📋 Key Information Summary
- Small cell lung cancer (SCLC) accounts for approximately 13–15% of all lung cancers in Australia, with strong association to cigarette smoking; incidence is declining in line with reduced smoking prevalence.
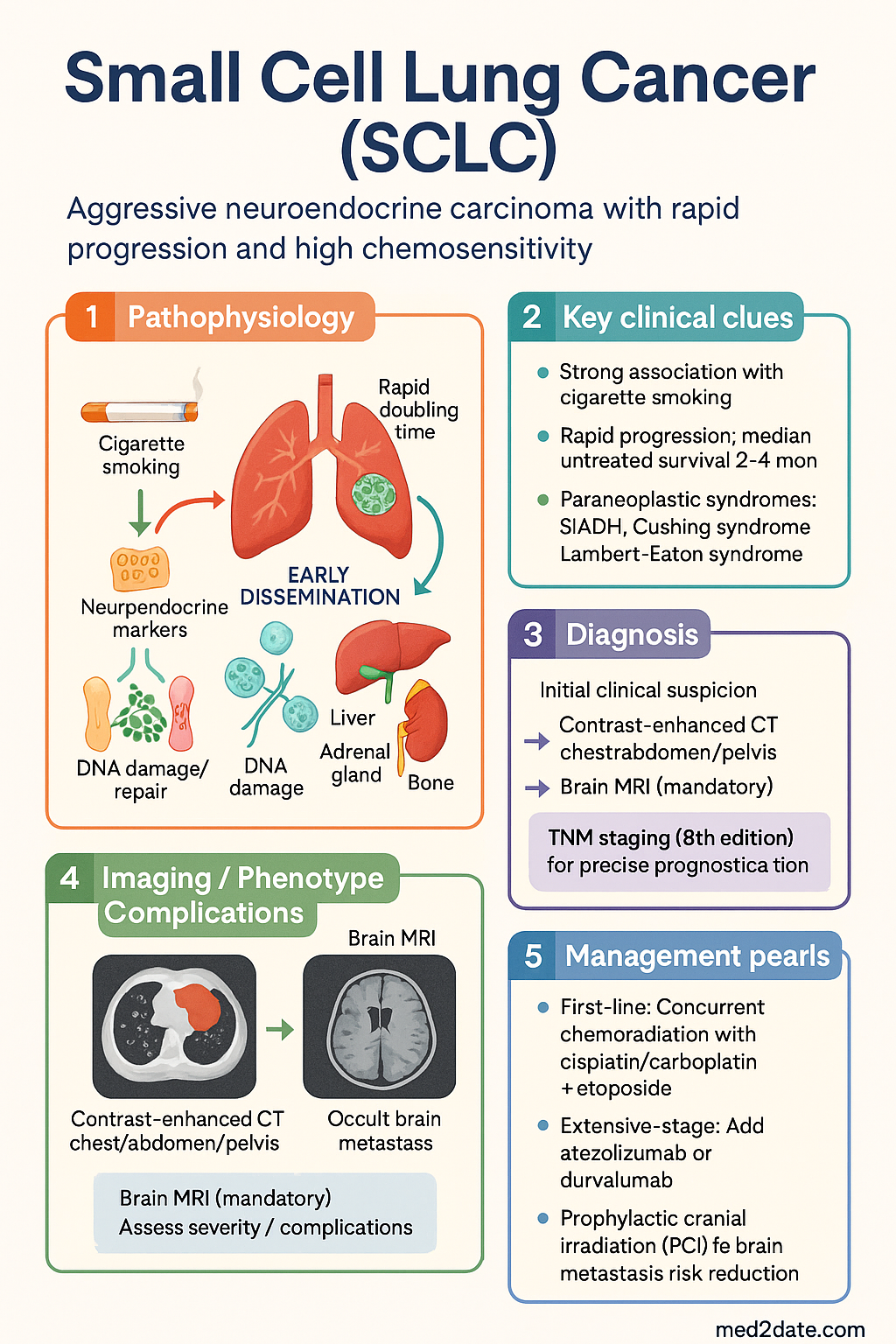
- SCLC is staged as limited stage (LS) (confined to one hemithorax and regional nodes, manageable within a single radiation field) or extensive stage (ES) (disease beyond these boundaries); TNM staging (8th edition) is increasingly used alongside the traditional two-stage system.
- Staging workup requires contrast-enhanced CT chest/abdomen/pelvis, brain MRI (mandatory), PET-CT (if available and will change management), and baseline bloods including LDH, sodium, and liver function tests.
- SCLC is characterised by rapid doubling time, early dissemination, and initial high chemosensitivity followed by near-universal relapse; median untreated survival is 2–4 months.
- Limited-stage first-line: Concurrent chemoradiation with cisplatin (or carboplatin) + etoposide combined with thoracic radiotherapy (45 Gy BID over 3 weeks preferred); deliver within the first 1–2 chemotherapy cycles.
- Extensive-stage first-line: Platinum + etoposide with atezolizumab (Tecentriq®) or durvalumab (Imfinzi®) for 4 cycles, followed by maintenance immunotherapy until progression or unacceptable toxicity.
- Prophylactic cranial irradiation (PCI) (25 Gy in 10 fractions) is recommended for patients with any-stage SCLC who achieve a good response, reducing brain metastasis risk by ~50% and improving overall survival.
- For extensive-stage patients who decline or are unfit for PCI, surveillance brain MRI every 3 months for 12 months is an acceptable alternative.
- Second-line options include lurbinectedin (Zepzelca®), temozolomide, topotecan, CAV (cyclophosphamide/doxorubicin/vincristine), or re-challenge with platinum/etoposide if relapse occurs >6 months after first-line (sensitive relapse).
- Paraneoplastic syndromes are common: SIADH (15%), Cushing syndrome (ectopic ACTH), Lambert-Eaton myasthenic syndrome, and hypercalcaemia; screen and manage alongside oncological treatment.
- Aboriginal and Torres Strait Islander Australians have higher lung cancer incidence and mortality, later-stage presentation, and lower treatment rates; culturally safe pathways and multidisciplinary input are essential.
- All SCLC patients should be discussed at a specialist lung cancer multidisciplinary team (MDT) meeting and referred early to palliative care for symptom management alongside active treatment.
Introduction & Australian Epidemiology
Small cell lung cancer (SCLC) is a high-grade neuroendocrine carcinoma of the lung distinguished by rapid proliferation, early metastatic spread, and initial exquisite chemosensitivity. It represents approximately 13–15% of all primary lung malignancies in Australia and is strongly linked to cigarette smoking, with >95% of cases occurring in current or former smokers. The disease is characterised by a very short doubling time (typically 30–60 days) and propensity for early haematogenous dissemination to the brain, liver, adrenal glands, and bone.
In Australia, lung cancer remains the fifth most commonly diagnosed cancer and the leading cause of cancer-related death. SCLC-specific data from the Australian Institute of Health and Welfare (AIHW) indicate approximately 2,000–2,500 new SCLC diagnoses annually. Five-year overall survival remains poor at approximately 6–8% for all stages combined, though limited-stage disease treated with concurrent chemoradiation achieves 2-year survival rates of 20–40%.
The incidence of SCLC has been gradually declining in Australia, paralleling national reductions in smoking prevalence achieved through public health measures such as plain packaging legislation and tobacco excise increases. However, SCLC in never-smokers remains exceptionally rare (<2–3% of cases). Rural and remote Australians, including Aboriginal and Torres Strait Islander peoples, experience disproportionate lung cancer burden due to higher smoking rates and delayed access to diagnosis and treatment.
Staging & Classification
Two-Stage System (Veterans Administration Classification)
The traditional two-stage system remains the most widely used framework for SCLC treatment planning in Australia:
TNM Staging (AJCC 8th Edition)
The AJCC TNM 8th edition staging system is increasingly applied to SCLC, allowing more precise prognostication. Limited stage broadly corresponds to TNM stages I–IIIB (T1–4, N0–3, M0), while extensive stage corresponds to stage IV (M1a/b/c) or T4/N3 disease not amenable to a single radiation field. TNM staging is recommended for surgical candidates (rare in SCLC) and clinical trial eligibility.
Staging Workup
Histological Subtypes
SCLC is classified into:
- Pure SCLC: Classic small cells with scant cytoplasm, finely granular "salt-and-pepper" chromasm, nuclear moulding, and very high mitotic rate. Accounts for ~90% of cases.
- Combined SCLC: SCLC with a component of NSCLC (adenocarcinoma, squamous cell carcinoma, or large cell carcinoma) comprising ≥10% of the tumour. Treat as SCLC unless the NSCLC component is predominant and actionable mutations are identified.
Treatment Approach
First-Line Chemotherapy Backbone
The platinum/etoposide doublet has been the standard of care for SCLC since the 1980s and remains the chemotherapy backbone for both limited and extensive stage disease. In Australia, either cisplatin or carboplatin may be used; carboplatin is preferred for patients with renal impairment, hearing loss, or when reduced infusion time is desired.
Immunotherapy Addition (Extensive Stage)
The addition of immune checkpoint inhibitors (ICIs) targeting PD-L1 to platinum/etoposide has become the standard of care for ES-SCLC following the IMpower133 and CASPIAN trials. Two agents are PBS-listed in Australia for this indication:
Thoracic Radiotherapy
Thoracic radiotherapy (TRT) is a critical component of limited-stage treatment. The preferred regimen is 45 Gy in 30 fractions delivered twice daily (BID) over 3 weeks (Turrisi regimen), concurrent with cycles 1–2 of EP. Hyperfractionated BID TRT demonstrated superior survival compared with once-daily 45 Gy in the pivotal Intergroup 0096 trial. Where BID scheduling is not feasible, once-daily TRT (60–70 Gy over 6–7 weeks) is an acceptable alternative per current evidence.
Prophylactic Cranial Irradiation (PCI)
SCLC has a high propensity for brain metastases: 50–60% at 2 years without PCI. PCI reduces the incidence of brain metastases by approximately 50% and confers an overall survival benefit of ~5% at 3 years. The standard dose is 25 Gy in 10 fractions. PCI is recommended for:
- All limited-stage patients who achieve a complete or near-complete response after chemoradiation
- Extensive-stage patients who achieve any response to first-line chemotherapy ± immunotherapy
- PCI is typically commenced 3–4 weeks after completion of systemic therapy
Timing of Chemotherapy and Radiotherapy
In limited-stage disease, concurrent chemoradiation should commence within the first 1–2 cycles of chemotherapy. Early concurrent therapy (starting with cycle 1 or 2) is associated with superior outcomes compared with delayed sequential therapy. Ensure adequate performance status (ECOG 0–2), pulmonary function (FEV₁ ≥1.0 L), and renal function before initiating concurrent treatment.
Limited Stage Management
Treatment Algorithm
Concurrent Chemoradiation Regimen
| Component | Preferred Regimen | Alternative |
|---|---|---|
| Chemotherapy | Cisplatin 60 mg/m² Day 1 + Etoposide 120 mg/m² Days 1–3, q21d × 4 cycles | Carboplatin AUC 5 Day 1 + Etoposide 100 mg/m² Days 1–3, q21d × 4 cycles |
| Thoracic RT | 45 Gy in 30 fractions BID (1.5 Gy/fraction) over 3 weeks | 60–70 Gy in 30–35 fractions once daily over 6–7 weeks |
| RT timing | Commence with cycle 1 or 2 of chemotherapy (early concurrent) | Must be completed by end of cycle 4 at latest |
| PCI | 25 Gy in 10 fractions (post-treatment, if good response) | Omitted with brain MRI surveillance if patient declines or unfit |
Surgical Management (Rare)
Surgery plays a very limited role in SCLC and is considered only for clinical stage I (T1–2, N0, M0) disease after thorough staging including mediastinoscopy or EBUS confirmation of N0 status. Adjuvant platinum-based chemotherapy (± PCI) should follow surgical resection. In practice, fewer than 2–5% of SCLC patients in Australia are surgical candidates.
Surveillance Protocols
Following completion of definitive therapy for limited-stage SCLC:
- Years 1–2: CT chest/abdomen/pelvis every 3 months; brain MRI every 3–6 months (if no PCI) or at clinician discretion (if PCI delivered)
- Years 3–5: CT chest every 6 months; brain MRI annually or if symptomatic
- Beyond 5 years: Annual CT chest; clinical review; smoking cessation support; assess for late treatment effects (cardiac, pulmonary fibrosis, neurocognitive decline)
Extensive Stage Management
First-Line Therapy
The current standard of care for ES-SCLC in Australia is platinum/etoposide combined with an anti-PD-L1 antibody (atezolizumab or durvalumab) for 4 cycles, followed by maintenance immunotherapy. This represents the most significant advance in SCLC treatment in three decades, providing a modest but clinically meaningful overall survival improvement of approximately 2–3 months compared with chemotherapy alone.
Phase III, 403 patients. Carboplatin/etoposide ± atezolizumab × 4 cycles → maintenance atezolizumab. Median OS: 12.3 vs 10.3 months (HR 0.70, p=0.007). 1-year OS: 51.7% vs 38.2%. Benefit seen across subgroups.
Phase III, 537 patients. Platinum/etoposide ± durvalumab × 4 cycles → maintenance durvalumab. Median OS: 13.0 vs 10.3 months (HR 0.73, p=0.0047). Flexible platinum choice (cisplatin or carboplatin).
First-Line Regimen Summary
Palliative Radiotherapy
Consolidative thoracic radiotherapy may be considered in ES-SCLC patients who achieve a good response to systemic therapy, based on the CREST trial suggesting potential benefit in selected patients. Palliative radiotherapy is indicated for symptomatic metastases (bone pain, superior vena cava obstruction, brain metastases, spinal cord compression).
Management of CNS Metastases
Brain metastases are present in 10–15% of ES-SCLC at diagnosis and develop in up to 50–60% during the disease course. Management depends on symptoms, number of lesions, and performance status:
| Clinical Scenario | Recommended Approach |
|---|---|
| Asymptomatic, limited brain metastases (1–3) | Stereotactic radiosurgery (SRS) if available, followed by systemic therapy. Consider PCI if no prior PCI. |
| Symptomatic, multiple brain metastases | Dexamethasone 8–16 mg/day IV/PO + whole brain radiotherapy (WBRT, 30 Gy / 10 fractions). Systemic therapy if performance status allows. |
| Brain metastases with impending herniation | Emergency neurosurgical referral if accessible lesion. Dexamethasone 10 mg IV stat then 4 mg IV q6h. Palliative WBRT. |
| Previously received PCI, now relapse in brain | SRS preferred if ≤4 lesions; WBRT if widespread. Re-challenge with PCI generally not recommended. |
Second-Line and Relapsed Disease
Nearly all SCLC patients will relapse after first-line therapy. Prognosis in relapsed disease is poor, with median survival of 4–6 months. Treatment choice depends on the relapse-free interval:
- Refractory disease (progression during or within 90 days of first-line): Poor prognosis; consider clinical trial, lurbinectedin, temozolomide, or best supportive care.
- Sensitive relapse (relapse >90 days after completing first-line): Re-challenge with platinum/etoposide is reasonable, particularly if relapse-free interval >6 months. Response rates 25–40%.
Supportive Care & Symptom Management
Early integration of palliative care improves quality of life and may improve survival in SCLC. Key supportive care considerations include:
- Pain management: WHO analgesic ladder; radiotherapy for painful bone metastases; bone-modifying agents (denosumab 120 mg SC q4w or zoledronic acid 4 mg IV q4w) for lytic bone metastases
- Superior vena cava (SVC) obstruction: Emergency radiotherapy and/or stenting; dexamethasone 8 mg IV
- Spinal cord compression: Dexamethasone 16 mg IV stat + urgent MRI + emergency radiotherapy within 24 hours; neurosurgical consultation if instability or diagnostic uncertainty
- Neutropenic sepsis: Assess febrile neutropenia risk; G-CSF (filgrastim/pegfilgrastim) support if ≥20% risk per NCCN criteria or previous episode. Empirical piperacillin/tazobactam 4.5 g IV q6h or cefepime 2 g IV q8h as per local protocols
- Thromboprophylaxis: Consider LMWH (enoxaparin 40 mg SC daily) for VTE prophylaxis in hospitalised cancer patients; SCLC carries high VTE risk
- Anti-emesis: NK1 antagonist (aprepitant) + 5HT3 antagonist (ondansetron) + dexamethasone for highly emetogenic cisplatin-containing regimens
Paraneoplastic Syndromes
| Syndrome | Incidence | Mechanism | Management |
|---|---|---|---|
| SIADH | 15% | Ectopic ADH secretion | Fluid restriction (<1 L/day), NaCl tablets, demeclocycline, tolvaptan; chemotherapy typically resolves SIADH |
| Ectopic ACTH / Cushing syndrome | 2–5% | Ectopic ACTH production | Ketoconazole 200 mg TDS or metyrapone for cortisol control; treat underlying SCLC urgently |
| Lambert-Eaton myasthenic syndrome (LEMS) | 3% | Anti-VGCC antibodies | 3,4-diaminopyridine (amifampridine); IVIG; treat SCLC; may improve with immunotherapy |
| Dermatomyositis | <1% | Immune-mediated | Corticosteroids; dermatology/rheumatology input; treat underlying malignancy |
Special Populations
Pregnancy
Paediatrics
Elderly (≥70 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Horn L, Mansfield AS, Szczęsna A, et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N Engl J Med. 2018;379(23):2220–2229. doi:10.1056/NEJMoa1809064
- 2. Paz-Ares L, Dvorkin M, Chen Y, et al. Durvalumab plus platinum–etoposide versus platinum–etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomised, controlled, open-label, phase 3 trial. Lancet. 2019;394(10212):1929–1939. doi:10.1016/S0140-6736(19)32222-6
- 3. Turrisi AT, Kim K, Blum R, et al. Twice-daily compared with once-daily thoracic radiotherapy in limited small-cell lung cancer treated concurrently with cisplatin and etoposide. N Engl J Med. 1999;340(4):265–271. doi:10.1056/NEJM199901283400403
- 4. Aupérin A, Arriagada R, Pignon JP, et al. Prophylactic cranial irradiation for patients with small-cell lung cancer in complete remission. N Engl J Med. 1999;341(7):476–484. doi:10.1056/NEJM199908123410703
- 5. Slotman BJ, Faivre-Finn C, Kramer G, et al. Prophylactic cranial irradiation in extensive small-cell lung cancer. N Engl J Med. 2007;357(7):664–672. doi:10.1056/NEJMoa071780
- 6. Trigo J, Subbiah V, Besse B, et al. Lurbinectedin as second-line treatment for patients with small-cell lung cancer: a single-arm, open-label, phase 2 basket trial. Lancet Oncol. 2020;21(5):645–654. doi:10.1016/S1470-2045(20)30068-1
- 7. National Health and Medical Research Council (NHMRC). Clinical Practice Guidelines for the Prevention, Diagnosis, and Management of Lung Cancer. Canberra: NHMRC; 2024.
- 8. Australian Institute of Health and Welfare (AIHW). Cancer in Australia 2023: AIHW Cat. No. CAN 143. Canberra: AIHW; 2023.
- 9. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework: Lung Cancer. Canberra: AIHW; 2023.
- 10. National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology: Small Cell Lung Cancer. Version 2.2024. Plymouth Meeting, PA: NCCN; 2024.
- 11. Früh M, De Ruysscher D, Popat S, et al. Small-cell lung cancer (SCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24(Suppl 6):vi99–vi105. doi:10.1093/annonc/mdt178
- 12. Cancer Council Australia. Lung Cancer Guidelines Wiki. Sydney: Cancer Council Australia; 2024. Available at: wiki.cancer.org.au
- 13. Goldstraw P, Chansky K, Crowley J, et al. The IASLC Lung Cancer Staging Project: proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM Classification for Lung Cancer. J Thorac Oncol. 2016;11(1):39–51. doi:10.1016/j.jtho.2015.09.009
- 14. Slotman BJ, van Tinteren H, Praag JO, et al. Use of thoracic radiotherapy for extensive stage small-cell lung cancer: a phase 3 randomised controlled trial. Lancet. 2015;385(9962):36–42. doi:10.1016/S0140-6736(14)61183-8
- 15. Royal Australian College of General Practitioners (RACGP). Guidelines for Preventive Activities in General Practice. 9th edn. Melbourne: RACGP; 2018.