📋 Key Information Summary
- Nontuberculous mycobacteria (NTM) are environmental organisms found in soil and water; over 190 species identified, but only a minority cause clinically significant pulmonary disease in humans.
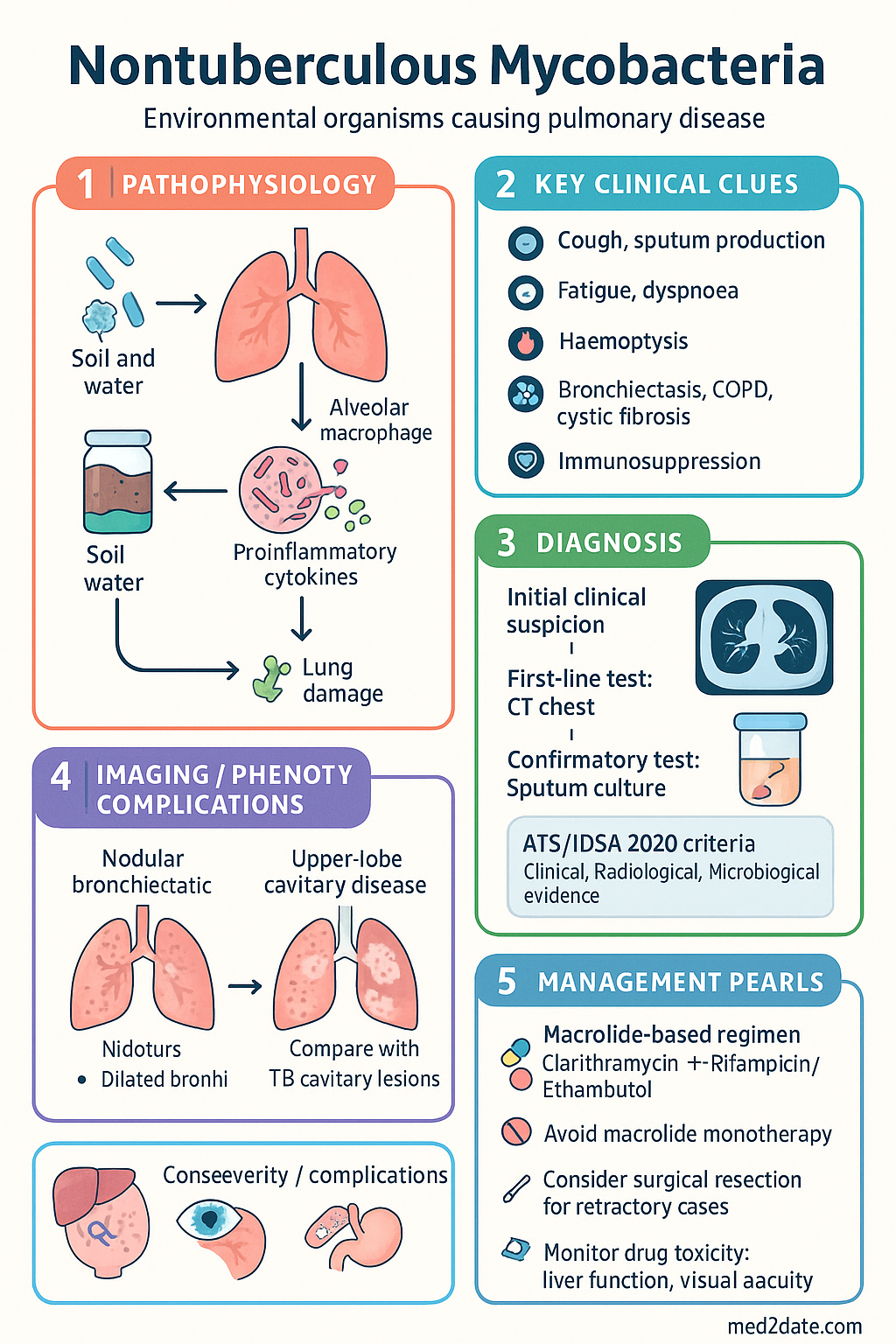
- The ATS/IDSA 2020 diagnostic criteria require clinical, radiological, AND microbiological evidence — a positive culture alone is insufficient for diagnosis.
- Mycobacterium avium complex (MAC) is the most common NTM species causing pulmonary disease in Australia, followed by M. abscessus complex and M. kansasii.
- Two major radiological phenotypes exist: nodular bronchiectatic (fibrocavitary) and upper-lobe cavitary disease — the phenotype guides treatment intensity and duration.
- MAC pulmonary disease is treated with a macrolide-based triple regimen: clarithromycin (or azithromycin) + rifampicin + ethambutol for a minimum of 12 months after sputum culture conversion.
- Macrolide monotherapy must be avoided in MAC to prevent acquired macrolide resistance, which dramatically worsens outcomes.
- Inhaled amikacin (Arikayce® liposomal) is PBS-listed (Authority Required) as add-on therapy for refractory MAC pulmonary disease in adults.
- M. abscessus pulmonary disease requires multidrug IV and oral therapy guided by species-level identification (M. abscessus subsp. abscessus vs massiliense vs bolletii) and susceptibility testing; macrolide susceptibility is critical.
- Surgical resection should be considered in localised NTM pulmonary disease (especially M. abscessus) that is refractory to medical therapy and in select MAC cavitary disease.
- Drug toxicity monitoring is essential: audiometry and vestibular assessment for amikacin, liver function for macrolides and rifampicin, visual acuity and colour vision for ethambutol, and renal function for aminoglycosides.
- Aboriginal and Torres Strait Islander Australians in remote communities may have higher exposure to environmental NTM; rheumatic heart disease-related bronchiectasis increases susceptibility to NTM infection.
- Recurrence rates after treatment completion are 20–50%; long-term sputum surveillance (at least 12 months post-treatment) is recommended.
Introduction & Australian Epidemiology
Nontuberculous mycobacteria (NTM) are ubiquitous environmental organisms found in natural and engineered water systems, soil, and aerosols. Unlike Mycobacterium tuberculosis, NTM are not transmitted person-to-person. Over 190 species have been identified, but relatively few cause clinically significant pulmonary disease. The most clinically relevant species in the Australian context are Mycobacterium avium complex (MAC), Mycobacterium abscessus complex, and Mycobacterium kansasii.
The incidence and prevalence of NTM pulmonary disease are increasing worldwide, including in Australia. Data from the NTM project and laboratory notifications suggest that NTM isolation rates in Australia have risen over the past two decades. Contributing factors include an ageing population, increasing prevalence of structural lung disease (particularly bronchiectasis), improved laboratory detection methods, and greater clinical awareness.
Australian Epidemiology
- MAC accounts for approximately 50–70% of NTM pulmonary isolates across major Australian centres.
- M. abscessus complex is the second most common pulmonary NTM and is the most challenging to treat due to intrinsic multidrug resistance.
- M. kansasii is less common in Australia than in parts of North America and Europe but remains an important cause of cavitary pulmonary disease.
- NTM disease is more common in patients with pre-existing bronchiectasis (including post-infectious bronchiectasis), chronic obstructive pulmonary disease (COPD), cystic fibrosis (CF), and immunosuppression.
- Hot-tub lung and hypersensitivity pneumonitis-like presentations from MAC in household water systems are increasingly recognised.
- Age-standardised NTM notification rates are highest in patients aged >60 years, with a female predominance (particularly for nodular bronchiectatic MAC disease).
- Aboriginal and Torres Strait Islander Australians may be disproportionately affected due to higher prevalence of bronchiectasis (often post-rheumatic fever), remote living conditions, and limited access to specialist respiratory services.
Diagnosis & Species
ATS/IDSA 2020 Diagnostic Criteria
Diagnosis of NTM pulmonary disease requires the integration of clinical, radiological, and microbiological criteria. A positive NTM culture alone is insufficient for diagnosis.
1. Clinical: Pulmonary symptoms (cough, sputum, fatigue, dyspnoea, haemoptysis) ± constitutional symptoms, OR radiological abnormalities.
2. Radiological: CT chest showing nodular or cavitary opacities, bronchiectasis with tree-in-bud nodules, or consolidation — not attributable to another cause.
3. Microbiological: ≥2 positive sputum cultures from separate specimens, OR ≥1 positive bronchoscopic wash/lavage culture, OR biopsy with histopathological features of mycobacterial disease with positive culture.
| Microbiological Criterion | Requirement | Notes |
|---|---|---|
| Sputum (expectorated or induced) | ≥2 positive cultures from separate specimens | At least 1 specimen should be an early-morning sample |
| Bronchoscopic wash or BAL | ≥1 positive culture | Useful when sputum is non-productive or results are equivocal |
| Lung biopsy | Positive culture + compatible histopathology (granulomatous inflammation or AFB) | Reserved for diagnostic uncertainty |
Key NTM Species in Australia
| Species / Complex | Clinical Significance | Typical Radiological Pattern | Culture Characteristics |
|---|---|---|---|
| MAC (M. avium complex) | Most common NTM pathogen; two phenotypes — nodular bronchiectatic (NB) and fibrocavitary (FC) | NB: right middle lobe/lingula tree-in-bud nodules with bronchiectasis FC: upper lobe cavitation with fibrosis |
Slow-growing; pigmented or non-pigmented colonies on LJ/MGIT; requires 2–6 weeks incubation |
| M. abscessus complex | Most treatment-resistant NTM; subdivided into subsp. abscessus, massiliense, bolletii | Bronchiectasis with nodules; cavitary disease in severe cases | Rapid-growing (visible within 7 days); scotochromogenic; species-level ID essential |
| M. kansasii | Second most common cause of NTM cavitary disease; typically responds well to treatment | Upper lobe cavitation mimicking TB; mass-like opacities | Slow-growing; photochromogenic (yellow pigment on light exposure); requires ≤14 days for visible growth on liquid media |
| M. xenopi | Thermophilic; associated with hot-water systems; causes cavitary disease in COPD patients | Upper lobe cavities; often indistinguishable from TB | Slow-growing; optimal growth at 42°C; pale yellow pigment |
Culture Confirmation & Susceptibility Testing
- Specimen collection: At least two early-morning sputum specimens on separate days. If the patient cannot expectorate, consider sputum induction (hypertonic saline) or bronchoscopy with BAL.
- Laboratory processing: Specimens should be decontaminated (N-acetyl-L-cysteine–sodium hydroxide [NALC-NaOH]) and inoculated onto both liquid (MGIT/BACTEC) and solid (Middlebrook 7H11 or Löwenstein-Jensen) media. Extended incubation (≥8 weeks for slow growers) is required.
- Species identification: Essential for guiding treatment. Matrix-assisted laser desorption/ionisation time-of-flight (MALDI-TOF) mass spectrometry is increasingly available in Australian laboratories. Molecular methods (16S rRNA gene sequencing, rpoB gene sequencing, hsp65 PCR-restriction enzyme analysis) provide definitive species-level identification.
- Susceptibility testing: Performed at reference laboratories (e.g., Victorian Infectious Diseases Reference Laboratory [VIDRL], Queensland Mycobacterial Reference Laboratory).
- MAC: Clarithromycin (critical — determines macrolide resistance status), amikacin, ethambutol, rifampicin, moxifloxacin, linezolid.
- M. abscessus complex: Clarithromycin (including 14-day extended incubation to detect erm(41)-inducible resistance in subsp. abscessus), amikacin, cefoxitin, imipenem, tigecycline, linezolid, clofazimine, bedaquiline.
- M. kansasii: Rifampicin (critical — rifampicin-susceptible M. kansasii responds well to standard TB-like regimen), isoniazid, ethambutol.
- Quality assurance: All NTM-positive cultures should be confirmed at a mycobacterial reference laboratory. Rapid-growing species require species-level identification (subspecies for M. abscessus complex) before treatment initiation.
MAC Pulmonary Disease — Treatment
Treatment of MAC pulmonary disease is guided by the radiological phenotype (nodular bronchiectatic vs fibrocavitary) and the presence of macrolide resistance. Macrolide-based combination therapy is the cornerstone of treatment, but regimen intensity and duration vary.
Nodular Bronchiectatic (NB) MAC Disease
The most common phenotype, particularly in older women with focal bronchiectasis (typically right middle lobe and lingula).
Recommended Regimens — Nodular Bronchiectatic Disease
Standard regimen (three-times-weekly):
- Clarithromycin 1000 mg PO three times per week (or azithromycin 500 mg PO three times per week) PLUS
- Rifampicin 600 mg PO three times per week PLUS
- Ethambutol 25 mg/kg PO three times per week
- Duration: Continue for a minimum of 12 months after sputum culture conversion (negative cultures from at least two separate specimens).
Daily regimen (alternative for more severe NB disease):
- Clarithromycin 500 mg PO BD (or azithromycin 250 mg PO daily) PLUS
- Rifampicin 450–600 mg PO daily PLUS
- Ethambutol 15 mg/kg PO daily
Fibrocavitary (FC) MAC Disease
Fibrocavitary disease carries a worse prognosis than NB disease and requires more aggressive treatment. Consider addition of an injectable aminoglycoside in the intensive phase.
- Clarithromycin 500–1000 mg PO daily PLUS
- Rifampicin 450–600 mg PO daily PLUS
- Ethambutol 15 mg/kg PO daily PLUS
- Amikacin 10–15 mg/kg IV/IM daily (or three times per week) during the initial 2–3 months, pending clinical and microbiological response.
- Consider substituting IV amikacin with inhaled amikacin (liposomal) once IV induction is complete.
Inhaled Amikacin (Liposomal)
Macrolide-Resistant MAC
Duration of Therapy
Treatment should continue for a minimum of 12 months after the first negative sputum culture. In practice, this means a total treatment duration of 15–24 months for most patients. Patients with fibrocavitary disease or macrolide-resistant MAC may require extended treatment (≥24 months). The decision to stop treatment should be based on achieving sustained sputum culture conversion (≥3 consecutive negative cultures over ≥3 months), resolution of symptoms, and radiological improvement or stability.
M. kansasii Pulmonary Disease
M. kansasii is generally more responsive to therapy than MAC. Rifampicin-susceptible M. kansasii is treated with a TB-like regimen:
- Rifampicin 600 mg PO daily PLUS
- Isoniazid 300 mg PO daily PLUS
- Ethambutol 15 mg/kg PO daily
- Duration: Continue for 12 months after sputum culture conversion (minimum total duration 12 months).
- Supplement with pyridoxine 25 mg PO daily to prevent isoniazid-related neuropathy.
Rifampicin-resistant M. kansasii should be treated in consultation with a mycobacterial specialist, considering moxifloxacin + ethambutol + isoniazid (if susceptible) + sulfamethoxazole-trimethoprim.
M. abscessus Complex — Management
Mycobacterium abscessus complex is the most treatment-resistant NTM species encountered in clinical practice. It comprises three subspecies — M. abscessus subsp. abscessus, M. abscessus subsp. massiliense, and M. abscessus subsp. bolletii — each with distinct macrolide resistance profiles that critically influence treatment outcomes.
Treatment Principles
- Multidrug IV induction therapy (typically ≥2–4 weeks, often extended to 2–3 months) followed by long-term oral/inhaled continuation therapy.
- Regimen selection is guided by subspecies identification, macrolide susceptibility, and drug susceptibility testing (DST) results.
- Treatment duration: minimum 12 months after sputum culture conversion, but many patients require ≥18–24 months total.
- Outcomes are poor: culture conversion rates are approximately 30–50% overall; better with subsp. massiliense.
- Early referral to a specialist mycobacterial centre is strongly recommended.
Standard Multidrug Regimen
Key Agents
Surgical Resection
Surgical resection should be considered in the following circumstances:
- Localised disease (e.g., single lobe or segment) refractory to ≥6 months of appropriate medical therapy.
- Persistent cavitary disease with ongoing positive sputum cultures despite optimised multidrug therapy.
- Massive haemoptysis requiring intervention.
- In combination with medical therapy — pre- and post-operative antimicrobial coverage reduces recurrence.
- Surgery should be performed by a thoracic surgeon experienced in NTM disease at a specialist centre, with adequate pulmonary reserve assessment (formal lung function testing with split-function studies).
Emerging Therapies for M. abscessus
- Bedaquiline: Case reports and small series suggest activity against M. abscessus in vitro; compassionate use in refractory disease. Accessed via Special Access Scheme.
- Omadacycline: Tetracycline-class agent with in vitro activity against M. abscessus; clinical data limited.
- Phage therapy: Experimental; individualised bacteriophage cocktails have shown promise in case reports; available through compassionate use pathways at select international centres.
Monitoring & Follow-up
Monitoring during NTM treatment encompasses three domains: (1) microbiological response — sputum culture conversion; (2) drug toxicity surveillance; and (3) clinical and radiological assessment. The duration and frequency of monitoring are long-term given the extended treatment courses required.
Sputum Culture Conversion
Drug Toxicity Monitoring
| Agent | Toxicity | Monitoring Parameter | Frequency |
|---|---|---|---|
| Ethambutol | Optic neuritis (dose- and duration-related) | Visual acuity + red-green colour discrimination (Ishihara plates) | Baseline; monthly for first 6 months; then every 3 months |
| Clarithromycin / Azithromycin | GI intolerance, QT prolongation, hepatotoxicity | LFTs, ECG (if risk factors for QT prolongation) | Baseline; 1 month; then every 3 months |
| Rifampicin | Hepatotoxicity, GI intolerance, orange discolouration, drug interactions | LFTs (ALT, ALP, bilirubin); INR if on warfarin | Baseline; 2 weeks; 1 month; then every 3 months |
| Amikacin (IV) | Nephrotoxicity, ototoxicity (cochlear + vestibular) | Serum creatinine/eGFR; trough levels; audiometry; vestibular function | Trough levels with every dose; creatinine twice weekly during IV; audiometry baseline + monthly |
| Amikacin (inhaled) | Dysphonia, cough, bronchospasm, potential ototoxicity | Audiometry; respiratory symptoms; spirometry | Baseline; 3-monthly audiometry; spirometry at 3 months |
| Linezolid | Myelosuppression, peripheral neuropathy, optic neuritis, lactic acidosis | FBC; visual acuity; peripheral nerve function | FBC fortnightly ×2 months, then monthly; visual acuity 3-monthly |
| Tigecycline | Nausea/vomiting, photosensitivity, coagulopathy | LFTs; coagulation studies; clinical tolerance | Baseline; weekly during IV therapy |
| Clofazimine | Skin discolouration, GI upset, QT prolongation | ECG (QTc); clinical assessment of skin changes; GI symptoms | Baseline ECG; 1 month; then every 3 months |
Treatment Duration Criteria
- Minimum treatment duration: 12 months after the first negative sputum culture (from ≥2 separate specimens).
- Culture conversion definition: Three consecutive negative cultures collected over ≥3 months, with no subsequent positive cultures during treatment.
- Extended treatment indications: Fibrocavitary disease, macrolide-resistant MAC, M. abscessus disease, immunosuppressed patients — these groups may require ≥24 months of total therapy.
- Treatment failure considerations: Persistently positive cultures after ≥6 months of appropriate therapy, clinical/radiological deterioration despite adherence, or emergence of new drug resistance. Consider regimen modification, surgical evaluation, or transition to suppressive therapy.
Recurrence Surveillance
Recurrence rates after completing treatment are significant (20–50% depending on species and phenotype). Long-term surveillance is essential:
- Sputum cultures every 3 months for the first 12 months post-treatment, then every 6 months for ≥2 years.
- CT chest at 6 and 12 months post-treatment, then annually for ≥2 years.
- Patients should be counselled to present early if new or worsening respiratory symptoms develop.
- Reinfection is common (particularly with MAC from the same environmental source) and must be differentiated from relapse by genotyping (if available) or comparison with pre-treatment isolate susceptibility profiles.
Special Populations
Pregnancy
Strategy: For stable NTM disease, consider deferring treatment until after delivery if clinically safe. If treatment is essential, use ethambutol + rifampicin + azithromycin (substituting for clarithromycin). Avoid aminoglycosides. Multidisciplinary planning with respiratory medicine, obstetrics, and infectious diseases is essential.
Paediatrics
Notes: NTM lymphadenitis (typically MAC or M. scrofulaceum) in children is managed primarily by surgical excision; antibiotics are reserved for incomplete excision or recurrence. Cervicofacial NTM lymphadenitis is self-limiting in many cases but surgical excision is preferred over incision and drainage.
Elderly
Notes: Elderly patients with nodular bronchiectatic MAC may be asymptomatic or minimally symptomatic. Treatment decisions should incorporate patient goals of care, comorbidities, and life expectancy. Observation with serial cultures may be appropriate in frail elderly patients with mild, indolent disease.
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Daley CL, Iaccarino JM, Lange C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA clinical practice guideline. Eur Respir J. 2020;56(1):2000535. doi:10.1183/13993003.00535-2020
- 2. Griffith DE, Aksamit T, Brown-Elliott BA, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367-416. doi:10.1164/rccm.200604-571ST
- 3. Thomson RM; NTM working group at Queen Elizabeth II Jubilee Hospital and The Prince Charles Hospital. Changing epidemiology of pulmonary nontuberculous mycobacteria infections. Emerg Infect Dis. 2010;16(10):1576-1583. doi:10.3201/eid1610.091201
- 4. Cowman S, van Ingen J, Griffith DE, Loebinger MR. Non-tuberculous mycobacterial pulmonary disease. Eur Respir J. 2019;54(1):1900250. doi:10.1183/13993003.00250-2019
- 5. Haworth CS, Banks J, Capstick T, et al. British Thoracic Society guidelines for the management of non-tuberculous mycobacterial pulmonary disease (NTM-PD). Thorax. 2017;72(Suppl 2):ii1-ii64. doi:10.1136/thoraxjnl-2017-210927
- 6. Koh WJ, Jeong BH, Kim SY, et al. Mycobacterial characteristics and treatment outcomes in Mycobacterium abscessus lung disease. Clin Infect Dis. 2017;64(3):309-316. doi:10.1093/cid/ciw724
- 7. Griffith DE, Eagle G, Thomson R, et al. Amikacin liposome inhalation suspension for treatment-refractory lung disease caused by Mycobacterium avium complex (CONVERT): a prospective, open-label, randomized study. Am J Respir Crit Care Med. 2018;198(12):1559-1569. doi:10.1164/rccm.201807-1318OC
- 8. Stout JE, Koh WJ, Yew WW. Update on pulmonary disease due to non-tuberculous mycobacteria. Int J Infect Dis. 2016;45:123-134. doi:10.1016/j.ijid.2016.03.006
- 9. Philley JV, Griffith DE. Treatment of nontuberculous mycobacterial pulmonary disease. Curr Top Microbiol Immunol. 2016;398:251-279. doi:10.1007/82_2016_502
- 10. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework — Respiratory diseases. Canberra: AIHW; 2023. Available at: https://www.aihw.gov.au/
- 11. Chang AB, Brown N, Toombs M, et al. Lung disease in Indigenous children. Paediatr Respir Rev. 2014;15(4):325-332. doi:10.1016/j.prrv.2014.04.011
- 12. Bryant JM, Grogono DM, Rodriguez-Rincon D, et al. Emergence and spread of a human-transmissible multidrug-resistant nontuberculous mycobacterium. Science. 2016;354(6313):751-757. doi:10.1126/science.aaf8156
- 13. Moon SM, Park HY, Kim SY, et al. Clinical characteristics, treatment outcomes, and resistance mutations associated with macrolide-resistant Mycobacterium avium complex lung disease. Antimicrob Agents Chemother. 2016;60(11):6758-6765. doi:10.1128/AAC.01240-16
- 14. Wassilew N, Hoffmann H, Andrejak C, Lange C. Pulmonary disease caused by non-tuberculous mycobacteria. Respiration. 2016;91(5):386-402. doi:10.1159/000445906
- 15. Dupont C, Joos L, Trachsel T, et al. Management of non-tuberculous mycobacterial lung disease — a practical approach. Swiss Med Wkly. 2023;153:40048. doi:10.4414/smw.2023.40048