📋 Key Information Summary
- Occupational lung diseases remain a significant cause of morbidity and mortality in Australia, with asbestos-related diseases, silicosis, coal workers' pneumoconiosis (CWP), and occupational asthma being the most prevalent conditions.
- A thorough occupational exposure history is the cornerstone of diagnosis — always ask about job titles, duration, specific agents, use of respiratory protective equipment (RPE), and latent period since first exposure.
- Asbestos-related diseases (asbestosis, pleural plaques, mesothelioma, lung cancer) continue to emerge decades after exposure due to Australia's historically heavy use; mesothelioma incidence in Australia remains among the highest globally.
- Silicosis is re-emerging in Australia, particularly from engineered stone (Caesarstone®, Smartstone®) fabrication — acute, accelerated, and chronic forms are recognised; all notifiable under state WHS legislation.
- Coal workers' pneumoconiosis was re-identified in Queensland in 2015 after being thought eradicated; mandatory screening with ILO-classified chest X-ray and low-dose CT is now required in coal mining states.
- Occupational asthma accounts for approximately 15–25% of adult-onset asthma; it is classified as sensitizer-induced (late-onset, immunological) or irritant-induced (reactive airways dysfunction syndrome — RADS).
- High-resolution CT (HRCT) chest is the imaging modality of choice for parenchymal occupational lung disease; plain chest X-ray remains important for screening and ILO classification.
- Spirometry with DLCO is essential baseline and surveillance testing; serial spirometry is mandated for at-risk workers in mining, stone fabrication, and asbestos-related industries.
- Definitive treatment for most pneumoconioses involves removal from exposure; immunosuppressive therapy has no proven role; lung transplantation may be considered for end-stage disease.
- Compensation and reporting obligations vary by state — most occupational lung diseases are notifiable under workers' compensation schemes; Safe Work Australia and state Work Health Safety (WHS) regulators must be notified for certain conditions (silicosis, mesothelioma).
- Aboriginal and Torres Strait Islander Australians face disproportionate risk through overrepresentation in mining, construction, and agricultural industries, combined with barriers to surveillance access in remote communities.
- Berylliosis, hard metal lung disease, organic dust toxic syndrome (ODTS), and building-related illness (sick building syndrome) are less common but important differential diagnoses in workers with relevant exposures.
- Prevention is paramount — workplace exposure limits (WELs) set by Safe Work Australia, engineering controls (LEV, wet suppression), and properly fitted P2/N95 respirators are essential interventions.
Introduction & Australian Epidemiology
Occupational lung diseases encompass a heterogeneous group of respiratory conditions caused by inhalation of dusts, fibres, fumes, chemicals, and biological agents in the workplace. In Australia, these conditions continue to impose a substantial burden despite decades of regulatory intervention and workplace health and safety reforms. The Australian Institute of Health and Welfare (AIHW) estimates that occupational exposures contribute to approximately 5,000 deaths and 140,000 disability-adjusted life years (DALYs) annually in Australia, with respiratory diseases being the leading cause of occupational mortality.
Australia has a particularly significant history with asbestos-related disease due to the widespread use of asbestos-containing materials (ACMs) from the 1940s to the mid-1980s, including the legacy of asbestos mining at Wittenoom in Western Australia. The country continues to experience one of the highest incidences of malignant mesothelioma globally, with approximately 700–800 new cases diagnosed annually.
The resurgence of silicosis in Australia, particularly among engineered stone workers since approximately 2015, has been described as a public health emergency. Safe Work Australia and state regulators have responded with emergency codes of practice, mandatory notification, and prohibition of dry-cutting of engineered stone (with a complete ban on engineered stone products from 1 July 2024).
| Disease | Estimated Annual Cases (Australia) | Latency Period | Key Industries |
|---|---|---|---|
| Malignant mesothelioma | 700–800 | 20–50 years | Construction, shipbuilding, mining, plumbing, electrical |
| Asbestosis | Declining; historical peak ongoing | 10–20+ years | Asbestos mining, insulation, construction |
| Silicosis | ~350+ notifications (2019–2023) | Acute: weeks–months; Chronic: 10–30 years | Engineered stone fabrication, tunnelling, quarrying, sandblasting |
| Coal workers' pneumoconiosis | ~100+ identified since 2015 screening | 10–20+ years | Underground and open-cut coal mining |
| Occupational asthma | ~3,000–5,000 (estimated) | Months–years (sensitizers); 24 hours (RADS) | Baking, painting, isocyanate manufacturing, healthcare, agriculture |
Asbestos-Related Disease
Asbestos-related diseases represent the most significant occupational health legacy in Australia. Despite a total ban on asbestos import and use since 31 December 2003, the long latency periods (often 20–50 years) mean that new cases continue to emerge. The National Strategic Plan for Asbestos Management and Awareness (2019–2023, now updated) guides Australia's approach to managing residual asbestos in buildings, infrastructure, and the environment.
Types of Asbestos Fibres
| Type | Mineral Group | Fibre Shape | Pathogenicity | Australian Context |
|---|---|---|---|---|
| Chrysotile (white) | Serpentine | Curled, flexible | Most commonly used; carcinogenic | 95% of world asbestos use; common in ACMs |
| Crocidolite (blue) | Amphibole | Straight, brittle | Most potent for mesothelioma | Mined at Wittenoom, WA (1943–1966) |
| Amosite (brown) | Amphibole | Straight, brittle | Highly carcinogenic | Imported in asbestos-cement products |
Asbestosis
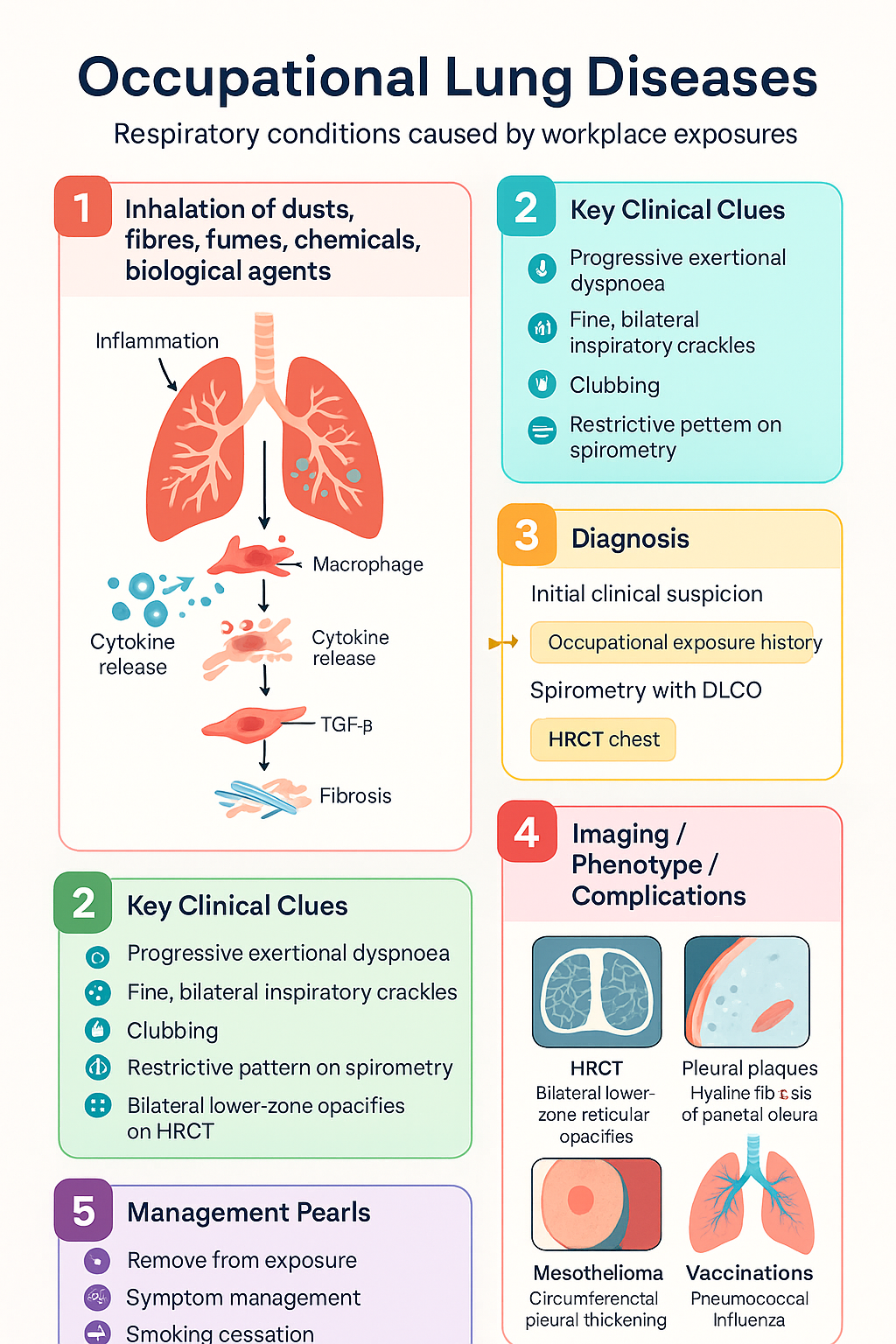
Asbestosis is a chronic, diffuse interstitial fibrosis of the lung parenchyma caused by inhalation of asbestos fibres. It requires substantial cumulative exposure (typically ≥25 fibre-years/mL, though lower exposures can cause disease) and has a latency of 10–20 years or more. There is no effective treatment beyond removal from further exposure and supportive care.
Clinical Features
- Progressive exertional dyspnoea over months to years
- Fine, bilateral, bibasilar inspiratory crackles ("velcro crackles")
- Clubbing (present in 30–50% of cases)
- Restrictive pattern on spirometry with reduced DLCO
- Bilateral lower-zone reticular or reticulonodular opacities on HRCT
- Bilateral lower-zone pleural plaques (often co-exist)
Pleural Plaques
Pleural plaques are the most common manifestation of asbestos exposure, affecting up to 50–60% of heavily exposed individuals. They represent localised hyaline fibrosis of the parietal pleura, typically on the posterolateral chest wall, diaphragmatic pleura, and mediastinal pleura. Pleural plaques are generally considered benign and do not progress to malignancy, though they indicate significant asbestos exposure and confer increased risk of other asbestos-related conditions.
Malignant Mesothelioma
Malignant mesothelioma is an aggressive malignancy of the serosal membranes (pleura, peritoneum, pericardium, tunica vaginalis) almost universally caused by asbestos exposure. Australia has one of the highest per capita rates globally. The median survival from diagnosis is 8–14 months with best supportive care, and 12–18 months with modern systemic therapy.
Diagnostic Pathway
- Clinical suspicion: Unilateral pleural effusion or pleural thickening in a patient with asbestos exposure history
- CT chest with contrast: Circumferential pleural thickening, nodularity, mediastinal pleural involvement, contraction of hemithorax
- Pleural fluid analysis: Cytology has low sensitivity (20–30%); elevated hyaluronic acid is suggestive
- Tissue biopsy: Definitive diagnosis requires histological examination; CT-guided core biopsy or thoracoscopic biopsy (VATS preferred)
- Immunohistochemistry: Calretinin+, WT-1+, CK5/6+, D2-40+ (epithelioid); negative carcinoma markers (TTF-1, CEA, BerEP4)
- BAP1 and MTAP loss: Molecular markers supporting mesothelioma diagnosis
Asbestos-Related Lung Cancer
Asbestos exposure increases the risk of bronchogenic carcinoma approximately 5-fold; this risk is multiplicative with cigarette smoking (up to 50–90-fold combined risk). Unlike mesothelioma, no specific histological type is pathognomonic, though adenocarcinoma and squamous cell carcinoma are most common. The latency period is typically 15–35 years.
Surveillance & Monitoring
Workers with significant asbestos exposure should undergo periodic medical surveillance as per the Safe Work Australia Model Code of Practice: Managing and Removing Asbestos.
Management Principles
Silicosis
Silicosis is caused by inhalation of respirable crystalline silica (RCS) dust, predominantly quartz (SiO₂). It is one of the oldest known occupational diseases and is now re-emerging in Australia as a modern epidemic, primarily driven by the engineered stone (Caesarstone®, Smartstone®, Essastone®) benchtop fabrication industry. The disease is entirely preventable through effective dust control.
In 2024, Australia became the first country in the world to ban the use, supply, and manufacture of engineered stone products (effective 1 July 2024), following an unprecedented spike in accelerated and chronic silicosis cases among stonemasons, many of whom were young workers aged 20–40.
Classification of Silicosis
Diagnostic Evaluation
Prevention & Workplace Controls
Treatment of Silicosis
- Removal from exposure: Mandatory for all forms of silicosis; further exposure accelerates progression even in chronic disease
- Whole lung lavage (WLL): Considered for acute silicoproteinosis and severe accelerated silicosis; performed under general anaesthesia; may improve gas exchange; limited evidence base — specialist centres only
- Corticosteroids: No proven benefit for chronic silicosis; may be trialled in acute silicoproteinosis or rapidly progressive disease on a case-by-case basis
- TB prophylaxis: Treat latent TB infection (LTBI) if identified in a silicotic patient — increased progression risk to active TB; 3 months isoniazid + rifampicin (3HR) or 4 months rifampicin (4R) preferred per Australian TB guidelines
- Lung transplantation: Consider for end-stage silicosis with progressive respiratory failure; refer to transplant centre early; Australian transplant centres in Sydney, Melbourne, Brisbane, Adelaide, Perth
- Supportive care: Pulmonary rehabilitation, supplemental oxygen if hypoxaemic, vaccination (influenza, pneumococcal, COVID-19), smoking cessation
Complicated Silicosis (Progressive Massive Fibrosis)
Complicated silicosis occurs when individual silicotic nodules coalesce into conglomerate masses ≥1 cm (ILO classification category B or C). This is termed progressive massive fibrosis (PMF). PMF is characterised by:
- Large, dense, upper-zone fibrotic masses, typically bilateral and symmetrical
- Progressive respiratory impairment with marked reduction in FVC, FEV1, and DLCO
- Traction bronchiectasis, emphysematous changes, and cor pulmonale in advanced disease
- Often progressive even after cessation of exposure
- May mimic malignancy on imaging — tissue diagnosis may be required
Coal Workers' Pneumoconiosis (CWP)
Coal workers' pneumoconiosis (CWP), also known as "black lung," is caused by inhalation of coal mine dust, which contains a mixture of coal particles, silica, and other mineral dusts. CWP was thought to have been eradicated in Australia until 2015, when cases were identified in Queensland coal miners through the newly implemented screening program. Subsequent investigations revealed under-diagnosis spanning decades, with cases also identified in New South Wales.
Classification: Simple vs Complicated CWP
Australian Screening Programs
Following the 2015 Queensland identification, mandatory screening programs were established in major coal-producing states:
| State/Territory | Legislation/Program | Screening Requirement | Key Features |
|---|---|---|---|
| Queensland | Coal Mine Workers' Health Scheme (CMWHS) | Pre-employment + periodic (annually for underground; every 3 years for open-cut after 5 years) | ILO-classified CXR by two independent B-readers; low-dose CT for discordant or abnormal results; spirometry; questionnaires |
| New South Wales | Coal Services Health Surveillance | Pre-employment + periodic | Similar to QLD model; ILO-classified CXR; spirometry |
| Other states | Various WHS regulations | Employer-facilitated health assessments | No mandatory B-reader classification; physician discretion |
Associated Conditions
- Dust-related diffuse fibrosis (DRDF): Interstitial fibrosis pattern distinct from silicosis; may coexist with CWP; restrictive physiology
- COPD/chronic bronchitis: Coal mine dust exposure is an independent risk factor for COPD, even in non-smokers
- Rheumatoid arthritis — Caplan syndrome: Rheumatoid nodules in the lungs of coal workers with RA; distinctive "eggshell" calcification pattern
- Lung cancer: Coal mine dust is classified by IARC as Group 1 carcinogen (coal gasification) / Group 2A (underground mining)
Management
- Removal from further coal dust exposure — essential for all diagnosed cases
- Serial spirometry and imaging to monitor for progression
- Smoking cessation — critical; multiplicative risk with coal dust for COPD and lung cancer
- Pulmonary rehabilitation for symptomatic patients
- Long-term oxygen therapy if resting PaO₂ ≤55 mmHg or ≤59 mmHg with cor pulmonale
- Vaccination: influenza (annually), pneumococcal (PCV20 or PCV13 + PPSV23), COVID-19
- Workers' compensation notification — all CWP diagnoses should be lodged with relevant state workers' compensation authority
- Lung transplantation referral for end-stage PMF with respiratory failure
Occupational Asthma
Occupational asthma (OA) is defined as asthma caused by workplace exposure to airborne agents and accounts for approximately 15–25% of adult-onset asthma in Australia. It is classified into two major categories: sensitizer-induced (immunological) and irritant-induced asthma. Early recognition and removal from exposure are critical, as delay in diagnosis leads to progressive airway remodelling and irreversible disease.
Classification
| Feature | Sensitizer-Induced OA | Irritant-Induced OA (RADS) |
|---|---|---|
| Mechanism | Immunological (IgE-mediated or non-IgE) | Direct airway epithelial injury; neurogenic inflammation |
| Latency period | Months to years (months–5 years typical) | 24 hours (single high-level irritant exposure) or cumulative |
| Dose-response | May occur at low doses once sensitized | Requires high-level acute exposure (single event) or repeated moderate exposure |
| Common agents | Isocyanates, flour/grain dust, latex, wood dusts (western red cedar), laboratory animal allergens, glutaraldehyde, epoxy resins | Chlorine, ammonia, SO₂, nitrogen oxides, fires, chemical spills |
| Prognosis | Improves with early removal; persistent if delayed >1–2 years | Often persistent; ~70% have persistent symptoms at 2 years |
| Peak expiratory flow (PEF) pattern | Work-related variability (≥20% diurnal variation on work days) | Persistent low variability pattern; less diurnal variation |
High-Risk Occupations & Agents in Australia
| Industry/Occupation | Causative Agent | Type |
|---|---|---|
| Baking/pastry | Flour dust, α-amylase | IgE-mediated sensitizer |
| Spray painting, foam manufacturing | Isocyanates (MDI, TDI, HDI) | IgE or non-IgE sensitizer |
| Healthcare/latex-exposed workers | Natural rubber latex proteins | IgE-mediated sensitizer |
| Woodworking | Western red cedar (plicatic acid), other hardwoods | Non-IgE sensitizer |
| Animal handlers, laboratory workers | Rat/rodent urinary proteins | IgE-mediated sensitizer |
| Agriculture, farming | Grain dust, pesticides, animal dander | Mixed |
| Chemical industry, cleaning | Chlorine, ammonia, cleaning agents | Irritant (RADS) |
| Mining, tunnelling | Diesel exhaust, blasting fumes | Irritant/non-specific |
Diagnostic Evaluation
A systematic approach to diagnosing occupational asthma is essential. The following investigations should be performed in a stepwise manner:
Management & Removal from Exposure
- Step 1 — Remove or reduce exposure: Ideally complete removal from the causative agent; if not feasible, relocate to a non-exposed area of the workplace with effective respiratory protection
- Step 2 — Pharmacological treatment: Standard asthma management per Australian Asthma Handbook — SABA PRN → low-dose ICS → ICS/LABA combination → add-on therapy (LTRA, LAMA, biologics if severe)
- Step 3 — Monitoring: Serial spirometry, PEF, FeNO, symptom scores; reassess at 3, 6, and 12 months post-exposure cessation
- Step 4 — Compensation: Lodgement of workers' compensation claim; occupational physician assessment; medicolegal documentation of causation
Compensation & Medicolegal Considerations
- Occupational asthma is a compensable condition under all Australian state and territory workers' compensation schemes
- A diagnosis made by a respiratory physician or occupational physician strengthens the claim
- Documentation of the causal agent, exposure history, temporal relationship, and objective test results is essential
- Some states (e.g., NSW) have presumptive provisions for certain occupation-agent pairs (e.g., bakers with flour-related asthma)
- Claims should be lodged as soon as possible; retrospective claims are possible but may face greater scrutiny
- Safe Work Australia Work-Related Disease Indicators provide guidance on notification obligations
Other Occupational Exposures
Berylliosis (Chronic Beryllium Disease — CBD)
Chronic beryllium disease (CBD) is a granulomatous lung disease caused by inhalation of beryllium dust or fume, mediated by a T-cell hypersensitivity reaction. In Australia, exposure occurs primarily in the aerospace, electronics, nuclear, and defence industries, as well as dental alloy manufacturing and recycling. CBD is now rare in Australia due to strict workplace controls but remains important in the differential diagnosis of granulomatous lung disease.
- Pathophysiology: Beryllium acts as a hapten, forming complexes with endogenous proteins that trigger CD4+ T-cell–mediated granulomatous inflammation
- Susceptibility: HLA-DPB1 Glu69 genotype confers susceptibility — genetic testing available
- Clinical features: Progressive dyspnoea, cough, fatigue, weight loss; bilateral hilar lymphadenopathy; diffuse pulmonary infiltrates; granulomas on lung biopsy (histologically indistinguishable from sarcoidosis)
- Diagnosis: Beryllium lymphocyte proliferation test (BeLPT) — gold standard; performed on peripheral blood and/or BAL lymphocytes; HRCT chest; transbronchial or surgical lung biopsy showing non-caseating granulomas
- Treatment: No proven disease-modifying therapy; corticosteroids (prednisolone 0.5–1 mg/kg/day, weaned over months) may slow progression; long-term immunosuppression in progressive disease; removal from exposure mandatory
- WEL: Safe Work Australia — time-weighted average (TWA) 0.002 mg/m³; short-term exposure limit (STEL) 0.01 mg/m³
Hard Metal Lung Disease
Hard metal disease is caused by exposure to tungsten carbide, cobalt, and other metals used in cutting tools, drill bits, and grinding operations. The condition can present as:
- Interstitial lung disease (giant cell interstitial pneumonia — GIP): Characteristic multinucleated giant cells in BAL and lung tissue; pathognomonic finding; restrictive physiology with reduced DLCO
- Occupational asthma: Cobalt-induced asthma (sensitizer or irritant); may present independently of ILD
- Industries affected: Tool and die manufacturing, diamond polishing, mining, tungsten carbide production
- Diagnosis: BAL showing characteristic giant cells (cannibalistic lymphocytes); HRCT with ground-glass opacification and fibrosis; cobalt serum/urine levels; cobalt SPT or specific IgE if asthma predominant
- Treatment: Removal from exposure; corticosteroids (variable response); supportive care; no PBS-listed disease-specific therapy
Organic Dust Toxic Syndrome (ODTS)
ODTS is a non-infectious, febrile illness caused by inhalation of large quantities of organic dusts, mycotoxins, or endotoxins, typically in agricultural settings. It is distinct from hypersensitivity pneumonitis (HP) and is characterised by:
- Exposure: Mouldy hay, grain silos, composting, mushroom farming, cotton dust (byssinosis)
- Onset: 4–8 hours after heavy exposure; fever, chills, myalgia, malaise, dry cough, dyspnoea
- Distinguishing features from HP: No sensitization required; occurs on first heavy exposure; self-limiting within 24–48 hours; no progressive fibrosis; no specific IgG antibodies
- Investigation: Usually clinical diagnosis; CXR typically normal; FBC shows neutrophilic leukocytosis; inflammatory markers elevated
- Management: Self-limiting; supportive care; remove from exposure; prevention through dust control, P2 respirators, avoiding entry into enclosed grain silos
- Compensation: Not typically compensable as a chronic disease, but acute episodes may be covered under workers' compensation if work-related
Building-Related Illness (Sick Building Syndrome)
Building-related illness encompasses a spectrum of symptoms attributed to time spent in specific buildings, particularly those with poor ventilation, microbial contamination, or volatile organic compound (VOC) exposure. In Australia, it has been reported in office buildings, schools, and public buildings, particularly in tropical and subtropical regions where mould growth is prevalent.
- Symptoms: Non-specific — headache, fatigue, mucosal irritation (eyes, nose, throat), difficulty concentrating, skin irritation; typically improve when away from the building
- Contributing factors: Inadequate ventilation (CO₂ >1000 ppm), mould (Stachybotrys, Aspergillus, Cladosporium), VOCs from building materials and furnishings, poor temperature/humidity control, bioaerosols
- Investigation: Primarily environmental — building assessment by occupational hygienist; air quality monitoring; CO₂ levels; fungal culture; inspection for water damage and mould
- Management: Address building defects — improve ventilation (minimum 7.5 L/s per person per AS 1668.2), remediate mould, replace water-damaged materials, improve filtration; medical management is supportive; specific mould allergy or HP should be diagnosed separately
- WorkCover implications: Workers' compensation claims may be made for building-related illness if a causal link to the workplace is established; environmental assessment is critical evidence
Investigations
The investigation of suspected occupational lung disease requires a systematic, evidence-based approach. All investigations should be interpreted in the context of the occupational exposure history, clinical presentation, and imaging findings.
Risk Stratification & Severity Scoring
Risk stratification for occupational lung disease considers the intensity and duration of exposure, the specific agent, individual host factors, and the presence or absence of pre-existing lung disease. The following framework assists clinicians in categorising risk and determining the urgency and frequency of surveillance.
Empirical & Directed Therapy
Treatment of occupational lung diseases is largely supportive, as definitive disease-modifying therapy is limited for most pneumoconioses. The cornerstone of management is removal from further exposure, symptom management, and prevention of complications. Specific directed therapy exists for mesothelioma and occupational asthma.
General Principles of Management
Directed Therapy by Condition
Monitoring
Long-term monitoring is essential for all occupational lung diseases, both to detect progression and to identify new complications. Monitoring frequency depends on the condition, severity, and whether the patient continues to be exposed.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians face a disproportionate burden of occupational lung disease, driven by overrepresentation in high-risk industries (mining, construction, agriculture, manufacturing) and significant barriers to accessing surveillance, diagnosis, and treatment services. The intersection of occupational exposures with higher baseline rates of chronic respiratory disease, smoking, and social disadvantage amplifies health impacts in Indigenous communities.
Quick Reference Summary
📚 References
- 1. Safe Work Australia. Workplace Exposure Standards for Airborne Contaminants. Canberra: Safe Work Australia; 2024. Available from: www.safeworkaustralia.gov.au.
- 2. Hoy RF, Baird T, Hammerschlag G, et al. Artificial stone-associated silicosis: a rapidly emerging occupational lung disease. Occup Environ Med. 2019;76(11):808–810.
- 3. Australian Institute of Health and Welfare (AIHW). Occupational respiratory disease in Australia. Cat. no. PHE 280. Canberra: AIHW; 2021.
- 4. Wolfe R, Coggon D. Asbestos-related diseases in Australia — trends and projections. Aust N Z J Public Health. 2022;46(4):490–496.
- 5. Safe Work Australia. Model Code of Practice: How to Manage and Control Asbestos in the Workplace. Canberra: Safe Work Australia; 2018 (updated 2023).
- 6. Blackley DJ, Crum JB, Halldin CN, Storey E, Laney AS. Resurgence of progressive massive fibrosis in coal miners — Eastern Kentucky, 2016. MMWR Morb Mortal Wkly Rep. 2016;65(49):1385–1389. [Relevant to Australian screening program development.]
- 7. Occupational Safety and Health Administration (OSHA) / International Labour Organization (ILO). Guidelines for the Use of the ILO International Classification of Radiographs of Pneumoconioses, Revised Edition 2011. Geneva: ILO; 2011.
- 8. Bernstein IL, Chan-Yeung M, Malo JL, Bernstein DI. Asthma in the Workplace. 4th ed. Boca Raton: CRC Press; 2013.
- 9. Vandenplas O, Dressel H, Nowak D, et al. What is the optimal management strategy for occupational asthma? Eur Respir Rev. 2012;21(124):94–100.
- 10. Baur X, Sigsgaard T, Aasen TB, et al. Guidelines for the management of work-related asthma. Eur Respir J. 2012;39(3):656–673.
- 11. Mastrangelo G, Ballarin MN, Bellini E, et al. Asbestos exposure and cancer risk: a review. Am J Ind Med. 2019;62(7):553–572.
- 12. Tzilas V, Bouros D, Barbieri A, et al. ESMO Clinical Practice Guidelines: Malignant Pleural Mesothelioma. Ann Oncol. 2022;33(12):1282–1293.
- 13. Haegens A, van der Vliet A, Butnor KJ, et al. Asbestos-induced lung inflammation and epithelial cell signalling. Am J Respir Cell Mol Biol. 2020;63(3):281–294.
- 14. Cummings KJ, Kreiss K. Occupational and environmental chronic beryllium disease. Curr Opin Allergy Clin Immunol. 2015;15(2):126–132.
- 15. WorkSafe Queensland. Coal Mine Workers' Health Scheme — Guideline. Brisbane: Queensland Government; 2023. Available from: www.worksafe.qld.gov.au.
- 16. National Aboriginal Community Controlled Health Organisation (NACCHO). National Aboriginal and Torres Strait Islander Health Plan 2021–2031. Canberra: Australian Government Department of Health; 2021.
- 17. Australian Government Department of Health and Aged Care. National Strategic Plan for Asbestos Awareness and Management 2019–2023. Canberra: Commonwealth of Australia; 2019.
- 18. Hnizdo E, Vallyathan V. Chronic obstructive pulmonary disease due to occupational exposure to silica dust: a review of epidemiological and pathological evidence. Occup Environ Med. 2003;60(4):237–243.
- 19. Respiratory physicians and occupational physicians — Thoracic Society of Australia and New Zealand (TSANZ). Position Statement on Silicosis and Engineered Stone. Sydney: TSANZ; 2023.
- 20. Blanc PD, Annesi-Maesano I, Balmes JR, et al. The occupational burden of nonmalignant respiratory diseases: an official American Thoracic Society and European Respiratory Society statement. Am J Respir Crit Care Med. 2019;199(11):1312–1334.