📋 Key Information Summary
- NIV (CPAP or BiPAP) reduces intubation rates, ICU length of stay and mortality in acute hypercapnic COPD exacerbations (NNT 10) and cardiogenic pulmonary oedema.
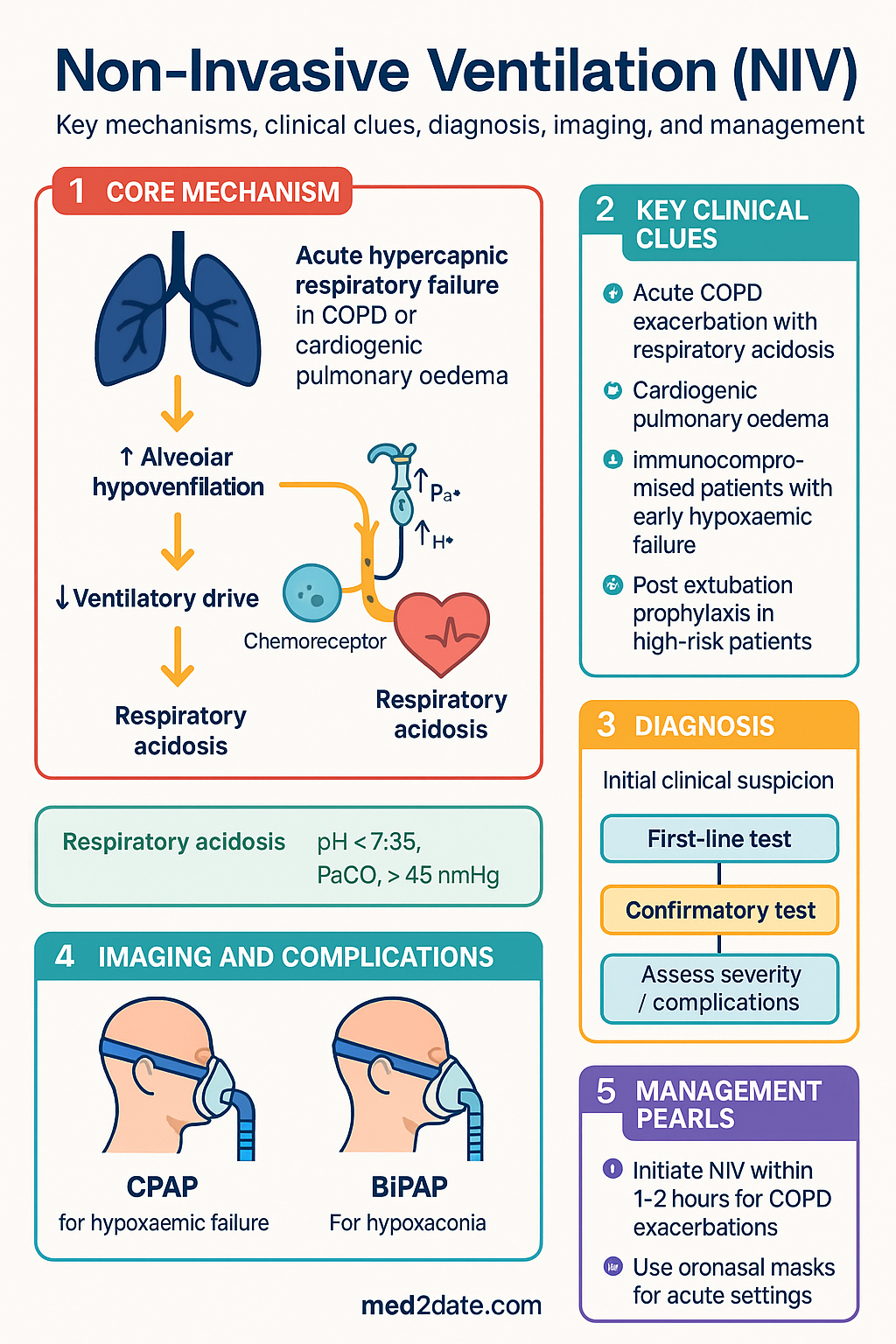
- Acute exacerbation of COPD with respiratory acidosis (pH <7.35, PaCO₂ >45 mmHg) is the strongest evidence-based indication for acute BiPAP — initiate within the first 1–2 hours.
- Cardiogenic pulmonary oedema responds rapidly to CPAP (5–10 cmH₂O); BiPAP (IPAP 10–15 / EPAP 5 cmH₂O) is an alternative, particularly if hypercapnia is present.
- CPAP vs BiPAP selection: use CPAP for pure hypoxaemic failure and obstructive sleep apnoea; use BiPAP when hypercapnia, work of breathing reduction, or ventilatory assist is needed.
- Interface choice matters: oronasal (full-face) masks are first-line for acute respiratory failure; nasal masks for chronic/home NIV; helmet interfaces are emerging but not standard in most Australian ICUs.
- NIV failure occurs in 20–40% of acute cases — reassess at 1–2 hours; rising PaCO₂, worsening pH (<7.25), haemodynamic instability, or inability to clear secretions mandate escalation to invasive ventilation.
- Contraindications to NIV: cardiac/respiratory arrest, inability to protect airway, life-threatening hypoxaemia, undrained pneumothorax, severe upper-GI bleeding, facial trauma, and patient refusal or non-compliance.
- Post-extubation NIV prophylaxis reduces reintubation in high-risk patients (age >65, COPD, cardiac failure, failed spontaneous breathing trial) — apply within 24–48 hours of extubation.
- Chronic home NIV is indicated for obesity hypoventilation syndrome (OHS), neuromuscular diseases (MND, DMD), and stable hypercapnic COPD (PaCO₂ ≥50 mmHg after acute admission) — improves survival and quality of life.
- Immunocompromised patients (haematological malignancy, post-transplant) with early hypoxaemic respiratory failure benefit from early NIV to avoid intubation-related infectious complications.
- Aboriginal and Torres Strait Islander Australians have higher COPD burden, later presentation, and greater barriers to home NIV access — culturally safe pathways and remote monitoring are essential.
- Monitor for NIV complications: mask discomfort, skin breakdown, gastric distension, aspiration risk, and patient-ventilator asynchrony — titrate pressures gradually and involve respiratory physiotherapy early.
Introduction & Australian Epidemiology
Non-invasive ventilation (NIV) delivers ventilatory support through a non-endotracheal interface — most commonly a nasal mask, oronasal mask, or nasal pillows — using either continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BiPAP). NIV has become a cornerstone of acute and chronic respiratory management across Australian emergency departments, respiratory wards, and intensive care units.
In Australia, COPD accounts for over 700,000 hospital bed-days annually and is the fifth leading cause of death. Approximately 20–30% of acute COPD exacerbations presenting to Australian EDs meet criteria for acute NIV. The Australian Institute of Health and Welfare (AIHW) reports that chronic lower respiratory diseases, predominantly COPD, caused 8,500 deaths in 2022, with Aboriginal and Torres Strait Islander Australians experiencing rates 2.5 times higher than non-Indigenous Australians.
Cardiogenic pulmonary oedema is the second most common acute NIV indication in Australian hospitals, with over 60,000 heart failure-related admissions per year. The National Stroke Foundation and Australian Resuscitation Council guidelines also endorse NIV in selected post-extubation and immunocompromised populations.
For chronic home NIV, the number of Australians on long-term ventilatory support has grown substantially over the past decade, driven by increased recognition of obesity hypoventilation syndrome (OHS) — estimated to affect 0.4–1.0% of the adult population — and improved survival in neuromuscular diseases such as motor neurone disease (MND) and Duchenne muscular dystrophy (DMD).
Indications for Acute NIV
NIV should be considered in any patient with acute or acute-on-chronic respiratory failure where the underlying cause is potentially reversible and the patient can cooperate, protect their airway, and tolerate the interface. The following are the principal evidence-based indications.
Acute Exacerbation of COPD (AECOPD)
Acute hypercapnic respiratory failure secondary to AECOPD is the single strongest indication for NIV. The landmark Cochrane review and subsequent meta-analyses confirm that BiPAP reduces the need for endotracheal intubation (RR 0.48), in-hospital mortality (RR 0.41), and treatment failure compared with standard medical therapy alone.
Initiation criteria (eTG Respiratory 2024):
- Respiratory acidosis: pH <7.35 with PaCO₂ >45 mmHg (6.0 kPa) despite maximal medical therapy (controlled oxygen, nebulised bronchodicoptors, systemic corticosteroids ± antibiotics)
- Severe dyspnoea with clinical signs of respiratory muscle fatigue (accessory muscle use, paradoxical abdominal movement, respiratory rate >25/min)
- Persistent hypoxaemia despite controlled oxygen therapy (target SpO₂ 88–92% in COPD)
Recommended settings:
| Parameter | Initial Setting | Titration Target |
|---|---|---|
| Mode | BiPAP (S/T mode) | — |
| EPAP (PEEP) | 4–5 cmH₂O | 4–6 cmH₂O (maintain to prevent atelectasis) |
| IPAP | 10–12 cmH₂O | Titrate by 2 cmH₂O every 15 min to 20–25 cmH₂O; target tidal volume 6–8 mL/kg |
| Backup rate | 12–14 breaths/min | Match patient's baseline rate or slightly below |
| FiO₂ | Titrate to SpO₂ 88–92% | Avoid high-flow uncontrolled O₂ in hypercapnic patients |
Cardiogenic Pulmonary Oedema (CPO)
NIV is highly effective in acute cardiogenic pulmonary oedema, reducing intubation rates and improving oxygenation within 1–2 hours. Both CPAP and BiPAP are supported by Level I evidence (3CPO trial, Cochrane review).
- CPAP (5–10 cmH₂O via tight-fitting oronasal mask) is first-line for CPO in most Australian EDs — simple, effective, and lower risk of gastric distension
- BiPAP (IPAP 10–15 cmH₂O, EPAP 5 cmH₂O) is preferred when concurrent hypercapnia (PaCO₂ >45 mmHg) is present or when CPAP alone fails to improve dyspnoea within 30–60 minutes
- Adjunctive therapy: IV frusemide 40–80 mg (or bumetanide 1–2 mg if frusemide allergy), sublingual or IV GTN, and urgent cardiology review for underlying cause (ACS, arrhythmia, valvular disease)
Immunocompromised Patients
Patients with haematological malignancies, solid organ transplant recipients, those receiving chemotherapy, and other immunocompromised states are at high risk of respiratory failure from opportunistic infections, drug-induced pneumonitis, and diffuse alveolar haemorrhage. NIV plays a critical role in avoiding intubation, which carries a mortality rate of 40–70% in this cohort.
- Early initiation in the ED or respiratory high-dependency unit for SpO₂ <90% on supplemental O₂ and respiratory rate >30/min
- CPAP or BiPAP depending on presence of hypercapnia — BiPAP preferred if PaCO₂ elevated
- Close monitoring for NIV failure is essential — immunocompromised patients who fail NIV have very high mortality; early escalation to invasive ventilation or ICU referral should be considered within 1–2 hours if no improvement
- Non-invasive high-flow nasal oxygen (HFNO, 30–60 L/min) is a complementary strategy, particularly for hypoxaemic respiratory failure without hypercapnia — available in most Australian tertiary ICUs
Post-Extubation NIV Prophylaxis
Prophylactic NIV applied after planned extubation reduces the rate of reintubation in patients at high risk of post-extubation respiratory failure. This is distinct from rescue NIV for post-extubation respiratory failure, where evidence is less robust.
High-risk criteria for post-extubation NIV:
- Age >65 years
- Underlying COPD or chronic respiratory disease
- Heart failure (LVEF <45%)
- APACHE II score >12 on day of extubation
- Body mass index (BMI) >30 kg/m²
- Failed first spontaneous breathing trial or multiple weaning attempts
- Hypercapnia during spontaneous breathing trial (PaCO₂ >45 mmHg)
- Upper airway stridor post-extubation (corticosteroids + NIV/CPAP)
Application: Initiate BiPAP (IPAP 12–15 cmH₂O / EPAP 5 cmH₂O) or CPAP (5–10 cmH₂O) within 24–48 hours post-extubation, applied for a minimum of 12–24 hours. The SuN-ICU trial (JAMA 2022) demonstrated that post-extubation high-flow nasal oxygen is non-inferior to NIV for preventing reintubation; however, NIV remains preferred in hypercapnic patients.
CPAP vs BiPAP — Mode Selection and Management
Mode Selection
| Feature | CPAP | BiPAP (Bilevel) |
|---|---|---|
| Mechanism | Continuous positive airway pressure — single fixed pressure throughout respiratory cycle | Two pressures: inspiratory (IPAP) and expiratory (EPAP) — pressure support = IPAP − EPAP |
| Primary effect | Stent upper airway, recruit alveoli, improve oxygenation, reduce preload/afterload | Reduces work of breathing, augments tidal volume, reduces PaCO₂ |
| Best for | Cardiogenic pulmonary oedema, OSA, post-extubation prophylaxis (normocapnic), hypoxaemic respiratory failure | Acute COPD exacerbation with hypercapnia, neuromuscular disease, OHS, chest wall deformity |
| Typical pressures | 5–15 cmH₂O (most commonly 7.5–10 cmH₂O) | IPAP 10–25 cmH₂O, EPAP 4–8 cmH₂O |
| Backup rate | Not applicable (patient triggers all breaths) | 10–16 breaths/min (S/T mode) |
| CO₂ clearance | Minimal — does not directly assist ventilation | Effective — higher pressure support increases minute ventilation |
Pressure Settings and Titration
Pressure settings should be individualised based on the clinical indication, patient tolerance, and physiological response. The goal is to achieve adequate tidal volumes (6–8 mL/kg ideal body weight), reduce respiratory rate (<25/min), and improve pH and PaCO₂ within 1–2 hours.
Interface Choice
The interface is a critical determinant of NIV success. A poorly fitting mask leads to air leak, patient discomfort, reduced efficacy, and treatment failure.
| Interface | Indication | Advantages | Disadvantages |
|---|---|---|---|
| Oronasal (full-face) mask | Acute respiratory failure (first-line) | Reduces mouth leak, better for mouth breathers, more effective at higher pressures | Claustrophobia, skin breakdown (nasal bridge), aspiration risk, vomiting |
| Nasal mask | Chronic/home NIV, OSA | Better tolerated long-term, less claustrophobic, can eat/drink/speak | Mouth leak at higher pressures, less effective in acute settings |
| Nasal pillows | Chronic home NIV (mild disease) | Minimal facial contact, no skin breakdown, comfortable | Limited to lower pressures (<15 cmH₂O), nasal irritation, epistaxis |
| Total-face mask | Patients with facial skin breakdown or unable to tolerate oronasal mask | Avoids pressure on nasal bridge, distributes contact pressure | Less available, high dead space, claustrophobia |
| Helmet | Prolonged NIV in ICU (emerging evidence) | No skin breakdown, can communicate, very well tolerated | High cost, limited availability in Australia, patient-ventilator asynchrony, CO₂ rebreathing risk |
Monitoring for NIV Success and Failure
Close monitoring in the first 1–2 hours is the single most important determinant of NIV outcomes. All patients on acute NIV require continuous pulse oximetry, regular vital sign assessment, and ABG monitoring.
Signs of NIV success (continue and wean):
- Decrease in respiratory rate (target <25/min within 1–2 hours)
- Improvement in pH (>7.30) and PaCO₂ (falling trend) on ABG at 1–2 hours
- Improved SpO₂ on target FiO₂ (88–92% for COPD; >94% for CPO)
- Reduced accessory muscle use, improved patient comfort, ability to speak in sentences
- Haemodynamic stability (HR <110, MAP >65 mmHg)
Signs of NIV failure (see NIV Failure section):
- Persistent or worsening tachypnoea (RR >30/min after 2 hours)
- Declining pH (<7.25) or rising PaCO₂ despite optimised settings
- Worsening oxygenation (SpO₂ <88% despite FiO₂ >0.6)
- Haemodynamic instability, altered consciousness (GCS <13), respiratory arrest
NIV Failure — Recognition and Escalation
NIV failure — defined as the need for endotracheal intubation and invasive mechanical ventilation despite NIV — occurs in approximately 20–40% of patients commenced on acute NIV. Early recognition of NIV failure is critical because delayed intubation is associated with significantly increased mortality (OR 2.0–4.0 in observational studies).
Criteria for Intubation — NIV Failure
The following criteria (adapted from BTS/ICS and TSANZ guidelines) should prompt immediate escalation to invasive ventilation. These should be assessed within 1–2 hours of NIV initiation and at regular intervals thereafter:
| Domain | NIV Failure Criterion |
|---|---|
| Gas exchange | pH <7.25 despite 1–2 hours of optimised NIV; or rising PaCO₂ with no improvement in pH |
| Oxygenation | PaO₂ <60 mmHg (8.0 kPa) or SpO₂ <88% despite FiO₂ ≥0.6 and EPAP ≥8 cmH₂O |
| Respiratory mechanics | Respiratory rate >30/min (or increasing) after 2 hours; paradoxical breathing; accessory muscle fatigue with inability to generate effective cough |
| Neurological | GCS ≤12 (or decline of ≥2 points); agitation requiring sedation that compromises respiratory drive; loss of airway reflexes |
| Haemodynamic | Systolic BP <90 mmHg requiring vasopressors; new or worsening arrhythmia; cardiac arrest |
| Secretion management | Inability to clear secretions despite physiotherapy; large-volume purulent secretions; risk of aspiration |
| Patient tolerance | Persistent mask intolerance, claustrophobia, or refusal to continue NIV despite adequate explanation and interface changes |
Early Recognition — Red Flags
Contraindications to NIV
NIV is contraindicated or relatively contraindicated in the following circumstances. In these situations, proceed directly to invasive mechanical ventilation or alternative management:
- Cardiac or respiratory arrest
- Inability to protect the airway (impaired cough reflex, excessive secretions, reduced GCS <8)
- Life-threatening hypoxaemia (PaO₂ <40 mmHg / 5.3 kPa on high-flow O₂)
- Undrained pneumothorax
- Massive haemoptysis
- Severe upper gastrointestinal bleeding with aspiration risk
- Facial trauma/burns precluding mask application
- Recent upper airway or oesophageal surgery
- Patient refusal or inability to cooperate despite maximal anxiolysis
- Haemodynamic instability (MAP <65 mmHg, requiring vasopressors)
- Inability to clear secretions (chronic bronchiectasis, neuromuscular weakness with ineffective cough)
- Extreme agitation or delirium (risk of mask removal, aspiration)
- Bowel obstruction (risk of gastric distension and aspiration with positive pressure)
- Pneumomediastinum or pneumothorax (drained) — use low pressures with caution
- Morbid obesity (BMI >50 kg/m²) — may require very high pressures; specialist NIV titration recommended
Chronic (Home) NIV
Long-term home NIV is an established treatment for chronic hypercapnic respiratory failure. In Australia, home NIV programmes are coordinated through state-based respiratory services (e.g., Austin Health Home Mechanical Ventilation Programme, Royal Prince Alfred Hospital HMV service, Westmead Hospital HMV Clinic, and equivalent services in other states). Access to home NIV requires specialist respiratory/sleep physician assessment, overnight oximetry and/or transcutaneous CO₂ monitoring, and titration polysomnography or respiratory polygraphy.
Obesity Hypoventilation Syndrome (OHS)
OHS is defined by the triad of obesity (BMI ≥30 kg/m²), chronic daytime hypercapnia (PaCO₂ ≥45 mmHg / 6.0 kPa), and sleep-disordered breathing, after exclusion of other causes of hypoventilation. It is estimated to affect 0.4–1.0% of obese adults but remains significantly underdiagnosed in Australia. Untreated OHS carries a mortality rate of 23% at 18 months and a five-fold increase in cardiovascular events compared with BMI-matched controls.
Treatment:
- First-line: CPAP for OHS with concurrent severe OSA (AHI ≥30) — effective in approximately 50–70% of patients. If persistent hypercapnia or symptoms on CPAP, switch to BiPAP.
- BiPAP (S/T mode): IPAP 12–20 cmH₂O, EPAP 6–10 cmH₂O, backup rate 14–16/min. Titrate to normalise PaCO₂ (<45 mmHg) during sleep. Preferred for OHS without significant OSA or with persistent hypercapnia on CPAP.
- Weight loss is essential adjunctive therapy — target ≥5–10% body weight loss. Refer to a multidisciplinary bariatric programme. Some patients can be weaned from NIV after significant weight loss.
- Comorbidities: Screen for and treat type 2 diabetes, hypertension, pulmonary hypertension, and obstructive sleep apnoea concurrently.
Neuromuscular Disease
Chronic NIV is the standard of care for respiratory failure in progressive neuromuscular diseases, particularly motor neurone disease (MND/ALS), Duchenne muscular dystrophy (DMD), myotonic dystrophy, and other muscular dystrophies. NIV improves quality of life, reduces hospitalisations, and extends survival in MND by a median of 7–13 months (Bourke et al., Lancet Neurology 2006).
- Initiation criteria: Symptoms of nocturnal hypoventilation (morning headache, excessive daytime somnolence, disturbed sleep) PLUS one of: FVC <80% predicted, sniff nasal inspiratory pressure (SNIP) <70 cmH₂O, overnight oximetry showing >10% time with SpO₂ <90%, or daytime PaCO₂ >45 mmHg
- Mode: BiPAP (S/T) is preferred — IPAP 10–20 cmH₂O, EPAP 4–6 cmH₂O, backup rate 12–16/min. Start with nocturnal use and extend to daytime as disease progresses.
- Interface: Nasal mask first-line for chronic use. Switch to oronasal mask when significant mouth leak occurs. Consider mouthpiece ventilation in advanced MND for daytime use.
- Cough augmentation: Mechanical insufflation-exsufflation (MI-E, e.g., CoughAssist™) is recommended for patients with peak cough flow <270 L/min. Available through State-based neuromuscular clinics (e.g., MND clinics at Royal Melbourne, Westmead).
- Advanced care planning: Early and ongoing discussion of NIV goals, disease progression, transition to invasive ventilation (tracheostomy), and end-of-life preferences — aligned with MND Australia guidelines.
Stable Hypercapnic COPD
The role of chronic NIV in stable hypercapnic COPD has evolved significantly following the HOT-HMV trial (Lancet Respiratory Medicine 2017) and subsequent studies. Current evidence supports home NIV in patients with persistent hypercapnia (PaCO₂ ≥53 mmHg / 7.0 kPa) after acute exacerbation, particularly when hypercapnia persists after resolution of the acute illness (typically assessed 2–4 weeks post-discharge).
- Indication: Persistent daytime hypercapnia (PaCO₂ ≥53 mmHg) or nocturnal hypercapnia (transcutaneous CO₂ >50 mmHg overnight) after resolution of acute exacerbation, despite optimal medical therapy (LAMA/LABA ± ICS, pulmonary rehabilitation, long-term oxygen therapy if indicated)
- Mode: BiPAP (S/T) — high-intensity NIV targeting normalisation of PaCO₂ (≤45 mmHg). IPAP typically 16–25 cmH₂O, EPAP 4–6 cmH₂O, backup rate 16–20/min
- Evidence: The HOT-HMV trial demonstrated improved event-free survival (hazard ratio 0.49) and reduced hospital readmissions at 12 months when home NIV was added to long-term oxygen therapy in persistent hypercapnic COPD patients
- Monitoring: Repeat ABG or transcutaneous CO₂ at 4–6 weeks, then 3-monthly for the first year. Adjust ventilator settings to maintain PaCO₂ <45 mmHg during sleep.
Investigations
Investigations serve three purposes in NIV management: confirming the indication, monitoring response, and identifying complications. The following are recommended for patients being considered for or commenced on NIV.
Special Populations
Pregnancy
Paediatrics
Elderly
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians bear a disproportionate burden of chronic respiratory disease, including COPD (2.5 times the non-Indigenous rate), bronchiectasis, and rheumatic heart disease leading to cardiogenic pulmonary oedema. These factors increase the likelihood that Indigenous Australians will require NIV — yet access barriers remain significant, particularly in remote communities.
📚 References
- 1. Osadnik CR, Tee VS, Carson-Chahhoud KV, et al. Non-invasive ventilation for the management of acute hypercapnic respiratory failure due to exacerbation of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017;7(7):CD004104.
- 2. Vital FM, Ladeira MT, Atallah AN. Non-invasive positive pressure ventilation (CPAP or bilevel NPPV) for cardiogenic pulmonary oedema. Cochrane Database Syst Rev. 2013;(5):CD005351.
- 3. Gray A, Goodacre S, Newby DE, et al. Noninvasive ventilation in acute cardiogenic pulmonary edema. N Engl J Med. 2008;359(2):142–151.
- 4. Murphy PB, Rehal S, Arbane G, et al. Effect of home noninvasive ventilation with oxygen therapy vs oxygen therapy alone on hospital readmission or death after an acute COPD exacerbation: a randomized clinical trial. JAMA. 2017;317(21):2177–2186.
- 5. Bourke SC, Tomlinson M, Williams TL, et al. Effects of non-invasive ventilation on survival and quality of life in patients with amyotrophic lateral sclerosis: a randomised controlled trial. Lancet Neurol. 2006;5(2):140–147.
- 6. Esteban A, Frutos-Vivar F, Ferguson ND, et al. Noninvasive positive-pressure ventilation for respiratory failure after extubation. N Engl J Med. 2004;350(24):2452–2460.
- 7. Delclaux C, L'Her E, Alberti C, et al. Treatment of acute hypoxemic nonhypercapnic respiratory insufficiency with continuous positive airway pressure delivered by a face mask: a randomized controlled trial. JAMA. 2000;284(18):2352–2360.
- 8. Stefan MS, Hill NS, Fisher KA, et al. National patterns of noninvasive ventilation use in the intensive care unit: analysis of a national database. Crit Care Med. 2020;48(7):e594–e601.
- 9. Masa JF, Corral J, Alonso ML, et al. Effectiveness of treatment with non-invasive ventilation in obesity hypoventilation syndrome: a multicentre randomised controlled trial (Pickwick study). Lancet Respir Med. 2015;3(11):867–876.
- 10. Australian Institute of Health and Welfare. Chronic respiratory diseases in Australia. AIHW Cat. No. ACM 36. Canberra: AIHW; 2023.
- 11. Davidson AC, Banham S, Elliott M, et al. BTS/ICS guideline for the ventilatory management of acute hypercapnic respiratory failure in adults. Thorax. 2016;71(Suppl 2):ii1–ii35.
- 12. Frat JP, Thille AW, Mercat A, et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med. 2015;372(23):2185–2196.
- 13. Australasian Sleep Association. Position paper: Home non-invasive ventilation in adults — a consensus statement. Respirology. 2019;24(5):417–430.
- 14. MND Australia. Clinical Practice Guidelines for Motor Neurone Disease: Respiratory Management. Sydney: MND Australia; 2020.