📋 Key Information Summary
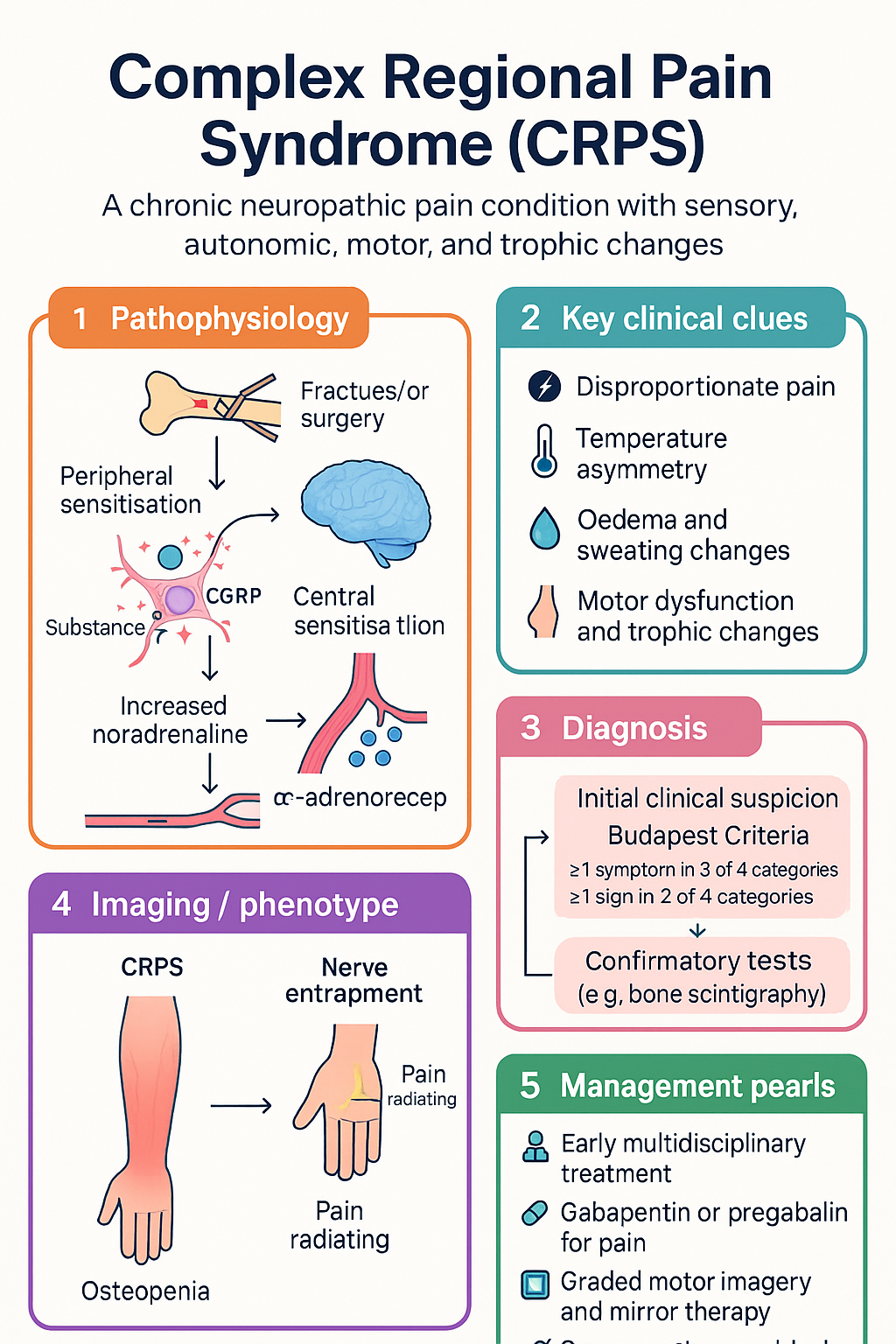
- Complex Regional Pain Syndrome (CRPS) is a chronic neuropathic pain condition characterised by disproportionate pain, sensory, autonomic, motor, and trophic changes — usually affecting a single limb.
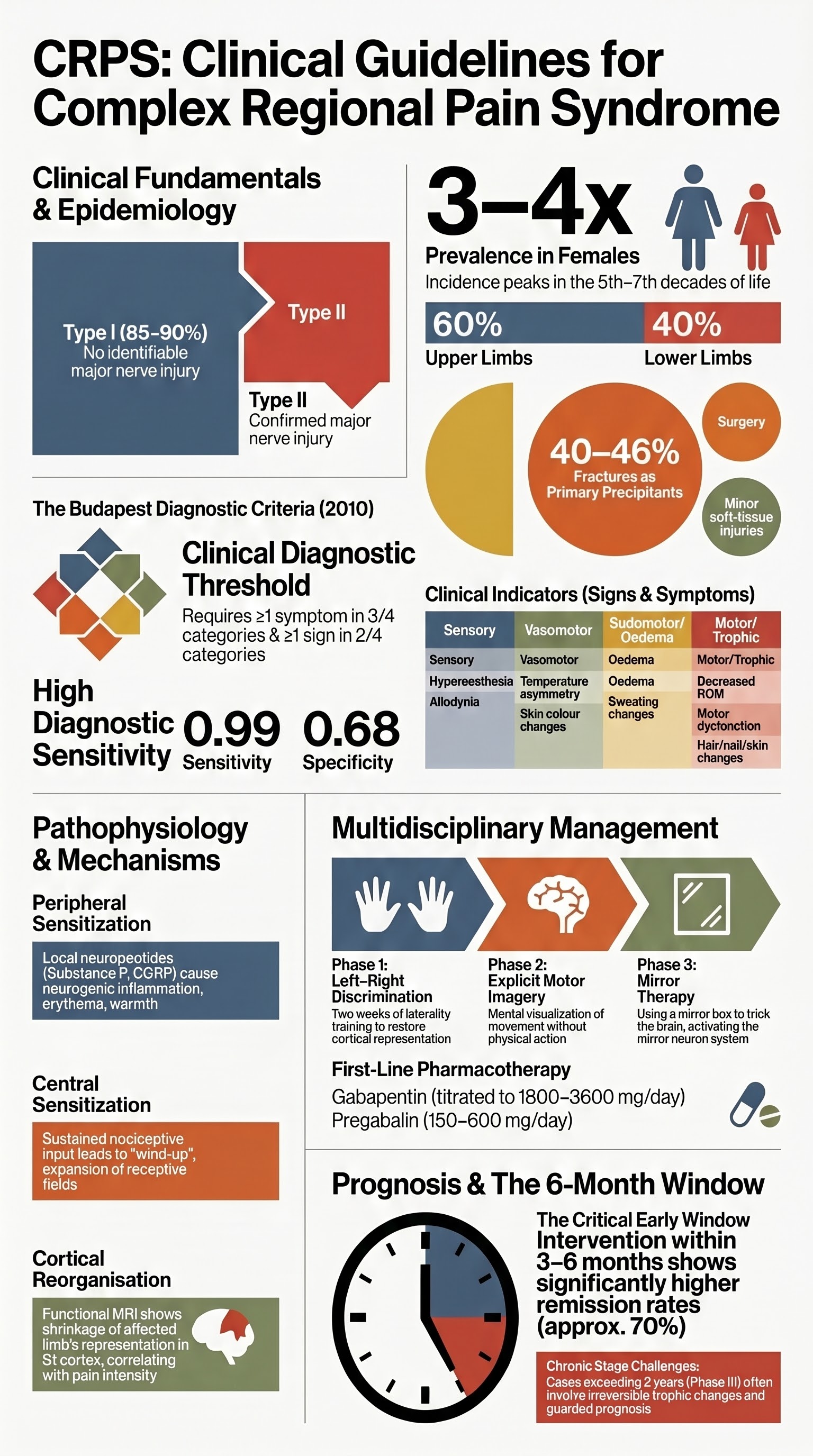
- CRPS Type I (formerly reflex sympathetic dystrophy) occurs without identifiable major nerve injury; CRPS Type II (formerly causalgia) follows a defined nerve injury.
- Diagnosis is clinical using the Budapest Criteria (2010), which require ≥1 symptom in 3 of 4 categories and ≥1 sign in 2 of 4 categories, with no better diagnosis to explain findings.
- Early diagnosis and commencement of multidisciplinary treatment within the first 3–6 months is associated with significantly better outcomes and reduced risk of chronicity.
- Graded motor imagery and mirror therapy are the most evidence-based physiotherapy interventions and should be initiated as first-line rehabilitation.
- Sympathetic dysfunction is variably present — CRPS may be sympathetically maintained (SMP) or sympathetically independent (SIP), and this distinction guides interventional management.
- First-line pharmacotherapy: gabapentin (titrate to 1800–3600 mg/day) or pregabalin (150–600 mg/day) — both PBS-listed for neuropathic pain.
- Second-line agents include oral bisphosphonates (alendronate or neridronate — neridronate not yet PBS-listed for CRPS), low-dose IV ketamine infusions (specialist-administered), and tricyclic antidepressants (amitriptyline).
- Interventional options for refractory cases: sympathetic nerve blocks, spinal cord stimulation, and intrathecal drug delivery — managed by pain medicine specialists.
- Aboriginal and Torres Strait Islander peoples face significant barriers to early CRPS diagnosis and access to multidisciplinary pain services; culturally safe care and telehealth pain programmes are essential.
- Prognosis is variable: ~70% of early-stage CRPS (Type I) achieves significant improvement or remission within 12–18 months with appropriate treatment; chronic CRPS (>2 years) has a more guarded prognosis.
- MBS item 110 (GP Management Plan) and item 81300 (Pain Medicine Physician attendance) support chronic pain care coordination in the Australian healthcare system.
Introduction & Australian Epidemiology
Complex Regional Pain Syndrome (CRPS) is a chronic neuropathic pain condition that typically affects a single extremity and is characterised by a constellation of sensory, autonomic, motor, and trophic disturbances that are disproportionate to the inciting event. The condition was historically divided into reflex sympathetic dystrophy (CRPS Type I) and causalgia (CRPS Type II).
In Australia, CRPS has an estimated incidence of 5.46–26.2 per 100,000 person-years, with the upper limbs affected more commonly than lower limbs (approximately 60:40 ratio). The condition is 3–4 times more common in females and peaks in incidence in the 5th–7th decades of life. Fractures remain the most common precipitant (approximately 40–46% of cases), followed by surgical procedures, sprains, and minor soft-tissue injuries.
The socioeconomic burden of CRPS in Australia is substantial: patients frequently experience loss of work capacity, prolonged opioid dependence, and reduced quality of life. The condition may lead to permanent limb dysfunction if not identified and managed within the critical early window. The Australian Commission on Safety and Quality in Health Care (ACSQHC) recognises chronic pain management as a priority area within the National Safety and Quality Health Service (NSQHS) Standards.
Budapest Diagnostic Criteria
The Budapest Criteria (Harden et al., 2010) are the current international consensus diagnostic criteria for CRPS and should be used in all clinical assessments. They replaced the earlier IASP (1994) criteria, which had high sensitivity (0.98) but poor specificity (0.36).
Budapest Criteria — Required Elements
| Category | Symptoms (patient report) | Signs (clinical examination) |
|---|---|---|
| Sensory | Hyperaesthesia and/or allodynia | Hyperaesthesia and/or allodynia |
| Vasomotor | Temperature asymmetry and/or skin colour changes | Temperature asymmetry and/or skin colour changes |
| Sudomotor / Oedema | Oedema and/or sweating changes | Oedema and/or sweating changes |
| Motor / Trophic | Decreased range of motion and/or motor dysfunction (weakness, tremor, dystonia) and/or trophic changes (hair, nail, skin) | Decreased range of motion and/or motor dysfunction and/or trophic changes |
Diagnostic threshold: The patient must report at least one symptom in 3 of the 4 categories, and the clinician must identify at least one sign in 2 of the 4 categories. There must be no other diagnosis that better explains the signs and symptoms.
Specifiers (Modifier Descriptors)
Following a clinical diagnosis of CRPS, the following specifiers may be appended:
- "with predominant sympathetically maintained pain" — if sympatholytic therapy (e.g., sympathetic nerve block) produces significant pain relief.
- "without sympathetically maintained pain" — if sympathetic blockade does not produce relief (sympathetically independent pain).
- "without continuing identifiable peripheral nociceptive input" — when no ongoing peripheral driver can be identified.
- "with continuing identifiable peripheral nociceptive input" — when an ongoing peripheral driver is present (e.g., non-union fracture).
Type I vs Type II CRPS
The distinction between CRPS Type I and Type II is based on the presence or absence of a definable nerve injury. Both types share the same diagnostic criteria and clinical features; the distinction primarily guides investigation and prognosis.
| Feature | CRPS Type I | CRPS Type II |
|---|---|---|
| Historical name | Reflex sympathetic dystrophy (RSD) | Causalgia |
| Nerve injury | No identifiable major nerve lesion | Identifiable major nerve injury confirmed on examination or investigation |
| Common precipitants | Fracture, immobilisation, surgery, sprain, minor trauma | Peripheral nerve transection, crush injury, iatrogenic nerve damage, gunshot wound |
| Incidence | More common (≈85–90% of CRPS cases) | Less common (≈10–15%) |
| NCS/EMG findings | Usually normal | Abnormal — axonal loss or demyelination in the affected nerve distribution |
| Pattern | May not respect a single nerve territory; often diffuse | Initially follows the distribution of the injured nerve but may spread |
| Prognosis | Generally more favourable with early treatment | Tends to have a more protracted course |
Pathophysiology
The pathophysiology of CRPS is complex and incompletely understood, involving peripheral and central nervous system mechanisms, neuroinflammation, and cortical reorganisation. Current evidence supports a multifactorial model.
Peripheral Mechanisms
- Peripheral sensitisation: Local release of pro-inflammatory neuropeptides (substance P, CGRP) from nociceptive C-fibres results in neurogenic inflammation — manifesting as oedema, erythema, and warmth.
- Sympathetic–afferent coupling: In sympathetically maintained pain (SMP), noradrenaline released by sympathetic efferents activates α-adrenoreceptors that have been aberrantly expressed on nociceptive afferents.
- Peripheral ischaemia: Vasomotor dysfunction leads to microvascular changes, contributing to trophic changes, skin atrophy, and osteopaenia.
Central Mechanisms
- Central sensitisation: Sustained nociceptive input produces wind-up in the dorsal horn, expansion of receptive fields, and reduced descending inhibitory modulation — leading to allodynia and hyperalgesia beyond the site of injury.
- Cortical reorganisation: Functional MRI studies demonstrate shrinkage of the somatotopic representation of the affected limb in S1 cortex, correlating with pain intensity and reversed by successful treatment (mirror therapy, graded motor imagery).
- Disrupted body schema: Patients frequently exhibit impaired proprioception, reduced left–right discrimination, and motor neglect of the affected limb — a key rationale for graded motor imagery programmes.
Genetic and Autoimmune Considerations
Emerging evidence suggests HLA associations (HLA-DQ8, HLA-B62) and autoantibodies against β2-adrenergic and muscarinic M2 receptors in a subset of CRPS patients, supporting a possible autoimmune phenotype — particularly in chronic, spreading CRPS. This remains an active area of research and does not currently alter standard management.
Sympathetic Dysfunction
Sympathetic nervous system dysfunction is a hallmark of CRPS but is not uniformly present. Understanding the sympathetically maintained (SMP) vs sympathetically independent (SIP) distinction is important for guiding interventional pain management.
Clinical Manifestations of Sympathetic Dysfunction
- Vasomotor: Temperature asymmetry (affected limb cooler in SMP; may be warmer in early neurogenic inflammation), skin colour changes (mottled cyanosis, erythema, or pallor).
- Sudomotor: Ipsilateral hyperhidrosis or, less commonly, hypohydrosis.
- Trophic changes: Brittle nails, altered hair growth (initially increased, later absent), shiny atrophic skin, and subcutaneous fat atrophy.
- Bone changes: Periarticular osteopaenia visible on plain radiograph; regional osteoporosis on DEXA in chronic cases.
Diagnosing SMP vs SIP
The gold standard is the sympathetic ganglion block (stellate ganglion block for upper limb; lumbar sympathetic block for lower limb). A ≥50% reduction in pain intensity post-block indicates sympathetically maintained pain. Thermography may demonstrate temperature asymmetry (affected limb ≤1°C cooler) but is not diagnostic alone.
Clinical Presentation & Diagnostic Criteria
CRPS typically presents within days to weeks of an inciting event (fracture, surgery, immobilisation, minor injury) but may develop insidiously. The clinical course is often divided into three phases, though not all patients follow this pattern:
Red Flags — Consider Alternative Diagnoses
- Absence of an inciting event (diagnose CRPS only with caution)
- Symptoms confined strictly to a single dermatome or peripheral nerve territory without spread — consider nerve entrapment or radiculopathy
- Systemic inflammatory features (fever, weight loss, polyarthralgia) — consider vasculitis, rheumatoid arthritis, or malignancy
- Bilateral symmetrical limb involvement — consider peripheral neuropathy, fibromyalgia
- Significant psychiatric comorbidity with symptom magnification — CRPS is NOT a psychiatric diagnosis, but comorbid anxiety and depression are common and should be managed
Investigations
CRPS remains a clinically diagnosed condition. Investigations are used to exclude alternative diagnoses, quantify bone involvement, and assess for nerve injury (Type II). No single investigation is diagnostic of CRPS.
Multidisciplinary Rehabilitation
Multidisciplinary rehabilitation is the cornerstone of CRPS management and should be initiated as early as possible — ideally within the first 3 months. The NHMRC-endorsed chronic pain framework emphasises a biopsychosocial approach combining physical therapy, psychological support, education, and pharmacotherapy.
Graded Motor Imagery Programme
This is the most evidence-based physiotherapy intervention for CRPS, with Level I evidence from randomised controlled trials (Moseley, 2004; Bowering et al., 2013).
Additional Physiotherapy Components
- Desensitisation: Graded exposure to textures — start with the least provocative (silk, cotton) and progress (wool, denim, velvet). Multiple sessions daily.
- Graded exercise therapy: Progressive loading of the affected limb — aerobic exercise, gentle resistance training, aquatic therapy. Avoid aggressive ROM in acute phase (may worsen pain).
- Stress loading: TENS (transcutaneous electrical nerve stimulation) and scrunch tasks — evidence from Oerlemans et al. (1999) supports combined exercise and stress loading.
- Oedema management: Elevation, compression garments (introduced gradually), manual lymphatic drainage.
- Functional restoration: Occupational therapy focus on ADLs, workplace modification, and graded return to function.
Psychological Support
Pain-related catastrophising, kinesiophobia (fear of movement), anxiety, and depression are common in CRPS and predict poorer outcomes. Evidence supports:
- Cognitive behavioural therapy (CBT): Addresses pain catastrophising, fear-avoidance, and coping strategies. Level I evidence.
- Acceptance and commitment therapy (ACT): Increasingly used in Australian chronic pain programmes.
- Eye movement desensitisation and reprocessing (EMDR): Emerging evidence for trauma-associated CRPS onset.
- Pain neuroscience education: Explaining central sensitisation mechanisms reduces catastrophising and improves engagement with rehabilitation.
Pharmacotherapy
Pharmacotherapy for CRPS should be initiated early and used as an adjunct to — not a substitute for — multidisciplinary rehabilitation. Current evidence supports a stepwise approach. International guidelines (IASP, European Pain Federation) and Australian practice are broadly aligned.
First-Line Agents: Gabapentinoids
Second-Line Agents
Ketamine Infusion Therapy
Opioid Analgesia
Other Agents
- Topical capsaicin 8% patch (Qutenza®): Specialist-applied under local anaesthesia. Repeated application may benefit localised CRPS. PBS Authority Required.
- Topical lidocaine 5% patch: May help localised allodynia. Not PBS-listed for this indication (available as authority for postherpetic neuralgia).
- Clonidine: Oral or transdermal — may benefit sympathetic-mediated symptoms. Not PBS-listed for CRPS.
- Corticosteroids: Short-course oral prednisolone (30–40 mg/day for 2–4 weeks with taper) — may benefit very early CRPS (within 3 months of onset) based on limited evidence. Avoid in chronic CRPS.
Monitoring
Regular structured monitoring is essential to track disease trajectory, medication adverse effects, functional improvement, and psychological wellbeing.
Outcome Measures
| Domain | Tool | Frequency |
|---|---|---|
| Pain intensity | Visual Analogue Scale (VAS) or Numeric Rating Scale (NRS 0–10) | Every visit |
| Functional status | CRPS Severity Score (CSS); Patient-Specific Functional Scale (PSFS) | Monthly initially, then 3-monthly |
| Quality of life | EQ-5D-5L; SF-36 | 3–6 monthly |
| Psychological screening | PHQ-9 (depression); GAD-7 (anxiety); PCS (pain catastrophising scale) | At baseline and 3-monthly |
| Limb volume | Circumferential measurement; water displacement | Monthly initially |
| Range of motion | Goniometry — compare to contralateral limb | Monthly initially |
| Bone density | DEXA of affected limb (MBS item 12306) | 12 monthly if bisphosphonate therapy used |
Medication Monitoring
- Gabapentinoids: FBC, LFTs, renal function at baseline and 3-monthly. Monitor for sedation, dizziness, peripheral oedema, weight gain.
- Amitriptyline: ECG at baseline if >60 years or cardiac risk factors (QTc monitoring). FBC, LFTs annually.
- Alendronate: Renal function (contraindicated eGFR <30). Dental review before initiation (osteonecrosis of jaw risk). DEXA at 12 months.
- Ketamine infusions: LFTs, renal function, FBC at baseline and during infusion. Continuous cardiorespiratory monitoring during inpatient infusion.
- Opioids (if used short-term): Opioid Risk Tool (ORT) screening. Naloxone co-prescribing discussion. Urine drug screening as per RACGP guidelines.
Prognosis
Prognosis in CRPS is heterogeneous and depends on disease duration at presentation, treatment initiation, type (I vs II), and psychosocial factors.
Prognostic Factors
| Factor | Better Prognosis | Worse Prognosis |
|---|---|---|
| Duration at diagnosis | <3 months | >12 months |
| CRPS type | Type I | Type II |
| Precipitant | Fracture, immobilisation | Surgery, unclear aetiology |
| Psychosocial | Low catastrophising, strong social support | High catastrophising, litigation, kinesiophobia |
| Treatment | Early multidisciplinary approach | Late or isolated pharmacotherapy |
| Spread | Localised to one limb | Spreading to contralateral limb or elsewhere |
Expected Outcomes
- CRPS Type I (early, <6 months): Approximately 70% of patients achieve significant improvement or complete remission within 12–18 months with appropriate multidisciplinary treatment.
- CRPS Type I (chronic, >2 years): Approximately 30–40% continue to experience significant pain and disability at 5 years.
- CRPS Type II: More protracted course; recovery of nerve function and pain resolution are less likely but still achievable with combined rehabilitation and interventional management.
- Spread: Occurs in approximately 7–24% of patients — most commonly to the contralateral limb. Spread is associated with longer disease duration and higher pain intensity.
- Recurrence: Re-injury or re-immobilisation of the previously affected limb may trigger recurrence. Patients should be counselled regarding prevention.
Special Populations
Aboriginal and Torres Strait Islander Health
📚 References
- 1. Harden RN, Bruehl S, Perez RSGM, et al. Validation of proposed diagnostic criteria (the "Budapest Criteria") for Complex Regional Pain Syndrome. Pain. 2010;150(2):268–274.
- 2. Harden RN, Oaklander AL, Burton AW, et al. Complex regional pain syndrome: practical diagnostic and treatment guidelines, 4th edition. Pain Medicine. 2013;14(2):180–229.
- 3. Moseley GL. Graded motor imagery is effective for long-standing complex regional pain syndrome: a randomised controlled trial. Pain. 2004;108(1–2):192–198.
- 4. Bowering KJ, O'Connell NE, Tabor A, et al. The effects of graded motor imagery and its components on chronic pain: a systematic review and meta-analysis. The Journal of Pain. 2013;14(1):3–13.
- 5. Varenna M, Adami S, Rossini M, et al. Treatment of complex regional pain syndrome type I with neridronate: a randomized, double-blind, placebo-controlled study. Rheumatology. 2013;52(3):534–542.
- 6. Sigtermans MJ, van Hilten JJ, Bauer MCR, et al. Ketamine produces effective and long-term pain relief in patients with Complex Regional Pain Syndrome Type 1. Pain. 2009;145(3):304–311.
- 7. Manicourt DH, Brasseur JP, Boutsen Y, et al. Role of alendronate in therapy for posttraumatic complex regional pain syndrome type I of the lower extremity. Arthritis & Rheumatism. 2004;50(11):3690–3697.
- 8. Oerlemans HM, Oostendorp RAB, de Boo T, Goris RJA. Pain and reduced mobility in complex regional pain syndrome I: outcome of a prospective randomised controlled clinical trial of adjuvant physical therapy versus occupational therapy. Pain. 1999;83(1):77–83.
- 9. de Mos M, de Bruijn AGJ, Huygen FJPM, et al. The incidence of complex regional pain syndrome: a population-based study. Pain. 2007;129(1–2):12–20.
- 10. Bruehl S. An update on the pathophysiology of complex regional pain syndrome. Anesthesiology. 2010;113(3):713–725.
- 11. Royal Australian College of General Practitioners (RACGP). Prescription of opioids for chronic non-cancer pain. East Melbourne: RACGP; 2020.
- 12. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 13. Australian Institute of Health and Welfare (AIHW). Chronic pain in Aboriginal and Torres Strait Islander peoples. Canberra: AIHW; 2022.
- 14. Goebel A, Bijnens E, Khurana A, et al. Intravenous immunoglobulin treatment of the complex regional pain syndrome: a randomized trial. Annals of Internal Medicine. 2017;166(11):808–816.
- 15. Marinus J, Moseley GL, Birklein F, et al. Clinical features and pathophysiology of complex regional pain syndrome. The Lancet Neurology. 2011;10(7):637–648.