common trigger for urogenital reactive arthritis in Australia and globally. The estimated incidence of ReA following urogenital Chlamydia infection is 1–4%, though this may be an underestimate given asymptomatic carriage.
Key Features of Chlamydia-Triggered ReA
- More common in males (M:F ratio approximately 5:1 for urogenital form).
- HLA-B27 present in 60–80% of affected individuals.
- Conjunctivitis and anterior uveitis are more common with Chlamydia-triggered ReA than enteric forms.
- Circinate balanitis (painless shallow ulcers on the glans penis) occurs in ~20–40% of male patients.
- Asymptomatic Chlamydia persistence is the putative mechanism — aberrant reticulate bodies within the synovium drive chronic inflammation.
Diagnosis of Chlamydia Trigger
- Nucleic acid amplification test (NAAT): First-line investigation — urine or urogenital swab for C. trachomatis DNA. Available through all Australian pathology providers; MBS-rebated.
- Serology: Anti-Chlamydia IgG/IgA may indicate past infection but is not specific for the reactive arthritis trigger and has limited diagnostic utility.
- Synovial fluid/tissue PCR: Research setting; not routinely available in Australia. May demonstrate Chlamydia DNA in synovial tissue even when urogenital NAAT is negative.
Enteric Triggers
Post-dysenteric reactive arthritis follows gastrointestinal infection with Salmonella (non-typhoidal), Shigella, Yersinia, or Campylobacter species. These organisms are notifiable under Australian state and territory public health legislation, and outbreaks are monitored by OzFoodNet and state health departments.
| Organism | ReA Incidence Post-Infection | HLA-B27 Prevalence | Australian Context |
|---|---|---|---|
| Salmonella spp. | 6–15% | 60–70% | Common cause; linked to poultry and egg outbreaks. Notifiable nationally. |
| Campylobacter spp. | 1–5% | ~50% | Most common bacterial enteric pathogen in Australia; linked to undercooked poultry. |
| Shigella spp. | 7–15% | 70–80% | Endemic in some Aboriginal communities; MSM transmission increasing. |
| Yersinia spp. | 10–25% | 60–75% | Less common in Australia; associated with pork and dairy products. |
Clinical Features of Enteric-Reactive Arthritis
- Onset 1–4 weeks after the diarrhoeal illness (which may be mild or self-limiting).
- Asymmetric oligoarthritis predominantly affecting the knees, ankles, and metatarsophalangeal joints.
- Lower frequency of urethritis and circinate balanitis compared with Chlamydia-triggered ReA.
- HLA-B27-positive patients more likely to develop sacroiliitis and chronic disease.
- Enteric-triggered ReA tends to have a more self-limiting course than urogenital-triggered ReA.
Investigation of Enteric Trigger
- Stool culture and multiplex PCR (GI pathogen panel) — available at all major Australian pathology providers (MBS-rebated).
- Serology for Yersinia (anti-Yop antibodies) — limited availability; request through reference laboratories.
- Blood cultures if febrile or systemically unwell (to exclude concurrent bacteraemia).
Extra-Articular Features
Reactive arthritis is a systemic inflammatory condition with multiple potential extra-articular manifestations. Recognition of these features is essential for diagnosis and comprehensive management.
Mucocutaneous Manifestations
- Circinate balanitis: Painless shallow erosions on the glans penis or urethral meatus; present in 20–40% of male patients. Does not require specific treatment beyond topical emollients.
- Keratoderma blennorrhagicum: Hyperkeratotic, psoriasiform lesions on the soles, palms, and around nails. Resembles pustular psoriasis. Topical corticosteroids or vitamin D analogues (calcipotriol) may be used.
- Oral ulcers: Painless shallow erosions on the palate, tongue, or buccal mucosa; usually transient.
- Nail changes: Onycholysis, subungual hyperkeratosis — indistinguishable from psoriatic nail disease.
Ocular Manifestations
- Conjunctivitis: Bilateral, mild, self-limiting; part of the classic triad but may be missed.
- Anterior uveitis: Typically unilateral; may be recurrent. HLA-B27-positive patients have higher recurrence rates.
- Episcleritis: Less common; presents with sectoral injection and mild discomfort.
Urethritis
- Sterile urethral discharge, dysuria, or increased urinary frequency.
- May be triggered by or coexist with active Chlamydia trachomatis infection — always perform NAAT.
- Cervicitis in female patients may be asymptomatic.
Enthesitis & Dactylitis
- Enthesitis: Inflammation at tendinous insertions — Achilles tendon insertion (most common), plantar fascia, patellar tendon, tibial tuberosity. Present in 40–70% of cases.
- Dactylitis: "Sausage digits" — diffuse swelling of an entire digit due to flexor tenosynovitis and joint inflammation. A hallmark of spondyloarthropathy.
Constitutional Symptoms
- Fatigue, malaise, low-grade fever, and weight loss may occur, particularly in the acute phase.
- Psoriasiform skin lesions, onychodystrophy, and conjunctivitis can mimic psoriatic arthritis — differentiation requires careful history regarding the preceding infection.
HLA-B27 Association
Human leucocyte antigen B27 (HLA-B27) is a major histocompatibility complex (MHC) class I molecule present in 6–8% of the general Australian population but in 60–80% of patients with reactive arthritis. Its presence is a major determinant of disease susceptibility, severity, and chronicity.
Role of HLA-B27 in Reactive Arthritis
- Increased susceptibility: HLA-B27-positive individuals are 10–50× more likely to develop ReA following a triggering infection.
- Sacroiliitis and axial disease: HLA-B27 is strongly associated with sacroiliac joint involvement and progression to ankylosing spondylitis-like phenotype.
- Chronicity: Patients who are HLA-B27-positive have higher rates of persistent arthritis (>6 months) and relapse.
- Extra-articular features: Uveitis and cardiac conduction abnormalities are more common in HLA-B27-positive patients.
- Not diagnostic: HLA-B27 testing alone cannot confirm or exclude ReA. Approximately 20–40% of ReA patients are HLA-B27-negative.
Proposed Mechanisms
- Arthritogenic peptide hypothesis: HLA-B27 presents bacterial peptides (e.g., from Chlamydia or Salmonella) that cross-react with self-peptides on joint surfaces.
- HLA-B27 misfolding: The HLA-B27 heavy chain tends to misfold in the endoplasmic reticulum, activating the unfolded protein response (UPR) and IL-23/IL-17 axis.
- Altered intracellular killing: HLA-B27 transgenic models show impaired clearance of intracellular Chlamydia and Salmonella, potentially promoting persistent infection.
Testing for HLA-B27 in Australia
Clinical Presentation & Diagnostic Criteria
Typical Presentation
A previously well patient, typically aged 20–40 years, presents with acute-onset asymmetric oligoarthritis predominantly affecting the lower limbs — knees, ankles, and first metatarsophalangeal joint (MTP) are most commonly involved. There is often a history of preceding urethritis (1–4 weeks prior) or diarrhoeal illness (1–4 weeks prior), though the preceding infection may be subclinical.
Diagnostic Criteria
There is no universally accepted gold-standard diagnostic criterion for ReA. The diagnosis remains clinical and is one of exclusion. The following frameworks are commonly used:
| Criterion Set | Key Features |
|---|---|
| Berlin criteria (1979, modified) | Asymmetric arthritis + evidence of preceding or concurrent infection + absence of other causes of arthritis. Does not require HLA-B27. |
| Classification of Spondyloarthropathies (Amor / ESSG) | ReA is classified under spondyloarthropathy umbrella. Inflammatory arthritis + preceding infection = sufficient for classification. |
| BASDAI / ASAS criteria | Primarily used for axial spondyloarthropathy; apply if sacroiliitis or axial symptoms are prominent. |
Differential Diagnosis
- Septic arthritis: Always exclude — aspirate synovial fluid urgently for cell count, Gram stain, and culture.
- Crystal arthropathy: Gout and pseudogout — synovial fluid polarised microscopy.
- Rheumatoid arthritis: Symmetric, small joints, RF/anti-CCP positive.
- Psoriatic arthritis: Skin/nail psoriasis, dactylitis, enthesitis — overlap with ReA is significant.
- Gonococcal arthritis: Disseminated N. gonorrhoeae — tenosynovitis, dermatitis, polyarthralgia; culture or NAAT positive.
- Ankylosing spondylitis: Chronic axial involvement with sacroiliitis; may evolve from ReA in HLA-B27-positive individuals.
- Viral arthritis: Parvovirus B19, rubella, hepatitis B — typically polyarticular and self-limiting.
Investigations
Investigations in ReA serve three purposes: (1) excluding septic arthritis and other differentials, (2) identifying the triggering infection, and (3) assessing disease severity and chronicity.
Baseline Blood Tests
Infection Screening
Synovial Fluid Analysis
Imaging
Risk Stratification & Prognostic Factors
Identifying patients at risk of chronic disease is essential for guiding treatment intensity and follow-up frequency.
Poor Prognostic Factors
- HLA-B27 positivity
- Urogenital (vs enteric) trigger
- Hip or shoulder involvement
- Elevated ESR/CRP persisting >3 months
- Dactylitis
- Sacroiliitis on imaging
- Inadequate initial response to NSAIDs
- Recurrent episodes
Treatment & Prognosis
First-Line: NSAIDs
NSAIDs are the mainstay of symptomatic treatment for reactive arthritis. Use the lowest effective dose for the shortest duration necessary. In Australia, two NSAIDs are commonly prescribed:
Second-Line: Corticosteroids
- Intra-articular corticosteroid injection: Triamcinolone acetonide 20–40 mg (knee) or 10–20 mg (ankle, MTP) — effective for persistent mono- or oligoarthritis despite NSAIDs. Perform under sterile conditions after excluding septic arthritis. PBS General Benefit (medical service).
- Systemic corticosteroids: Prednisolone 15–25 mg PO daily, tapered over 4–6 weeks. Reserved for severe polyarticular disease or significant extra-articular features refractory to NSAIDs. Use lowest dose for shortest duration.
Third-Line: DMARDs (Chronic/Refractory Disease)
DMARDs are considered when arthritis persists beyond 6 weeks despite NSAIDs and corticosteroids, or in patients with frequent relapses. The evidence base for DMARDs in ReA is limited, primarily from small trials and observational studies.
Antibiotics for Active Chlamydia Infection
Antibiotic therapy for the arthritis itself has NOT been shown to be beneficial in randomised controlled trials (including the STOP-REA and CLAIRTHRITIS trials). However, if there is evidence of active concurrent Chlamydia trachomatis infection (positive NAAT), treat the infection as per Australian STI management guidelines:
Prognosis
Complete remission within 6–12 months with NSAID therapy alone. Enteric-triggered ReA generally has a better prognosis than urogenital-triggered ReA. Most patients do not develop chronic disease.
Persistent arthritis >6 months. May evolve into undifferentiated spondyloarthropathy or, in HLA-B27-positive patients, ankylosing spondylitis. Requires long-term DMARD therapy and rheumatology follow-up.
Follow-Up
- Review at 4–6 weeks post-diagnosis: assess NSAID response, symptom trajectory, and extra-articular features.
- If improving: continue NSAIDs with plan to wean over 2–4 weeks as symptoms resolve.
- If not improving at 6 weeks: refer rheumatology for DMARD consideration.
- Ophthalmology review if anterior uveitis develops at any stage (urgent referral).
- Sexual health screening and partner notification for Chlamydia-triggered ReA.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Reactive arthritis has particular significance in Aboriginal and Torres Strait Islander communities due to higher rates of both enteric infections and sexually transmitted infections, including Chlamydia trachomatis. The disproportionate burden of ReA reflects broader social determinants of health, including overcrowded housing, limited access to clean water and sanitation in remote communities, and barriers to healthcare access.
Key Considerations
Recommended Actions
- Incorporate enteric and STI screening into routine health assessments for Aboriginal and Torres Strait Islander patients (MBS 715 Health Assessment).
- Ensure rheumatology referrals are facilitated through ACCHOs and Indigenous-specific care pathways where available.
- Utilise telehealth for specialist consultations (MBS items 91822–91826).
- Consider Closing the Gap PBS co-payment for medication access.
- Engage Aboriginal Health Workers in patient education and follow-up coordination.
- Advocate for improved environmental health infrastructure to reduce enteric infection burden.