📋 Key Information Summary
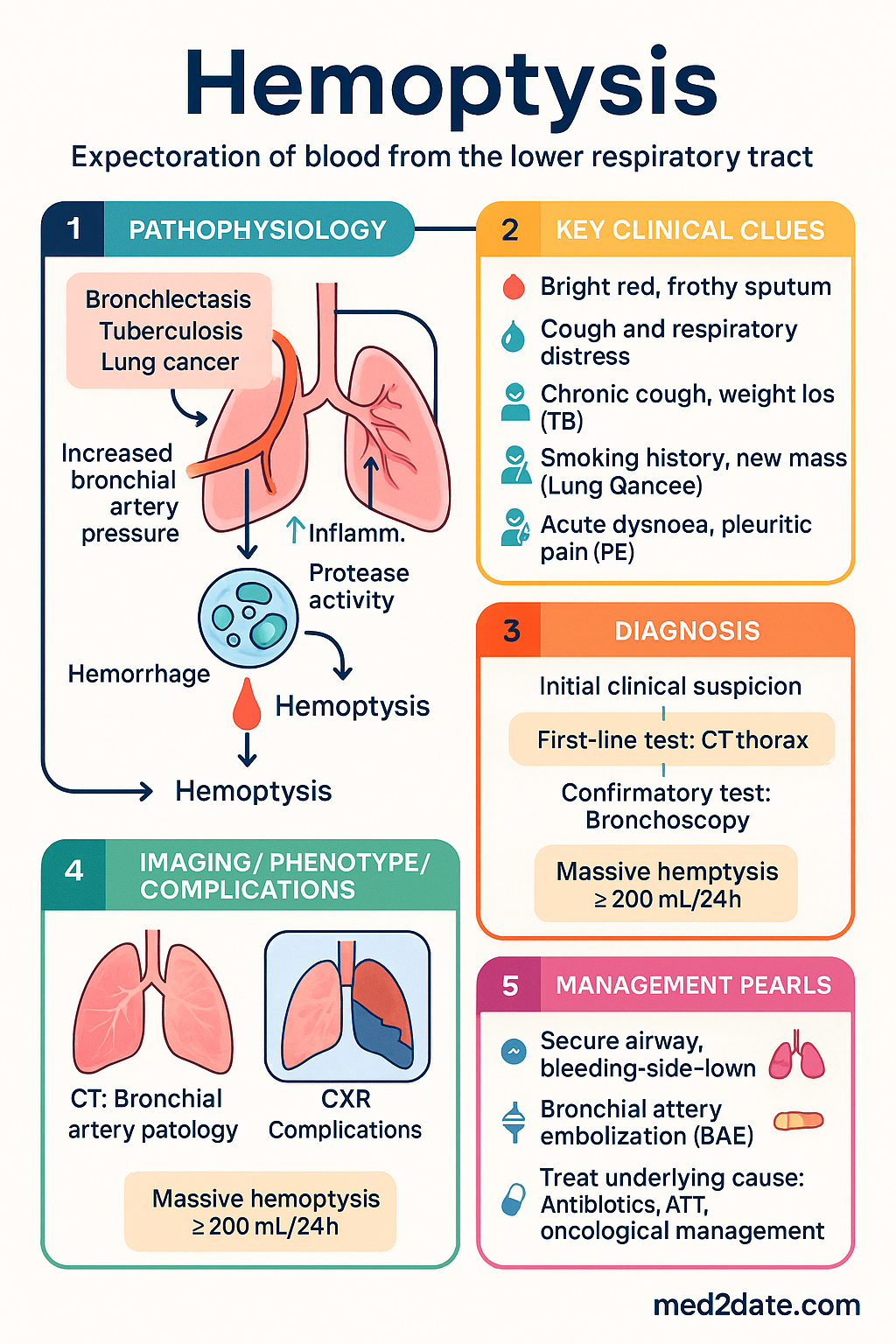
- Define hemoptysis clearly: expectoration of blood originating from the lower respiratory tract (below the glottis); always exclude pseudohemoptysis (upper GI, nasopharyngeal, or oropharyngeal sources) and hematemesis before initiating workup.
- Quantify the volume: massive hemoptysis is defined as ≥200 mL in 24 hours (some sources use ≥500–600 mL/24h); mortality rises sharply above 1,000 mL/24h and is driven by asphyxiation rather than exsanguination.
- Massive hemoptysis is a medical emergency: establish large-bore IV access, cross-match blood, position the patient bleeding-side-down, secure the airway (consider single-lumen ETT advanced to main bronchus of non-bleeding lung), and activate interventional radiology for bronchial artery embolization (BAE).
- Bronchiectasis is the leading cause in Australia, particularly in the setting of chronic lung disease, post-infectious damage, and cystic fibrosis; tuberculosis and lung malignancy are the next most common aetiologies.
- CT pulmonary angiography (CTPA) is the imaging modality of choice for suspected pulmonary embolism presenting with hemoptysis; contrast-enhanced CT of the thorax with arterial phase is preferred for identifying bronchial artery pathology and localising bleeding.
- Fibreoptic bronchoscopy is indicated for localising the bleeding source when CT is non-diagnostic, in recurrent hemoptysis, and when malignancy is suspected; perform during active bleeding when feasible or within 24–48 hours of cessation.
- Bronchial artery embolization (BAE) is the first-line treatment for massive and life-threatening hemoptysis, with immediate success rates of 70–90%; recurrence rates are 10–30% and are highest in aspergilloma and malignancy.
- Surgical resection is reserved for BAE failure or specific anatomical lesions (e.g., aspergilloma, localised bronchiectasis, cavitary lung disease) and carries operative mortality of 7–18% in emergency settings.
- Treat the underlying cause: antibiotics for pneumonia and bronchiectasis exacerbations, anti-tuberculosis therapy (ATT), oncological management for lung cancer, anticoagulation for PE, and immunosuppression for vasculitis.
- Tranexamic acid (TXA) — 1 g IV stat in massive hemoptysis, followed by 1 g IV over 8 hours; consider 500 mg–1 g TDS PO for non-massive hemoptysis while investigating (PBS Authority Required for oral form).
- Aboriginal and Torres Strait Islander Australians have disproportionately higher rates of bronchiectasis, tuberculosis, and rheumatic heart disease — all key causes of hemoptysis; remote access to bronchoscopy and embolization services remains a significant barrier.
- Red flags for immediate escalation: hemodynamic instability, massive bleeding (>200 mL/24h), respiratory compromise, anticoagulant or antiplatelet use, and suspected pulmonary embolism — all warrant emergent resuscitation and specialist consultation.
Introduction & Australian Epidemiology
Hemoptysis — the expectoration of blood or blood-streaked sputum originating from the lower respiratory tract — is a presenting symptom that ranges from self-limited and benign to life-threatening. It accounts for approximately 10–15% of pulmonary outpatient referrals and 5–15% of respiratory-related hospital admissions in Australia. While the majority of cases are caused by acute bronchitis or mild lower respiratory tract infections, clinicians must maintain a high index of suspicion for serious underlying pathology including bronchiectasis, tuberculosis (TB), lung cancer, and pulmonary embolism (PE).
In Australia, bronchiectasis — both cystic fibrosis (CF)-related and non-CF-related — is the single most common cause of significant hemoptysis, accounting for 20–30% of cases in published Australian series. Lung cancer and TB together account for a further 20–40%, with the relative proportions varying by geography and population. In remote and regional Aboriginal and Torres Strait Islander communities, post-infectious bronchiectasis and TB remain disproportionately prevalent, with notification rates of TB in Indigenous Australians approximately 1.5 times those of non-Indigenous Australians.
Massive hemoptysis — typically defined as ≥200 mL in 24 hours — carries a mortality of 50–100% without intervention, with death occurring primarily from asphyxiation rather than haemorrhagic shock. The availability of bronchial artery embolization (BAE) at major tertiary centres (including Royal Prince Alfred Hospital Sydney, The Alfred Melbourne, Royal Brisbane and Women's Hospital, and Sir Charles Gairdner Hospital Perth) has reduced in-hospital mortality from massive hemoptysis to 7–18%.
Assessment & Quantification
Initial Clinical Assessment
The initial approach to the patient presenting with hemoptysis must address three sequential questions: (1) Is this truly hemoptysis from the lower respiratory tract? (2) How much blood is being lost and is the patient physiologically stable? (3) What is the likely source and underlying cause?
Pseudohemoptysis vs True Hemoptysis
Before pursuing a respiratory investigation pathway, clinicians must exclude pseudohemoptysis — the expectoration of blood originating from a non-pulmonary source. Common mimics include:
- Hematemesis (upper GI bleeding): dark or coffee-ground vomitus, history of liver disease or peptic ulcer disease; the blood may be coughed up after vomiting (Boerhaave syndrome). Test: urea:creatinine ratio >100:1 favours GI origin.
- Nasopharyngeal bleeding (epistaxis): anterior rhinoscopy or ENT assessment reveals posterior nasal drip source; common in patients on anticoagulation or with hereditary haemorrhagic telangiectasia (HHT).
- Oropharyngeal bleeding: dental sources, tonsillar bleeding, or oral mucosal lesions; direct visualisation confirms the diagnosis.
Quantification: Massive vs Non-Massive
Quantification of hemoptysis volume is critical for triage and management decisions. While patient-reported volumes are often inaccurate (patients tend to overestimate), the following thresholds guide clinical urgency:
Localisation of Bleeding
Bleeding-side-down positioning is the immediate management priority. Where history and imaging are non-diagnostic, lateralisation can be guided by:
- Patient-reported side: unreliable alone (sensitivity ~50%), but should be documented.
- Chest X-ray (CXR): focal infiltrate, mass, cavity, or ground-glass opacity may localise the bleeding side; normal CXR in up to 30% of hemoptysis cases.
- CT thorax: highest yield for localisation (sensitivity 70–88%); arterial phase CT identifies hypertrophied bronchial arteries and active extravasation.
- Bronchoscopy: definitive localisation in 73–93% when performed during active bleeding; yield drops to 50% if performed >48 hours after cessation.
Aetiology
The aetiology of hemoptysis is broad and varies with population, geography, and comorbidity. In Australian published series, the following causes predominate. Importantly, up to 20–30% of cases remain idiopathic after comprehensive investigation — these patients generally have an excellent prognosis (<5% rate of serious pathology at 5-year follow-up).
| Cause | Approximate Frequency | Key Clinical Features | Australian Context |
|---|---|---|---|
| Bronchiectasis | 20–30% | Chronic productive cough, recurrent infections, clubbing, coarse crackles | Leading cause in Australia; non-CF bronchiectasis very common in Indigenous Australians and CF populations |
| Tuberculosis | 10–20% | Chronic cough, weight loss, night sweats, cavitary disease, immunosuppression | Higher rates in Indigenous communities, migrants from high-burden countries, immunocompromised; 1,300+ notifications/year nationally |
| Lung cancer | 10–20% | Age >50, smoking history, weight loss, chest pain, new mass on imaging | Leading cause of cancer death in Australia (~9,000 deaths/year); hemoptysis in ~20–30% of lung cancer patients at some point |
| Acute bronchitis / LRTI | 15–25% | Acute onset, self-limited, viral prodrome, mild blood-streaked sputum | Most common benign cause; usually managed in primary care |
| Pneumonia / lung abscess | 5–10% | Fever, purulent sputum, focal consolidation, pleuritic chest pain | Community-acquired or aspiration-related; CA-MRSA necrotising pneumonia may present with severe hemoptysis |
| Aspergilloma / chronic pulmonary aspergillosis | 5–10% | Pre-existing cavitary disease (TB, sarcoidosis), fungal ball on imaging | High risk of massive hemoptysis; recurrence after BAE is highest with aspergilloma |
| Pulmonary embolism | 3–5% | Acute dyspnoea, pleuritic chest pain, tachycardia, DVT risk factors | Must exclude in any patient with hemoptysis + dyspnoea; CTPA is essential |
| Vasculitis (GPA, MPA, Goodpasture's) | 1–3% | Hemoptysis + haematuria, raised inflammatory markers, positive ANCA/anti-GBM antibodies | Diffuse alveolar haemorrhage (DAH) is a rheumatological emergency requiring ICU admission and pulse IV methylprednisolone |
| Other (AVMs, coagulopathy, trauma, iatrogenic) | 5–10% | HHT (Osler-Weber-Rendu), anticoagulant use, post-bronchoscopy, post-transplant | Consider iatrogenic in post-procedural patients; coagulopathy (DOAC, warfarin, thrombocytopenia) amplifies any source |
| Idiopathic | 20–30% | Comprehensive investigation negative; usually minor or moderate volume | Excellent prognosis; recurrence risk <5% at 5 years; follow-up CXR recommended |
Bronchiectasis
Bronchiectasis — permanent abnormal dilatation of bronchi — is the single most common cause of hemoptysis in Australian practice. Haemoptysis occurs in 46–69% of patients with bronchiectasis at some point in their disease course, and is the presenting symptom in 15–20%. The mechanism involves hypertrophied, fragile bronchial arteries (systemic pressure) eroding into the airway lumen. In Australia, non-CF bronchiectasis is particularly prevalent in Aboriginal and Torres Strait Islander communities, where childhood respiratory infections (including adenovirus, pertussis, and measles, prior to widespread vaccination) have contributed to post-infectious bronchiectasis.
Tuberculosis
TB remains a significant cause of hemoptysis in Australia, particularly in high-risk groups including Aboriginal and Torres Strait Islander Australians, migrants and refugees from high-burden countries (sub-Saharan Africa, South-East Asia, the Indian subcontinent), people experiencing homelessness, and immunocompromised individuals (HIV, biologics, transplant). Active pulmonary TB with cavitary disease is the most common TB-related cause of hemoptysis; however, old TB scars may serve as the substrate for aspergilloma formation, which itself carries a high risk of massive hemoptysis.
Lung Cancer
Lung cancer accounts for 10–20% of hemoptysis presentations and is the most common malignancy to cause hemoptysis. Squamous cell carcinoma is the histological subtype most likely to cause hemoptysis due to its central airway location and propensity for cavitation. Any patient aged ≥40 years with unexplained hemoptysis and a smoking history should be investigated urgently for lung cancer. In Australia, the National Lung Cancer Screening Program (commencing July 2025) will use low-dose CT to detect early-stage disease, though hemoptysis itself warrants prompt investigation beyond screening pathways.
Pulmonary Embolism
PE presents with hemoptysis in 3–5% of cases, typically as small-volume blood-streaked sputum associated with acute dyspnoea and pleuritic chest pain. The mechanism is pulmonary infarction. PE must be actively excluded in any patient presenting with hemoptysis and concurrent respiratory symptoms, particularly when DVT risk factors are present. Failure to diagnose PE in a patient with hemoptysis is a critical safety event — CTPA should not be omitted due to concerns about contrast in the setting of active bleeding.
Vasculitis and Diffuse Alveolar Haemorrhage (DAH)
DAH represents a rheumatological emergency. It is characterised by the triad of hemoptysis, new bilateral alveolar infiltrates on CXR/CT, and a drop in haemoglobin. The most common causes are granulomatosis with polyangiitis (GPA, formerly Wegener's), microscopic polyangiitis (MPA), and anti-glomerular basement membrane disease (anti-GBM, Goodpasture's syndrome). Renal involvement (rapidly progressive glomerulonephritis) coexists in up to 60% of cases. Urgent serological testing (ANCA, anti-GBM, complement) and nephrology/rheumatology referral are essential. First-line treatment is pulse IV methylprednisolone 500–1,000 mg daily for 3 days, followed by cyclophosphamide and/or rituximab.
Diagnostic Evaluation
The diagnostic workup for hemoptysis should be guided by the severity of bleeding, the clinical context, and the pre-test probability of serious underlying pathology. In all cases, the investigation pathway should proceed in parallel with resuscitation — do not delay management for diagnostic certainty in massive hemoptysis.
Laboratory Investigations
Imaging
Bronchoscopy
Fibreoptic (flexible) bronchoscopy is the gold standard for localising bleeding within the airways and obtaining tissue for histological and microbiological analysis. Rigid bronchoscopy offers superior suctioning and airway control in massive hemoptysis and is preferred in tertiary centres with the expertise to perform it.
| Indication | Timing | Yield |
|---|---|---|
| Active hemoptysis (moderate–massive) | Emergent / within hours | 73–93% localisation |
| CT non-diagnostic | Within 48 hours of cessation | Additional pathology found in 10–30% |
| Suspected endobronchial malignancy | Urgent (within 2 weeks per lung cancer pathways) | Diagnostic in 60–85% of central tumours |
| Suspected TB (sputum AFB negative) | Within 1–2 weeks | Bronchial washings AFB positive in additional 10–20% |
| Recurrent hemoptysis, no cause found | Elective, within 4 weeks | Identifies cause in 30–40% of initially negative cases |
Bronchial Arteriography
Performed by interventional radiology, bronchial arteriography is both diagnostic and therapeutic (proceeding to embolization). It identifies hypertrophied and abnormal bronchial arteries, aberrant systemic arteries (from intercostal, subclavian, or internal mammary arteries), and active contrast extravasation. Available at all major Australian tertiary centres; patients in remote areas may require aeromedical retrieval (RFDS or equivalent).
Additional Investigations (as indicated)
- Sweat test / CFTR genetics: if bronchiectasis in a young patient without known CF.
- Immunoglobulins (IgG, IgA, IgM, IgG subclasses): if recurrent infections with bronchiectasis — assess for common variable immunodeficiency (CVID).
- Echocardiography: if mitral stenosis (rare but classic cause), pulmonary hypertension, or right heart dysfunction suspected.
- CT of sinuses: if GPA suspected (upper airway involvement is common).
- Renal biopsy: if ANCA-positive vasculitis with renal involvement (rapidly progressive glomerulonephritis).
Management
Emergency Management: Massive Hemoptysis
Massive hemoptysis (≥200 mL/24h or any hemoptysis with haemodynamic/respiratory compromise) is a medical emergency requiring a coordinated multidisciplinary approach involving respiratory medicine, interventional radiology, thoracic surgery, and intensive care.
Non-Massive Hemoptysis: Outpatient / Inpatient Workup
For minor and moderate hemoptysis without haemodynamic compromise, the approach is diagnostic rather than emergent:
- Stabilise and assess vital signs. Continuous pulse oximetry. Document estimated volume and character of hemoptysis.
- Perform CXR — first-line imaging in all cases.
- CT thorax with contrast — if CXR is abnormal, if risk factors for malignancy are present (age ≥40, smoking ≥20 pack-years), or if hemoptysis is recurrent.
- Sputum samples — AFB (3 early morning specimens), bacterial culture, cytology.
- Consider CTPA — if PE is in the differential (dyspnoea, pleuritic pain, DVT risk).
- Bronchoscopy — if CT is non-diagnostic, if malignancy is suspected, or if hemoptysis recurs after an initial negative workup.
- Tranexamic acid 500 mg–1 g PO TDS may be prescribed while awaiting investigation to reduce bleeding frequency (off-label use; discuss with the patient regarding potential risks of thrombosis).
Pharmacotherapy for Underlying Causes
Quick Reference: Common Scenarios
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Radchenko C, Alraiyes AH, Shojaee S. A systematic approach to the management of massive hemoptysis. J Thorac Dis. 2017;9(Suppl 10):S1069–S1086. doi:10.21037/jtd.2017.06.90
- 2. Sakr L, Dutau H. Massive hemoptysis: an update on the role of bronchoscopy in diagnosis and management. Respiration. 2010;80(1):38–58. doi:10.1159/000274492
- 3. Jean-Baptiste E. Clinical assessment and management of massive hemoptysis. Crit Care Med. 2000;28(5):1642–1647. doi:10.1097/00003246-200005000-00082
- 4. Chang YL, Lee YC. Massive hemoptysis: assessment and management. Semin Respir Crit Care Med. 2017;38(6):778–788.
- 5. Chang CC, Chen YJ, Lee YC. Bronchial artery embolisation for haemoptysis: a systematic review and meta-analysis. Eur Respir J. 2023;61(6):2201593.
- 6. Chang AB, Bell SC, Byrnes CA, et al. Chronic suppurative lung disease and bronchiectasis in children and adults in Australia and New Zealand. Med J Aust. 2010;193(1):356–365. doi:10.5694/j.1326-5377.2010.tb03588.x
- 7. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework: Detailed Analyses 2023. Canberra: AIHW; 2023.
- 8. Lung Foundation Australia. The Australian Bronchiectasis Handbook. 3rd ed. Brisbane: Lung Foundation Australia; 2023.
- 9. Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook. Australian Government Department of Health; 2024. [Accessed 2024].
- 10. Ruhl AP, Berhane K, Gillmeyer KR, et al. Hospitalization and mortality in hemoptysis: a systematic review and meta-analysis. Chest. 2020;158(6):2540–2551.
- 11. World Health Organization (WHO). Global Tuberculosis Report 2023. Geneva: WHO; 2023.
- 12. RHDAustralia (ARF/RHD writing group). The Australian Guideline for Prevention, Diagnosis and Management of Acute Rheumatic Fever and Rheumatic Heart Disease. 3rd ed. Darwin: RHDAustralia; 2020.
- 13. De Soyza A, Aksamit T, Bhatt SP, et al. Bronchiectasis research and medical network: a comprehensive review of bronchiectasis. Lancet Respir Med. 2023;11(2):188–202.
- 14. Krukonis ES, Grewal HK, Mehta AC. The role of interventional pulmonary in massive hemoptysis: a narrative review. J Thorac Dis. 2023;15(4):2276–2289.
- 15. Expert Group for Respiratory. Haemoptysis. In: Therapeutic Guidelines: Respiratory. Melbourne: Therapeutic Guidelines Limited; 2023. [Informing source — primary literature cited above].