📋 Key Information Summary
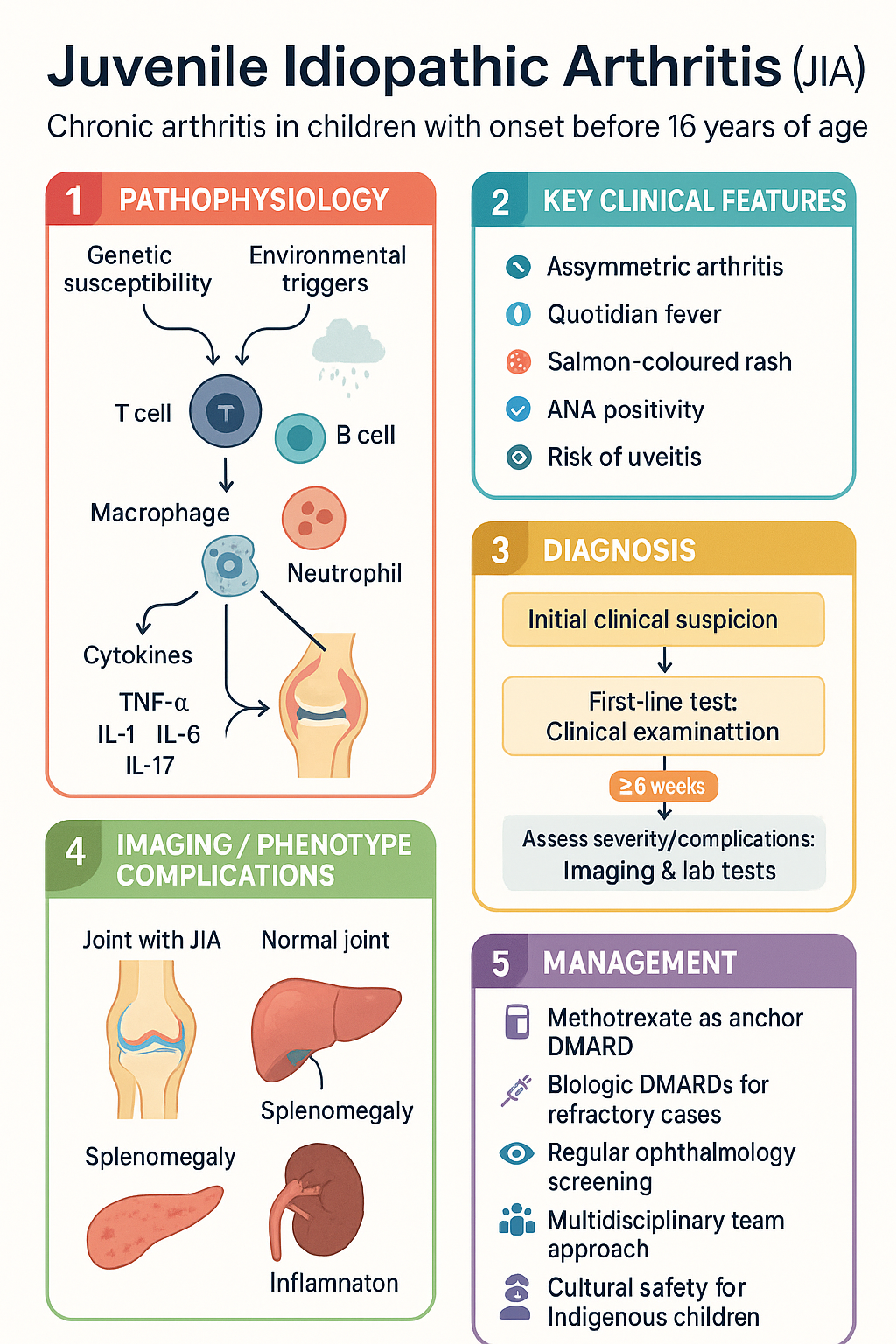
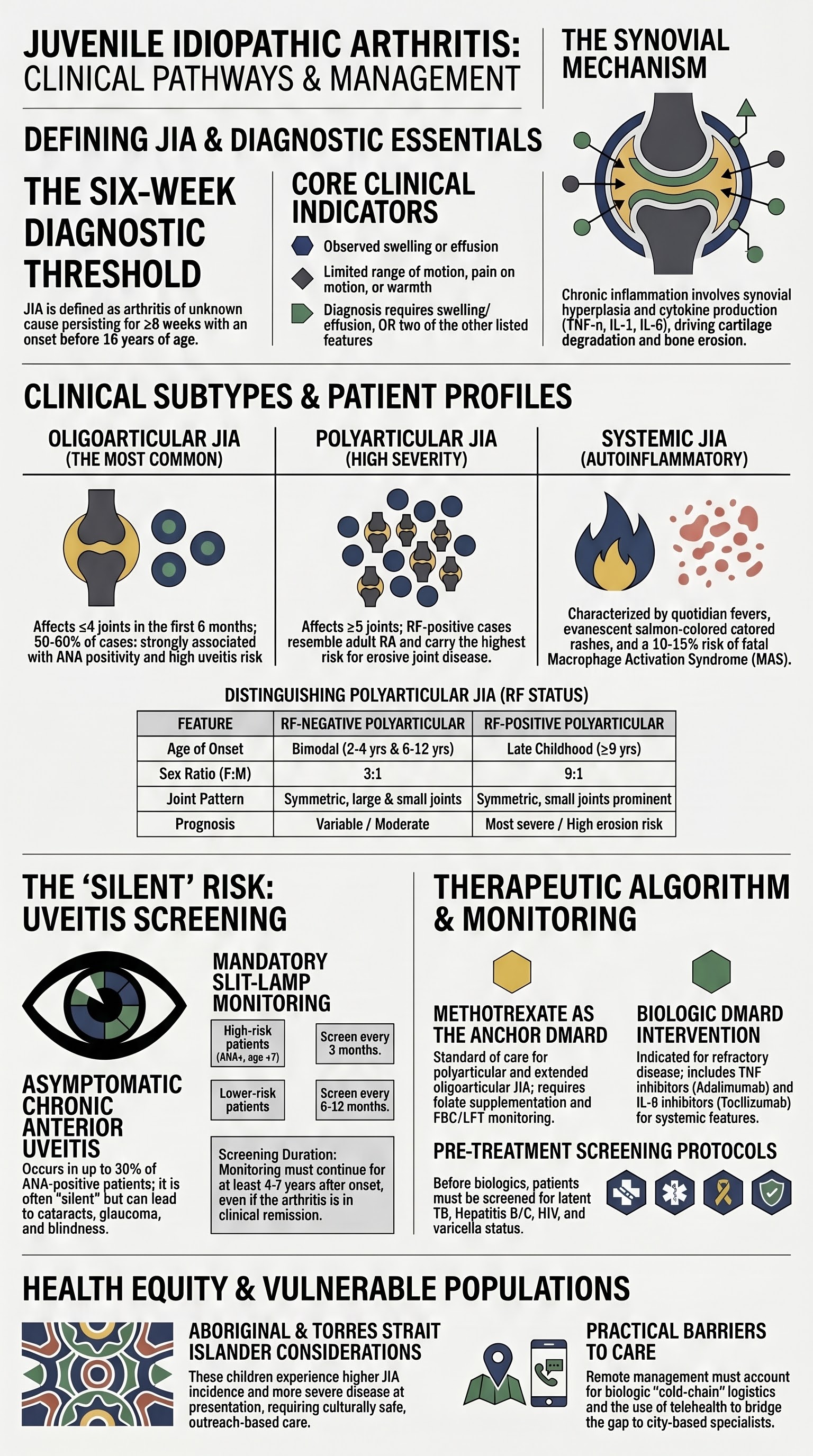
- Juvenile Idiopathic Arthritis (JIA) is the most common chronic rheumatic disease in children, defined as arthritis of unknown cause persisting for ≥6 weeks with onset before 16 years of age.
- Classification follows the International League of Associations for Rheumatology (ILAR) criteria, subdivided into oligoarticular, polyarticular, systemic, enthesitis-related, psoriatic, and undifferentiated arthritis.
- Oligoarticular JIA (≤4 joints in first 6 months) is the most common subtype, strongly associated with ANA positivity and risk of asymptomatic chronic anterior uveitis.
- All children with JIA require baseline and regular screening ophthalmology examinations for uveitis, as it is often silent and can lead to blindness.
- Systemic JIA presents with quotidian fever, evanescent salmon-coloured rash, serositis, hepatosplenomegaly, and lymphadenopathy; it carries a risk of life-threatening macrophage activation syndrome (MAS).
- Methotrexate is the anchor disease-modifying anti-rheumatic drug (DMARD) for polyarticular, extended oligoarticular, and systemic JIA with active arthritis.
- Biologic DMARDs, particularly TNF inhibitors (adalimumab, etanercept) and IL-6 inhibitors (tocilizumab), are indicated for refractory disease or specific subtypes.
- Early, aggressive treatment aiming for remission or minimal disease activity is crucial to prevent joint damage, growth disturbance, and disability.
- Management requires a multidisciplinary team including paediatric rheumatology, ophthalmology, physiotherapy, occupational therapy, and psychology.
- Aboriginal and Torres Strait Islander children experience a higher burden of JIA, often with delayed diagnosis and greater disease severity, necessitating culturally safe care and outreach services.
Introduction & Australian Epidemiology
Juvenile Idiopathic Arthritis (JIA) is a heterogeneous group of disorders characterised by chronic arthritis of at least six weeks' duration with onset before the age of 16 years, after other causes have been excluded. It is the most common chronic rheumatic condition of childhood and a significant cause of disability and morbidity.
In Australia, the incidence is estimated at 2-4 per 100,000 children per year, with a point prevalence of approximately 1 in 1,000. There is considerable variation in subtype distribution, with oligoarticular JIA being the most common overall. Data suggests Aboriginal and Torres Strait Islander children may have a higher incidence and present with more severe disease.
The disease has a significant impact on quality of life, affecting physical function, school attendance, and family dynamics. Early diagnosis and initiation of appropriate therapy by a paediatric rheumatologist is paramount to achieving optimal long-term outcomes.
Pathophysiology
JIA is an autoimmune/autoinflammatory disorder driven by a complex interplay of genetic susceptibility and environmental triggers. The precise aetiology is unknown, but key mechanisms involve dysregulation of the adaptive and innate immune systems.
There is a strong association with specific HLA alleles (e.g., HLA-DR5 in oligoarticular JIA, HLA-B27 in enthesitis-related arthritis). Environmental factors such as infections may trigger disease in genetically predisposed individuals through molecular mimicry or bystander activation.
The synovial membrane in JIA shows features of chronic inflammation with infiltration of T cells, B cells, macrophages, and neutrophils. This leads to hyperplasia of the synovial lining, neovascularisation, and production of pro-inflammatory cytokines (e.g., TNF-α, IL-1, IL-6, IL-17). These cytokines drive cartilage degradation, bone erosion, and the systemic features of fever and growth disturbance.
Systemic JIA has a distinct autoinflammatory pathophysiology, with a prominent innate immune dysregulation and overproduction of IL-1β and IL-6, explaining its unique clinical features and response to specific cytokine blockade.
Oligoarticular JIA
Oligoarticular JIA is defined as arthritis affecting four or fewer joints during the first six months of disease. It accounts for approximately 50-60% of all JIA cases in Australia and predominantly affects young girls (peak onset 2-4 years).
Subtypes
- Persistent oligoarticular: Arthritis remains in ≤4 joints throughout the disease course.
- Extended oligoarticular: After the initial 6 months, arthritis extends to affect >4 joints. This occurs in up to 50% of patients initially presenting with oligoarticular disease.
Key Features
- Asymmetric arthritis, commonly affecting large joints (knees, ankles, wrists).
- High prevalence of antinuclear antibody (ANA) positivity (60-80%).
- Significant risk of chronic anterior uveitis (up to 20%), especially in young, ANA-positive girls.
- Often presents with a painless limp or joint swelling; may have leg length discrepancy due to growth disturbance.
Polyarticular JIA
Polyarticular JIA is defined as arthritis affecting five or more joints within the first six months of disease. It accounts for 20-30% of JIA cases. It is further subdivided by rheumatoid factor (RF) status.
Subtypes
| Feature | RF-negative Polyarticular JIA | RF-positive Polyarticular JIA |
|---|---|---|
| Age of onset | Bimodal (2-4 yrs and 6-12 yrs) | Late childhood/adolescence (≥9 yrs) |
| Sex ratio (F:M) | 3:1 | 9:1 |
| Joint pattern | Symmetric, small & large joints | Symmetric, small joints (hands/feet) prominent, erosive |
| Prognosis | Variable, often moderate | Most severe, high risk of erosive disease and disability |
| ANA positivity | 40-50% | Less common |
Clinical Presentation
Children present with pain, stiffness, and swelling in multiple joints. Morning stiffness is prominent. Systemic features like low-grade fever and fatigue may be present but are not dominant. RF-positive polyarticular JIA clinically resembles adult rheumatoid arthritis and has the worst functional prognosis among JIA subtypes.
Systemic JIA & Macrophage Activation Syndrome
Systemic JIA (sJIA) accounts for 10-20% of JIA cases and is distinguished by prominent systemic inflammation. It has a biphasic age distribution (1-5 years and late childhood).
Diagnostic Features (Requires arthritis + ≥1 major criterion)
MAS Diagnosis & Management
Triggers: Flare of sJIA, intercurrent infection, or change in medication.
Clinical/Lab Features (2016 MAS/sJIA criteria): Fever, hepatomegaly, falling ESR (due to fibrinogen consumption), hypofibrinogenaemia (<2.5 g/L), elevated AST, falling platelet count (<181 × 10⁹/L), elevated ferritin (>684 ng/mL), elevated LDH.
Immediate Management:
- High-dose corticosteroids: IV methylprednisone 30 mg/kg (max 1 g) daily for 3 days.
- Ciclosporin: 2-5 mg/kg/day in divided doses (TDS-QID). PBS Authority Required for this indication.
- Anakinra (IL-1 receptor antagonist): 2-10 mg/kg/day SC. Often used as first-line if MAS is diagnosed early. PBS Authority Required.
- Supportive ICU care for haemodynamic instability, coagulopathy, and cytopenias.
Enthesitis-Related Arthritis (ERA)
ERA is part of the juvenile spondyloarthropathy spectrum. It is defined by the presence of both arthritis and enthesitis, or arthritis OR enthesitis with at least two of: sacroiliac joint tenderness, inflammatory spinal pain, HLA-B27 positivity, family history of HLA-B27-associated disease, anterior uveitis (often acute), or onset in a male ≥6 years old.
Key Features
- Predominantly affects males (8:1 ratio).
- Enthesitis (pain at tendon/ligament insertions) is a hallmark, commonly at Achilles tendon, patellar insertion, plantar fascia, and tibial tuberosity.
- Arthritis is often asymmetric, affecting large joints of the lower limbs (knees, ankles).
- Sacroiliitis and spondylitis may develop later in the disease course.
- Acute anterior uveitis (symptomatic, unilateral) is associated, contrasting with the chronic asymptomatic uveitis in oligoarticular JIA.
Treatment involves NSAIDs for symptomatic relief, physiotherapy, and early introduction of DMARDs (sulfasalazine, methotrexate) for peripheral arthritis. TNF inhibitors are highly effective for refractory disease and axial involvement.
Uveitis Screening
Chronic anterior uveitis (CAU) is a serious extra-articular manifestation of JIA, occurring in 15-20% of patients overall, but up to 30% in ANA-positive oligoarticular JIA. It is typically asymptomatic, insidious in onset, and can lead to sight-threatening complications (cataracts, glaucoma, band keratopathy, visual loss) if not detected and treated early.
| JIA Subtype & Risk Factors | Screening Frequency |
|---|---|
| Oligoarticular, Polyarticular, Psoriatic JIA + ANA + Age <7 yrs at onset | Every 3 months |
| Oligoarticular, Polyarticular, Psoriatic JIA + ANA + Age ≥7 yrs at onset | Every 6 months |
| Systemic JIA (without ANA or other risk factors) | Every 12 months |
| Enthesitis-Related Arthritis | Every 6 months (for acute anterior uveitis) |
Screening Duration: Continue for at least 4-7 years after disease onset, even if arthritis is in remission. Many recommend lifelong screening due to late-onset uveitis.
Treatment: Topical corticosteroids are first-line for active uveitis. Methotrexate is the most common steroid-sparing agent. TNF inhibitors, particularly adalimumab (PBS-listed for this indication), are second-line for refractory uveitis.
Methotrexate & Biologics in Children
Early, aggressive treatment with disease-modifying anti-rheumatic drugs (DMARDs) is the standard of care for JIA to control inflammation, prevent joint damage, and preserve growth and function.
Anchor DMARD: Methotrexate
Biologic DMARDs
Indicated for patients with inadequate response or intolerance to methotrexate. Selection is guided by JIA subtype, dominant clinical features (e.g., uveitis, systemic features), and PBS criteria.
| Agent (Class) | Typical Indication in JIA | Paediatric Dose (example) | PBS Status |
|---|---|---|---|
| Etanercept (TNFi) | Polyarticular, extended oligoarticular, ERA | 0.8 mg/kg (max 50 mg) SC once weekly | Authority Required |
| Adalimumab (TNFi) | Polyarticular, ERA, refractory uveitis | 20-40 mg SC every 2 weeks (weight-based) | Authority Required |
| Tocilizumab (IL-6Ri) | Systemic JIA (with systemic features), polyarticular | 8-12 mg/kg IV monthly OR 4-16 mg/kg SC weekly | Authority Required |
| Anakinra (IL-1Ri) | Systemic JIA (especially with MAS risk) | 1-2 mg/kg (max 100 mg) SC daily | Authority Required |
| Abatacept (T-cell co-stim. modulator) | Polyarticular JIA (refractory) | 10 mg/kg (max 125 mg) IV at 0,2,4 wks then monthly OR weight-based SC weekly | Authority Required |
Clinical Presentation & Diagnostic Criteria
Diagnosis of JIA is clinical and requires exclusion of other causes (infectious, reactive, post-streptococcal, malignancy, other rheumatic diseases). The ILAR classification criteria (2001 revision) are used.
Core Diagnostic Criteria
- Age of onset <16 years.
- Arthritis (swelling OR effusion OR two of: limitation of range of motion, tenderness/pain on motion, warmth) in one or more joints.
- Duration of disease ≥6 weeks.
- Exclusion of other known causes of arthritis.
A thorough history and examination should document pattern of joint involvement, systemic symptoms, family history, and risk factors for uveitis. Baseline investigations are essential to rule out differential diagnoses.
Investigations
Investigations are used to support diagnosis, exclude differential diagnoses, assess disease activity, and monitor for drug toxicity.
Note: Australian MBS item numbers are indicative and subject to change. Always verify current item numbers and rebate eligibility.
Risk Stratification & Severity Scoring
Risk stratification guides treatment intensity and prognostication. There is no single universal score, but factors influencing poor prognosis are well-recognised.
Poor Prognostic Factors
- Hip, wrist, or cervical spine arthritis.
- Polyarticular course or RF positivity.
- Persistently elevated inflammatory markers (ESR/CRP).
- Radiographic damage (erosions, joint space narrowing).
- Systemic features (fever, rash) in sJIA.
Empirical & First-Line Therapy
Treatment is not truly "empirical" as diagnosis is confirmed first. The initial pharmacological strategy aims to rapidly control inflammation.
Directed / Mechanism-Specific Therapy
For patients with inadequate response to methotrexate or high-risk disease at presentation, biologic DMARDs targeting specific cytokines are indicated.
Therapeutic Algorithm by Subtype
Monitoring
Regular, structured monitoring is essential to assess disease activity, detect complications, and monitor drug toxicity.
Disease Activity Monitoring
- Clinical assessment: Joint counts (active, limited), patient/parent global assessment, functional assessment (CHAQ).
- Laboratory: ESR, CRP, FBC (for MAS monitoring in sJIA).
- Goal: Achieve clinical remission on medication (ACR JIA criteria).
Drug Safety Monitoring
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Petty RE, et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31(2):390-2.
- 2. Australian Institute of Health and Welfare (AIHW). Rheumatoid arthritis and other musculoskeletal conditions. AIHW, Canberra. 2023.
- 3. Ravelli A, et al. 2016 Classification Criteria for Macrophage Activation Syndrome Complicating Systemic Juvenile Idiopathic Arthritis. Arthritis Rheumatol. 2016;68(3):566-76.
- 4. Heiligenhaus A, et al. Evidence-based, interdisciplinary guidelines for anti-inflammatory treatment of uveitis associated with juvenile idiopathic arthritis. Rheumatol Int. 2012;32(5):1121-33.
- 5. Ringold S, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Treatment of Juvenile Idiopathic Arthritis. Arthritis Rheumatol. 2019;71(5):703-16.
- 6. Ruperto N, et al. A randomized trial of parenteral methotrexate comparing an intermediate dose with a higher dose in children with juvenile idiopathic arthritis who failed to respond to standard doses. Arthritis Rheum. 2010;62(7):2103-12.
- 7. Pharmaceutical Benefits Scheme (PBS). Australian Government Department of Health. Available from: www.pbs.gov.au. [Accessed 2024].
- 8. Royal Australasian College of Physicians (RACP). Paiatric palliative care: a guide for health professionals. 2022.
- 9. South Australian Department of Health. Model of Care for Paediatric Rheumatology. 2021.
- 10. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. 2021.
- 11. Beukelman T, et al. 2011 American College of Rheumatology recommendations for the treatment of juvenile idiopathic arthritis. Arthritis Care Res (Hoboken). 2011;63(4):465-82.