📋 Key Information Summary
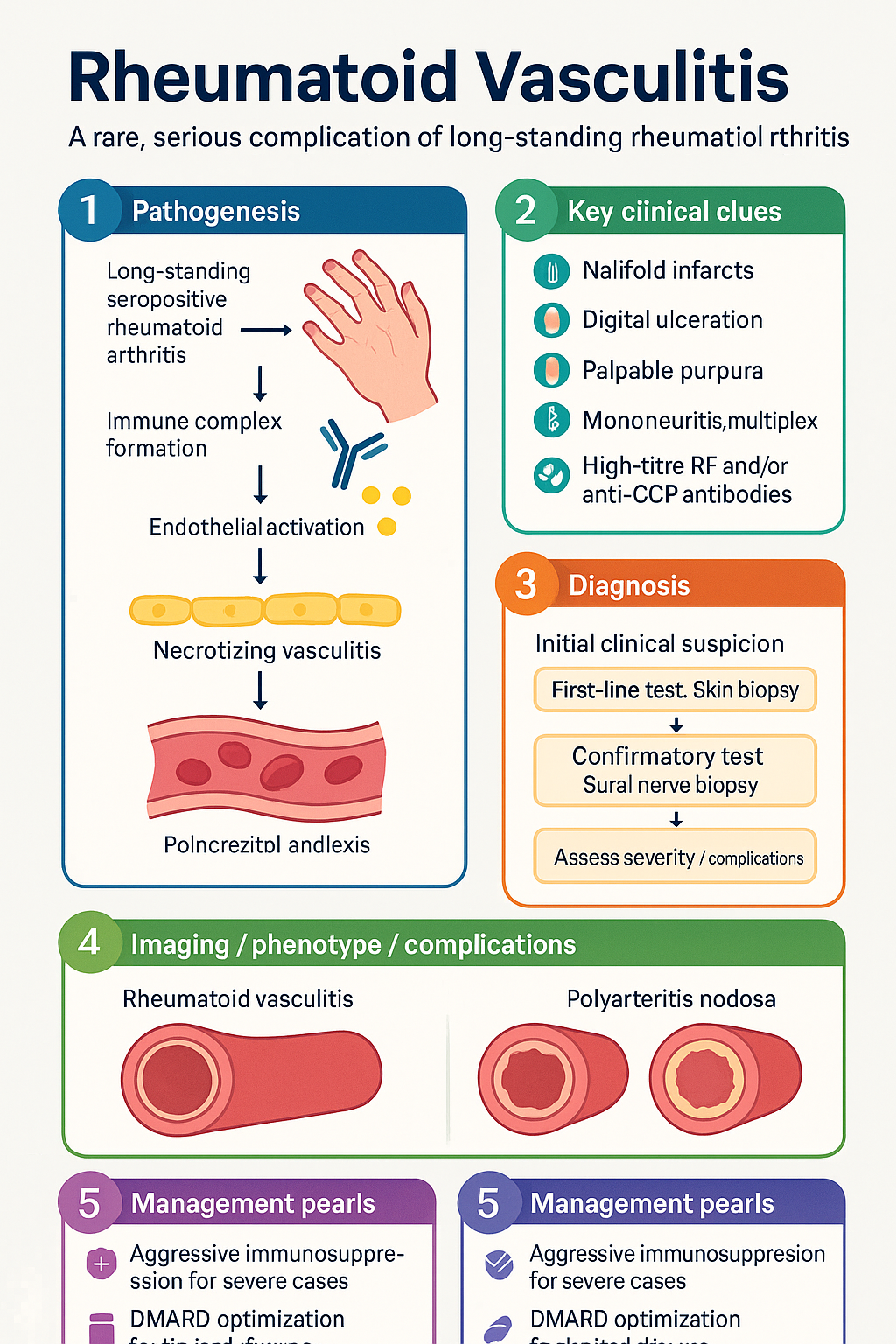
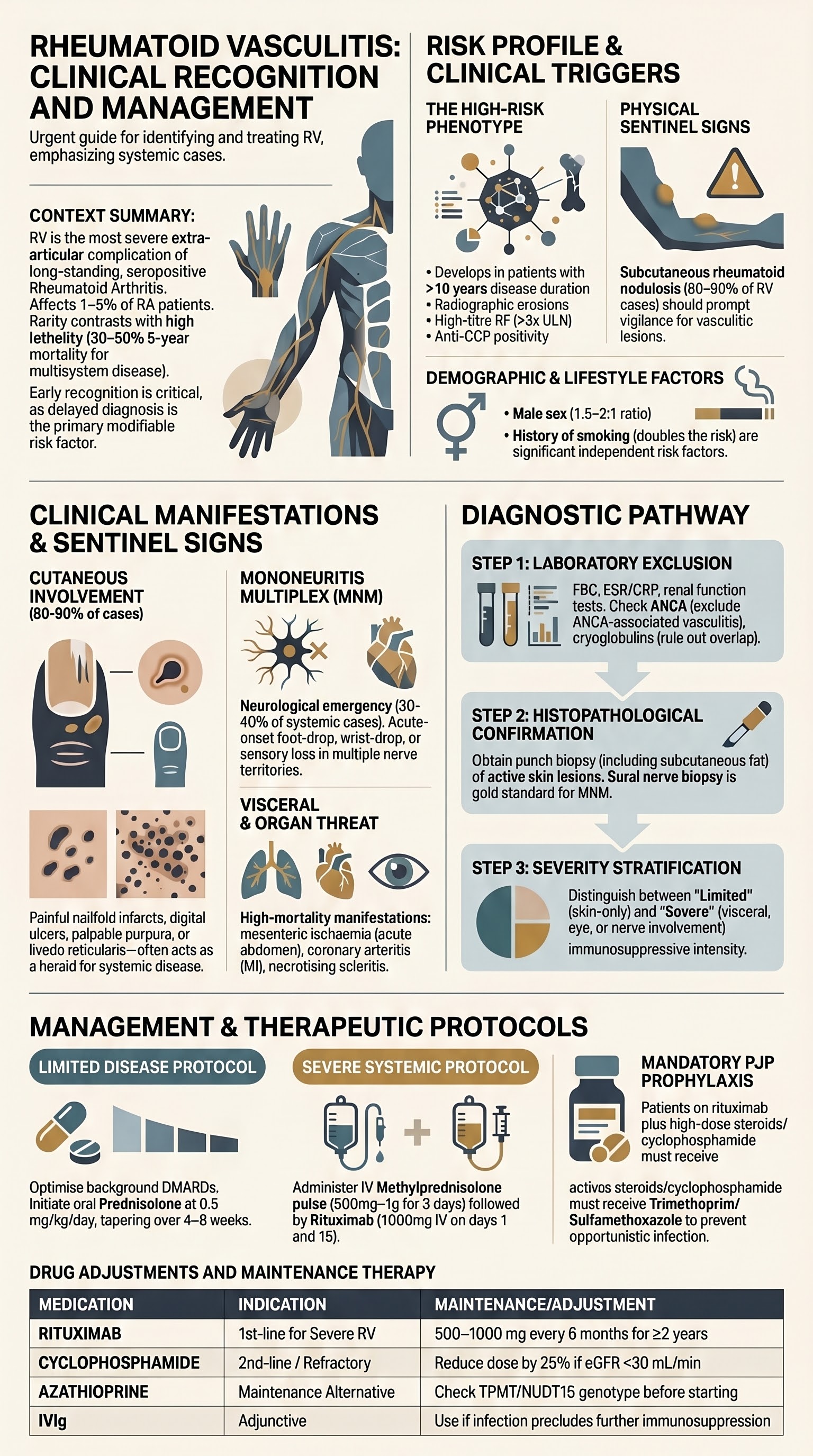
- Rheumatoid vasculitis (RV) is a rare, serious extra-articular complication of long-standing seropositive rheumatoid arthritis, occurring in approximately 1–5% of patients with RA.
- Key risk factors include long disease duration (>10 years), high-titre rheumatoid factor (RF) and/or anti-CCP antibodies, male sex, smoking history, persistent joint erosions, and prior nodulosis.
- Cutaneous manifestations are the most common presentation — nailfold infarcts, digital ulceration, palpable purpura, and livedo reticularis — and should prompt urgent vasculitis workup.
- Mononeuritis multiplex (acute onset of foot-drop, wrist-drop, or sensory loss in multiple nerve territories) is a hallmark of moderate-to-severe RV and indicates ischaemic nerve damage.
- Visceral involvement can affect the mesenteric circulation (acute abdomen), coronary arteries (MI), pulmonary parenchyma, and kidneys (necrotising glomerulonephritis), with high morbidity and mortality.
- Diagnosis requires tissue biopsy (skin, sural nerve) demonstrating necrotising or leucocytoclastic vasculitis of small-to-medium vessels; ANCA should be checked to exclude ANCA-associated vasculitis.
- Severity is stratified into limited (cutaneous-only) vs. severe (mononeuritis multiplex, visceral, scleritis) — severe disease demands aggressive immunosuppression.
- Limited skin-only RV: optimise DMARDs, add short course of oral prednisolone 0.5 mg/kg/day tapering over 4–8 weeks.
- Severe RV (nerve, eye, visceral): IV methylprednisolone 500 mg–1 g daily × 3 days then oral taper, PLUS rituximab 1000 mg IV × 2 (days 1 and 15) — first-line per RAVE/EUVAS evidence; cyclophosphamide is second-line.
- Intravenous immunoglobulin (IVIg) 2 g/kg over 2–5 days may be used adjunctively or when infection precludes further immunosuppression.
- RV carries significant mortality (5-year mortality 30–50% for severe multisystem disease); early recognition and aggressive treatment improve outcomes.
- PJP prophylaxis with trimethoprim/sulfamethoxazole is mandatory for patients receiving intensive immunosuppression (rituximab + high-dose corticosteroids or cyclophosphamide).
- Aboriginal and Torres Strait Islander patients may present later with more advanced disease due to healthcare access barriers; culturally safe outreach vasculitis screening should be integrated into chronic disease programmes.
- All patients should be managed in conjunction with rheumatology and, for visceral or neurological involvement, a vasculitis or combined rheumatology–immunology centre of expertise.
Introduction & Australian Epidemiology
Rheumatoid vasculitis (RV) is a necrotising vasculitis affecting small and medium-sized arteries that occurs as an extra-articular manifestation of rheumatoid arthritis (RA). It is distinct from other ANCA-associated vasculitides and represents the most severe extra-articular complication of RA, carrying substantial morbidity and mortality.
The prevalence of RV has declined significantly since the introduction of early aggressive DMARD therapy and biologic agents for RA. Historical series reported 1–5% of RA patients; contemporary Australian data suggest an incidence below 0.5% in patients on modern treat-to-target regimens. However, RV remains an important diagnosis to recognise because of its devastating complications when untreated.
In Australia, RV is managed primarily by rheumatologists with access to vasculitis expertise at tertiary centres (e.g., Royal Adelaide Hospital Vasculitis Clinic, Royal Melbourne Hospital, St Vincent's Sydney, Royal Perth Hospital). Referral to a multidisciplinary vasculitis team is strongly recommended for all patients with suspected severe or systemic RV.
Risk Factors in Long-Standing RA
Rheumatoid vasculitis develops almost exclusively in patients with established, seropositive, erosive RA. The following risk factors have been consistently identified in cohort studies:
| Risk Factor | Detail | Evidence Strength |
|---|---|---|
| Disease duration | Typically >10 years; median 15–20 years at presentation | Strong |
| Seropositivity | High-titre RF (>3× ULN); anti-CCP positivity adds independent risk | Strong |
| Rheumatoid nodulosis | Subcutaneous nodules present in 80–90% of RV patients | Strong |
| Male sex | Male-to-female ratio approximately 1.5–2:1 in RV (cf. 3:1 F:M in RA overall) | Moderate |
| Smoking | Current or ex-smoking doubles risk; dose-dependent relationship | Strong |
| Erosive disease | Radiographic erosions present in virtually all RV patients | Strong |
| Previous extra-articular features | Prior episcleritis, pleuritis, Felty syndrome increase risk | Moderate |
| HLA-DRB1 shared epitope | Homozygosity for shared epitope alleles associated with severe extra-articular RA | Moderate |
| Drug factors | Methotrexate withdrawal or dose reduction may unmask latent vasculitis in some cases | Limited |
Cutaneous Manifestations
Skin involvement is the most common presentation of RV, occurring in 80–90% of cases. Cutaneous RV exists on a spectrum from limited (skin-only) to a harbinger of systemic disease.
Nailfold Infarcts (Splinter Haemorrhages)
Small, dark, linear haemorrhages in the nail bed representing distal digital arteriolar occlusion. While common in active RA without vasculitis, the presence of multiple new, painful nailfold infarcts — especially with perungual erythema — raises concern for vasculitis.
Digital Ulceration
Punched-out, painful ulcers at the fingertips (over digital pulps) or periungual areas. These result from small-vessel occlusion and are often bilateral. Deep ulcers that extend to bone carry risk of digital gangrene and amputation.
Livedo Reticularis
A violaceous, net-like mottling pattern most visible on the lower extremities and trunk. In the context of RV, livedo indicates medium-vessel involvement and may be associated with a more aggressive disease course and higher likelihood of visceral disease.
Other Cutaneous Features
- Palpable purpura: Leucocytoclastic vasculitis on histopathology; most common histological finding in RV skin biopsies.
- Deep dermal nodules: Tender nodules on extensor surfaces mimicking rheumatoid nodules but with vasculitic histopathology.
- Pyoderma gangrenosum-like ulceration: Large, undermined, necrotic ulcers — a severe cutaneous manifestation.
- Leg ulceration: Often multifactorial (venous + vasculitic); biopsy essential to distinguish.
Mononeuritis Multiplex
Mononeuritis multiplex (MNM) is a hallmark of moderate-to-severe rheumatoid vasculitis and is present in approximately 30–40% of patients with systemic RV. It results from ischaemic damage to the vasa nervorum of peripheral nerves.
Clinical Features
- Acute onset (hours to days) of asymmetric motor and/or sensory deficits in the distribution of two or more named peripheral nerves.
- Common patterns: Foot-drop (common peroneal nerve), wrist-drop (radial nerve), sensory loss in superficial peroneal or sural nerve territories.
- Often preceded by severe neuropathic pain in the affected limb.
- May progress to polyneuropathy if untreated — confluent mononeuritis multiplex mimicking distal symmetric polyneuropathy.
Investigations
- Nerve conduction studies (NCS) / electromyography (EMG): Confirm axonal pattern mononeuritis multiplex (reduced CMAP/SNAP amplitudes with preserved conduction velocities). MBS item 12300 (nerve conduction studies).
- Sural nerve biopsy: Gold standard — demonstrates necrotising arteritis of the vasa nervorum with fibrinoid necrosis. Reserve for diagnostic uncertainty or when skin biopsy is non-diagnostic.
- Exclude mimics: Diabetic mononeuropathy, compressive neuropathies, vasculitis from other aetiologies (PAN, EGPA).
Visceral Involvement
Visceral involvement in RV is less common than cutaneous or neurological disease but carries the highest mortality. Any organ system supplied by small-to-medium arteries can be affected.
| Organ System | Manifestation | Frequency | Key Investigations |
|---|---|---|---|
| Mesenteric / GI | Bowel ischaemia, perforation, acute abdomen | 5–10% | CT angiography abdomen/pelvis; surgical consultation |
| Coronary | Vasculitic coronary arteritis → myocardial infarction | Rare | ECG, troponin, coronary angiography |
| Pulmonary | Parenchymal vasculitis, pulmonary haemorrhage, cavitating nodules | 5–10% | HRCT chest, bronchoscopy with BAL (haemosiderin-laden macrophages) |
| Renal | Necrotising glomerulonephritis (pauci-immune pattern) | 5–15% | Urinalysis, serum creatinine, renal biopsy |
| Ocular | Scleritis (necrotising), peripheral ulcerative keratitis (PUK) | 10–15% | Slit-lamp examination by ophthalmology; urgent referral |
| CNS | Cerebral vasculitis (rare), stroke | <5% | MRI brain with MRA, CSF analysis, exclude embolic/thrombotic causes |
Diagnosis & Biopsy
There are no validated classification criteria specific to rheumatoid vasculitis. Diagnosis is based on clinical features of vasculitis in a patient with established RA, after exclusion of other causes. Tissue biopsy confirming vasculitis is highly desirable.
Diagnostic Approach
- Step 1 — Clinical suspicion: New vasculitic-appearing skin lesions, mononeuritis multiplex, scleritis, or visceral ischaemia in a patient with seropositive RA.
- Step 2 — Exclude mimics: ANCA-associated vasculitis (check c-ANCA/PR3, p-ANCA/MPO), cryoglobulinaemia, infective endocarditis, cholesterol emboli, drug-induced vasculitis, polyarteritis nodosa.
- Step 3 — Tissue biopsy: Skin biopsy of active lesion (punch biopsy including subcutaneous fat) is the first-line approach. Sural nerve biopsy if neuropathy present and skin biopsy non-diagnostic.
- Step 4 — Assess extent: Full systemic workup to determine limited vs. severe disease (see Severity Stratification below).
Biopsy Findings in RV
| Biopsy Site | Histopathology | Sensitivity |
|---|---|---|
| Skin (active lesion) | Leucocytoclastic vasculitis of dermal vessels; fibrinoid necrosis; perivascular neutrophilic infiltrate with nuclear dust | 60–80% (palpable purpura highest yield) |
| Sural nerve | Necrotising arteritis of epineural vessels; axonal degeneration | 80–90% when MNM present |
| Kidney | Pauci-immune necrotising crescentic GN (may be ANCA-negative) | Variable |
| GI tract | Transmural necrotising arteritis; mucosal ulceration | Usually surgical specimen |
Laboratory Investigations
Risk Stratification / Severity Scoring
RV is classified into limited (cutaneous-only) and severe (systemic) disease. This distinction drives therapeutic intensity.
Empirical Therapy
Treatment of RV is not protocolised in the same way as ANCA-associated vasculitis, but management principles are similar. All severe RV should be managed in conjunction with a vasculitis or specialist rheumatology centre.
Limited (Cutaneous-Only) Disease
Concurrently optimise background DMARD therapy (methotrexate, leflunomide, or sulfasalazine). Adding or increasing hydroxychloroquine 200 mg BD may be considered for mild cutaneous disease.
Moderate-to-Severe Systemic Disease — 1st-Line
2nd-Line / Refractory Disease
Adjunctive Therapy
Directed / Pathogen-Specific and Mechanism-Specific Therapy
Rituximab has emerged as the preferred B-cell depleting agent for severe RV based on extrapolation from RAVE and RITUXVAS trials in ANCA-associated vasculitis and observational data in RV specifically. Its mechanism — B-cell depletion reducing RF-producing and autoantibody-producing B lymphocytes — is well-suited to the pathophysiology of RV.
Therapy by Disease Severity
Maintenance Therapy After Induction
- Rituximab maintenance: 500–1000 mg IV every 6 months for a minimum of 2 years, guided by relapse risk. Monitor CD19+ B-cell count and immunoglobulin levels.
- Azathioprine alternative: 2 mg/kg/day PO (check TPMT/NUDT15 genotype before commencing) as maintenance if rituximab not tolerated or unavailable.
- Mycophenolate mofetil: 1–1.5 g BD PO — may be used as steroid-sparing agent in maintenance; limited evidence in RV specifically.
- Methotrexate: Continue background MTX for RA disease control; may be continued through rituximab therapy at reduced dose.
Monitoring
RV requires close monitoring during both induction and maintenance phases, for disease activity, treatment toxicity, and infection risk.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Makol A, Matteson EL, Warrington KJ. Rheumatoid vasculitis: an update. Curr Opin Rheumatol. 2015;27(1):63–70.
- 2. Puechal X, et al. Rheumatoid vasculitis: a systematic review of the literature. Autoimmun Rev. 2021;20(5):102800.
- 3. Stone JH, et al. Rituximab versus cyclophosphamide for ANCA-associated vasculitis (RAVE). N Engl J Med. 2010;363(3):221–232.
- 4. Jones RB, et al. Rituximab versus cyclophosphamide in ANCA-associated renal vasculitis (RITUXVAS). N Engl J Med. 2010;363(3):211–220.
- 5. Bartels CM, et al. Rheumatoid vasculitis: declining incidence in the biologic era. J Rheumatol. 2019;46(6):576–583.
- 6. Sayarlioglu M. Rheumatoid nodules and rheumatoid vasculitis. Turk J Rheumatol. 2014;29(2):121–128.
- 7. Australian Institute of Health and Welfare (AIHW). Rheumatoid arthritis in Aboriginal and Torres Strait Islander peoples. Cat. no. PHE 257. Canberra: AIHW; 2021.
- 8. The Royal Australian College of General Practitioners (RACGP). Smoking, health and Australian policy. East Melbourne: RACGP; 2023.
- 9. National Health and Medical Research Council (NHMRC). Australian guidelines for the clinical care of people with rheumatoid arthritis. Canberra: NHMRC; 2018.
- 10. Chung SA, et al. 2021 American College of Rheumatology/Vasculitis Foundation guideline for the management of polyarteritis nodosa. Arthritis Care Res. 2021;73(8):1061–1070.
- 11. RHDAustralia. Australian rheumatic fever and rheumatic heart disease guidelines. 3rd ed. Darwin: Menzies School of Health Research; 2020.
- 12. Mocanu M, et al. Mononeuritis multiplex in rheumatoid vasculitis: outcomes with rituximab therapy. J Clin Rheumatol. 2020;26(4):148–153.
- 13. Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook. Australian Government Department of Health; 2024.
- 14. Medical Benefits Schedule (MBS) Online. Australian Government Department of Health. Available at: www.mbsonline.gov.au. Accessed 2024.