📋 Key Information Summary
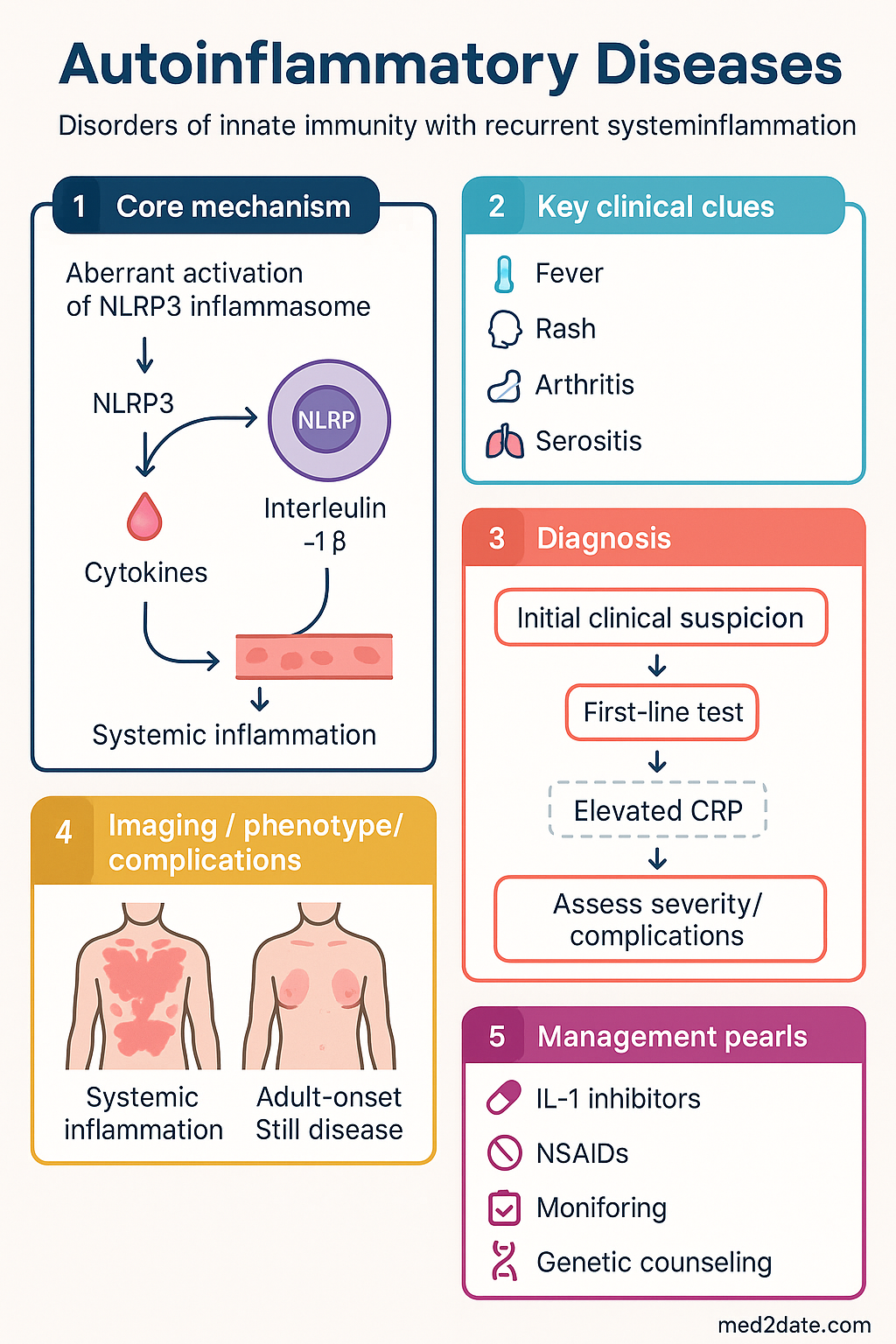
- Autoinflammatory diseases are disorders of innate immunity with recurrent, unprovoked systemic inflammation; they lack pathogenic autoantibodies or autoreactive T-cells.
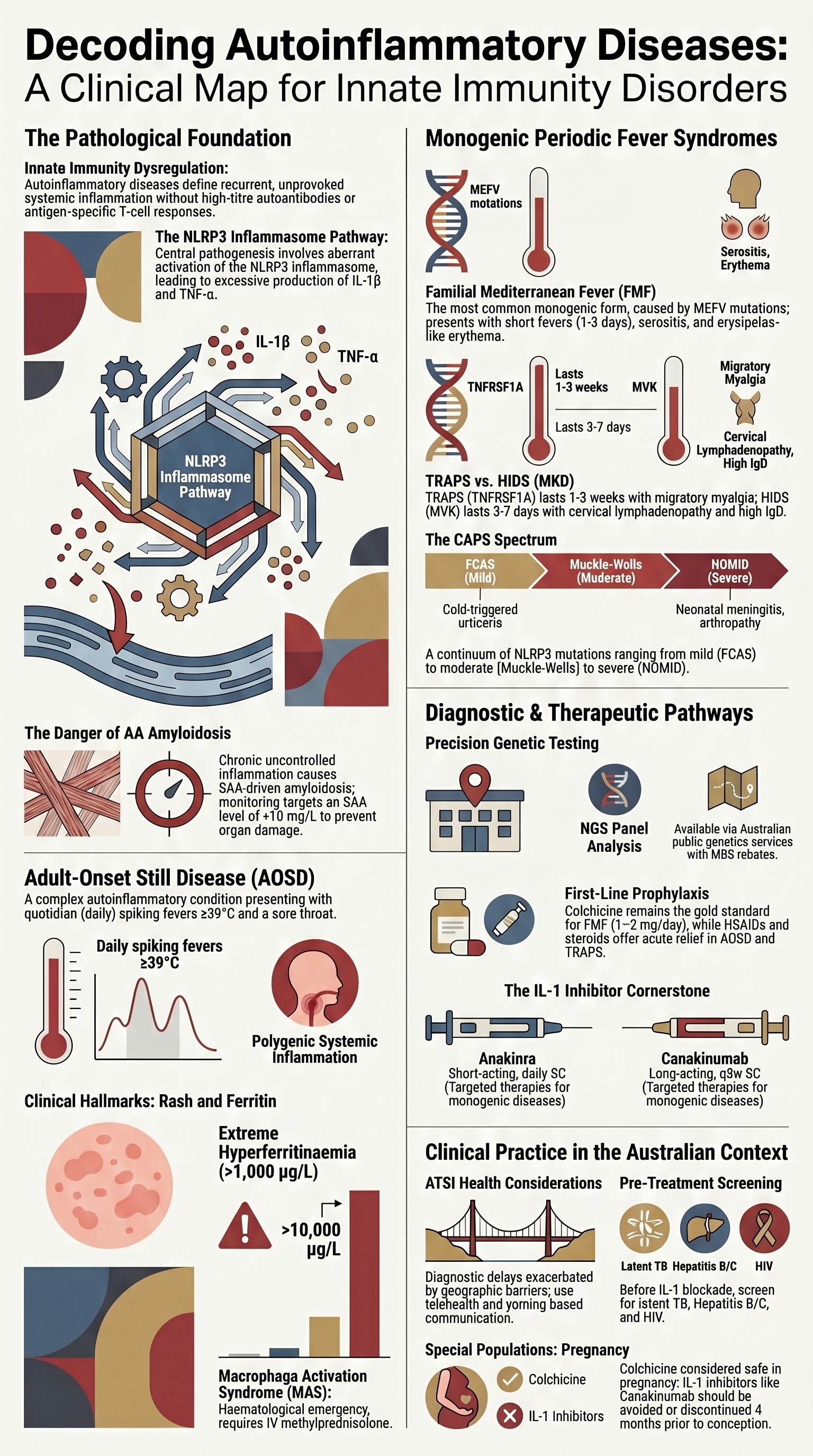
- Familial Mediterranean fever (FMF) is the most common monogenic autoinflammatory disease; treat with colchicine as first-line prophylaxis.
- Cryopyrin-associated periodic syndromes (CAPS) — comprising FCAS, MWS, NOMID — respond dramatically to IL-1 blockade.
- TRAPS (TNF-receptor–associated periodic syndrome) and HIDS (hyper-IgD syndrome / mevalonate kinase deficiency) should be considered in undifferentiated recurrent fever.
- Adult-onset Still disease (AOSD) presents with quotidian spiking fevers, evanescent salmon rash, and marked hyperferritinaemia.
- IL-1 inhibitors (anakinra, canakinumab, rilonacept) are the cornerstone therapy for most monogenic autoinflammatory diseases.
- Genetic testing via next-generation sequencing panels is now available through Australian public genetics services (MBS rebate applicable).
- Serum amyloid A (SAA)-driven AA amyloidosis is the most feared long-term complication of uncontrolled autoinflammation.
- Inflammasomopathies — including PAPA, DADA2, DIRA, HA20 — are NLRP3/inflammasome-mediated entities with IL-1 or TNF-α responsiveness.
- Special populations — pregnancy, paediatrics, renal impairment — require tailored dosing and monitoring of IL-1 inhibitors.
- Aboriginal and Torres Strait Islander peoples may face delayed diagnosis due to geographic and systemic barriers; ensure culturally safe referral pathways.
Introduction & Australian Epidemiology
Autoinflammatory diseases are rare disorders characterised by dysregulation of the innate immune system, leading to sterile, recurrent episodes of inflammation. Unlike autoimmune conditions, they lack high-titre autoantibodies or antigen-specific T-cell responses. Central pathogenic mechanisms involve aberrant activation of the NLRP3 inflammasome, excessive IL-1β, TNF-α, or other innate cytokine production.
In Australia, monogenic autoinflammatory diseases are estimated to affect 1–3 per 100,000 population, though FMF prevalence is higher in communities with Mediterranean or Middle Eastern ancestry. Adult-onset Still disease is more common, with an estimated incidence of 0.16 per 100,000 per year. Significant diagnostic delay (mean 5–10 years for monogenic conditions) remains a key challenge in the Australian setting.
Management centres on achieving sustained inflammatory control to prevent AA amyloidosis, leveraging IL-1 and targeted cytokine inhibition. Australian specialists should coordinate through multidisciplinary teams involving rheumatology, immunology, genetic medicine, and nephrology.
Familial Mediterranean Fever (FMF)
Overview
FMF is an autosomal-recessive disorder caused by pathogenic variants in MEFV (chromosome 16p13.3) encoding pyrin. It is the most common monogenic autoinflammatory disease worldwide, particularly prevalent in Mediterranean, Middle Eastern, and Armenian populations. In Australia, FMF is seen in individuals of Lebanese, Turkish, Armenian, Jewish, and Arab descent.
Clinical Features
- Recurrent, self-limiting febrile episodes (1–3 days), typically with serositis (peritonitis, pleuritis, pericarditis)
- Erysipelas-like erythema over the lower limbs
- Acute monoarthritis (large joints)
- In children: episodes may be shorter and more frequent; scrotal oedema is a recognised feature
- AA amyloidosis is the major long-term complication — 60–70% risk without prophylaxis
Diagnosis
Clinical diagnosis supported by Tel-Hashomer criteria; genetic confirmation with MEFV genotyping (MBS-rebated). Common Australian-pathogenic variants: M694V, V726A, M680I. Compound heterozygotes may present with milder phenotype.
Treatment
Cryopyrin-Associated Periodic Syndromes (CAPS)
Spectrum
CAPS are autosomal-dominant gain-of-function variants in NLRP3 (CIAS1), leading to constitutive inflammasome activation and IL-1β overproduction. Three severity phenotypes exist on a continuum:
Treatment
- Canakinumab (Ilaris®) 150 mg SC every 8 weeks for MWS/FCAS; 2–4 mg/kg (max 300 mg) every 4–8 weeks for NOMID — ⚠ PBS Authority Required
- Anakinra (Kineret®) 1–2 mg/kg/day SC — alternative; ⚠ PBS Authority Required
- IL-1 blockade is lifelong; withdrawal leads to rapid disease flare
- NSAIDs and corticosteroids are ineffective as monotherapy
TRAPS & HIDS
| Feature | TRAPS | HIDS (MKD) |
|---|---|---|
| Gene | TNFRSF1A | MVK |
| Inheritance | Autosomal dominant | Autosomal recessive |
| Episode duration | 1–3 weeks (longer than FMF) | 3–7 days |
| Hallmark features | Migratory myalgia, centrifugal erythematous rash, periorbital oedema | Cervical lymphadenopathy, abdominal pain, elevated IgD (>100 IU/mL) |
| 1st-line Rx | Corticosteroids (acute); NSAIDs | NSAIDs, corticosteroids (limited efficacy) |
| Targeted therapy | Etanercept or IL-1 inhibitor | Anakinra (acute/rescue) or canakinumab (prophylaxis) |
| PBS access | ⚠ Authority Required | ⚠ Authority Required |
Adult-Onset Still Disease (AOSD)
Clinical Presentation
AOSD is a polygenic autoinflammatory condition with characteristic features:
- Quotidian (daily) spiking fevers ≥39°C, often with a single daily spike ("double quotidian" pattern in ~20%)
- Evanescent salmon-pink macular rash (trunk/proximal limbs, coincides with fever)
- Arthritis (wrists, knees, ankles); chronic in ~50%
- Sore throat (pharyngitis) — a classic early symptom
- Lymphadenopathy, hepatosplenomegaly, serositis
- Markedly elevated ferritin (often >1,000 µg/L; >10,000 µg/L raises macrophage activation syndrome concern)
Diagnostic Criteria (Yamaguchi, modified)
Requires ≥5 criteria (including ≥2 major), after excluding infection, malignancy, and other rheumatic diseases.
| Major Criteria | Minor Criteria |
|---|---|
| Fever ≥39°C, intermittent, ≥1 week | Sore throat |
| Arthralgia ≥2 weeks | Lymphadenopathy |
| Typical rash (salmon, evanescent) | Hepatomegaly or splenomegaly |
| Leukocytosis ≥10×10⁹/L (≥80% neutrophils) | Abnormal liver function tests |
| Negative RF and ANA |
Treatment Ladder
- 1st-line: NSAIDs (indomethacin 50 mg TDS PO) — symptom control
- 2nd-line: Corticosteroids (prednisolone 0.5–1 mg/kg/day PO, taper over weeks)
- Steroid-sparing / refractory: Methotrexate 10–25 mg/week PO/SC — ✔ PBS General Benefit
- IL-1 blockade (biologic-refractory): Anakinra 100 mg SC daily or canakinumab 150 mg SC q8w — ⚠ PBS Authority Required
- Refractory: Tocilizumab 8 mg/kg IV q4w (limited data); cyclosporin A as rescue
Inflammasomopathies & IL-1 Inhibitors
Inflammasome-Mediated Diseases
| Syndrome | Gene / Pathway | Key Features | Preferred Agent |
|---|---|---|---|
| PAPA | PSTPIP1 | Pyogenic arthritis, pyoderma gangrenosum, acne | Anakinra or IL-6 inhibitor |
| DADA2 | CECR1 (ADA2) | Livedo, early-onset lacunar strokes, vasculitis, immunodeficiency | Anti-TNF (etanercept/adalimumab) |
| DIRA | IL1RN | Neonatal-onset sterile multifocal osteomyelitis, periostitis, pustulosis | Anakinra (replaces endogenous IL-1Ra) |
| HA20 | OTULIN | Early-onset Behçet-like disease; oral/genital ulcers, fever | Anakinra or anti-TNF |
IL-1 Inhibitors — Comparison
Genetic Testing
Genetic confirmation is increasingly essential for precision therapy. Australian resources:
Practical Guidance
- Discuss genetic testing with a clinical geneticist or genetic counsellor pre-test
- Genetic results require phenotypic correlation — variants of uncertain significance (VUS) are common
- Inform Medicare genetics referral (GP referral → specialist → genetics service)
- Presymptomatic testing in at-risk family members for autosomal-dominant conditions (TRAPS, CAPS) should follow NHRMC guidelines
- Store DNA samples for future re-analysis as gene panels expand
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Federici S, Sormani MP, Ozen S, et al. Evidence-based provisional clinical classification criteria for autoinflammatory periodic fevers. Ann Rheum Dis. 2015;74(5):799–805.
- 2. Shinar Y, Obici L, Aksentijevich I, et al. Guidelines for the genetic diagnosis of hereditary recurrent fevers. Ann Rheum Dis. 2012;71(10):1599–1605.
- 3. Ozen S, Bilginer Y. A clinical guide to autoinflammatory diseases: familial Mediterranean fever and next-of-kin. Nat Rev Rheumatol. 2014;10(3):135–147.
- 4. Kuemmerle-Deschner JB, Ozen S, Tyrrell PN, et al. Diagnostic criteria for cryopyrin-associated periodic syndrome (CAPS). Ann Rheum Dis. 2017;76(6):942–947.
- 5. Lachmann HJ, Kone-Paut I, Kuemmerle-Deschner JB, et al. Use of canakinumab in the cryopyrin-associated periodic syndrome. N Engl J Med. 2009;360(23):2416–2425.
- 6. Lachmann HJ, Papa R, Gerhold K, et al. The phenotype of TNF receptor-associated autoinflammatory syndrome (TRAPS) in 83 patients. Medicine (Baltimore). 2014;93(17):258–267.
- 7. van der Hilst JCH, Bodar EJ, Barron KS, et al. Long-term follow-up, clinical features, and quality of life in a series of 103 patients with hyperimmunoglobulinemia D syndrome. Medicine (Baltimore). 2008;87(6):301–310.
- 8. Gerfaud-Valentin M, Jamilloux Y, Iwaz J, Sève P. Adult-onset Still's disease. Autoimmun Rev. 2014;13(7):708–722.
- 9. Navon Elkan P, Pierce SB, Segel R, et al. Mutant adenosine deaminase 2 in a polyarteritis nodosa vasculopathy. N Engl J Med. 2014;370(10):921–931.
- 10. Aksentijevich I, Masters SL, Ferguson PJ, et al. An autoinflammatory disease with deficiency of the interleukin-1-receptor antagonist. N Engl J Med. 2009;360(23):2426–2437.
- 11. Ruperto N, Brunner HI, Quartier P, et al. Two randomized trials of canakinumab in systemic juvenile idiopathic arthritis. N Engl J Med. 2012;367(25):2396–2406.
- 12. Australian Government Department of Health. Pharmaceutical Benefits Scheme — Anakinra (Kineret) Authority Required listing. PBS Online. Updated 2024. Available at: pbs.gov.au.
- 13. Australian Indigenous HealthInfoNet. Overview of Aboriginal and Torres Strait Islander health status 2023. Perth: AIHW/HealthInfoNet; 2024.
- 14. RACGP. Red Book: Immunisation and infectious diseases — screening for latent TB before biologic therapy. 10th edition. Melbourne: RACGP; 2023.